
Abstract
When considering cases of infant head injury as a result of a short fall, investigators often have to base their opinions on the potential severity of a head injury on a scene description and/or photographic evidence of the potential impact surfaces. While variation in the attenuation properties of typical domestic surfaces and underlying support structures have been reported in the literature, this study investigates whether there is a need to consider the nature and composition of specific potential impact floor surfaces/sites, within a scene, prior to providing an opinion about the likely head impact injury outcome. An instrumented headform was impacted within a suspected crime scene to determine whether different potential impact sites posed different risks of producing head injury. The impact acceleration–time waveform, for the headform, was shown to vary considerably across the floor. By applying recognized head impact injury risk measures (peak g and head injury criterion), it was illustrated that the risk of an infant sustaining a significant head injury could vary considerably, depending upon the exact point of impact with the floor. This study highlights the potential for variation in impact force across a scene and illustrates the need to consider surface composition at specific sites across the entire potential impact area, since the risk of head injury can vary significantly. Caution should therefore be exercised when expressing opinions based solely on verbal, written or photographic evidence of head impact surfaces, without due consideration of the specific area onto which a head might have impacted.
Introduction
This study describes the case of a six-month-old infant who sustained a complex skull fracture and subdural haemorrhage as a result of an alleged short fall. The explanation provided by the infant's carer was that the injuries were sustained during a short fall, from arms, on or around a landing stair area. The infant was described as having jerked backwards and fallen, banging its head onto the floor. A written description of the scene and photographic evidence was provided (shown diagrammatically in Figure 1).
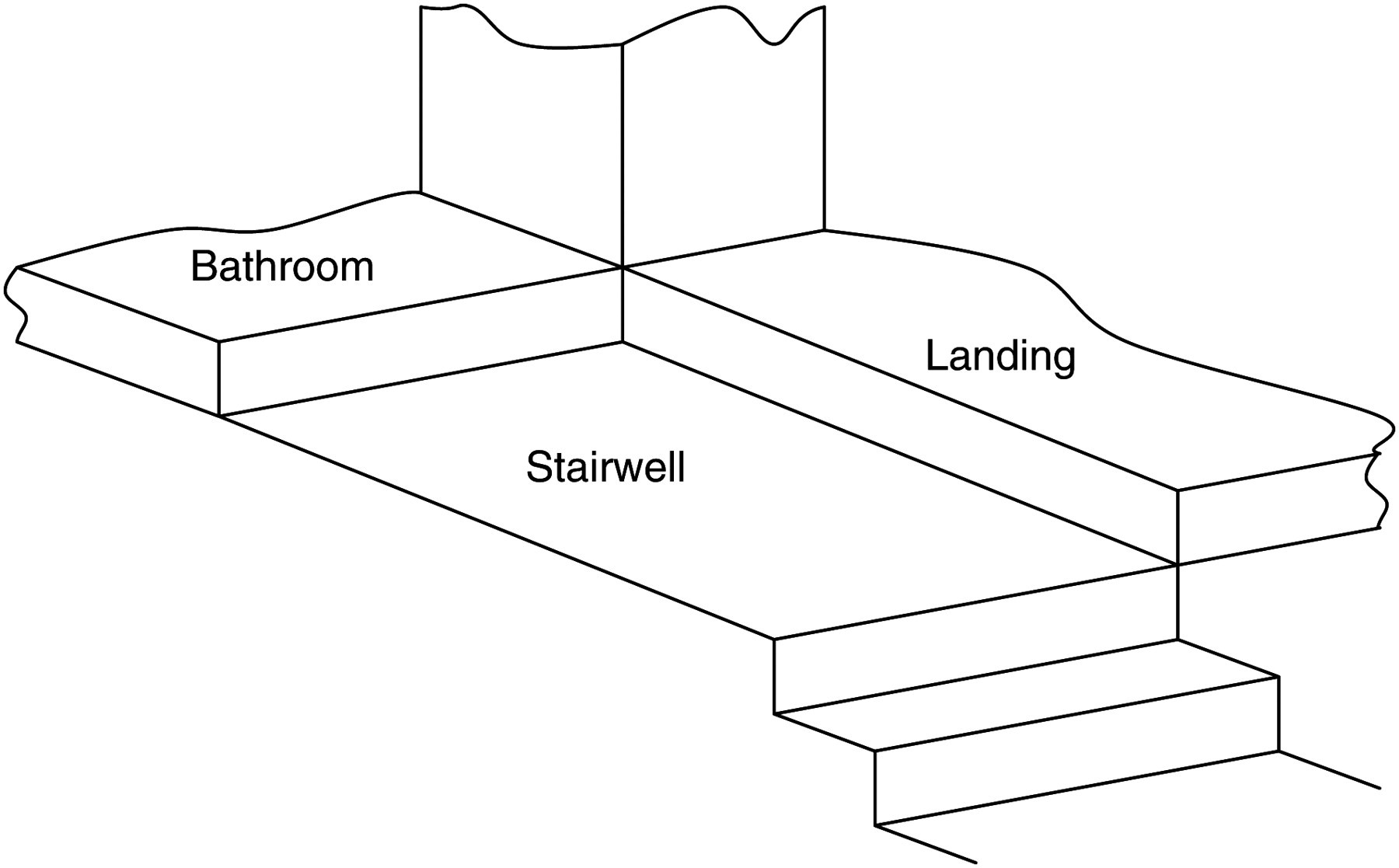
Schematic representation of scene
When considering such cases of infant head injury as a result of a short fall, previous studies have highlighted reliance on photographic evidence of the impact surface as a potential weakness. 1 The contact surface has previously been deemed more important than the fall height in determining the potential for injury, following impact, 2 while also reported is the importance of considering the combined impact attenuation properties of all component layers of the surface. 1 Subsequently, this study reports an in situ biomechanical analysis, utilizing a methodology developed by Cory and Jones, 1 applying an instrumented biofidelic headform to investigate the potential variation in risk of head injuries being sustained from short fall-related impacts across a scene.
Infants are commonly injured by a fall, with stairways being recognized as the most common cause of infant injury. 3 Of injuries from infants falling on stairways, 90% injure their head and 72% of these sustain a skull fracture; 4 this high incidence is thought to be probably due to their larger proportion of head mass and relatively poor co-ordination. 5
Experimentation has previously identified that freefall drops from a relatively low height (82 cm) onto commonly encountered domestic surfaces (stone, carpet and foam backed linoleum) are sufficient to cause skull fracture in infants. 6,7 Indeed, investigation has indicated that falls from heights as low as 30 cm onto hard surfaces are sufficient to exceed the safety reference value, 50g, associated with head injury; 7 however, no skull fractures were reported at this fall height. 8 These results, which feature both fracture and internal head injury, are corroborated by a recent study describing head impacts onto carpeted stairs from fall heights of 24.5 and 76.2 cm, producing respective impacts of 50g and 100g. 9
A number of head impact methodologies (HIMs) exist for predicting the risk of sustaining head injury during an impact. The least sophisticated HIM requires analysis of the peak acceleration (peak g), for which a broad range of opinions exist as to the level at which a person can be expected to sustain a critical head injury. Peak accelerations have been proposed, as an estimate of head injury tolerance, and a spectrum of head injury risk has been proposed. Consensus suggests the following: <50g = permanent damage unlikely; 50g–150g = small risk of permanent damage; 150g–200g = moderate-definite risk of permanent damage and >200g = grave risk of permanent damage. 10–15,20
The head injury criterion (HIC) is a more universally applied HIM. Also based on the acceleration–time waveform, HIC considers only selected data from a simulated impact; ensuring that the less injurious portion, for a prescribed time period of the acceleration–time waveform, is excluded from the calculation. HIC provides a correlation between the acceleration/time data, derived from the headform drop tests and the percentage risk of life-threatening head injury in a given population. The Federal Motor Vehicle Safety Standard (FMVSS) stipulates that HIC = 1000 equates to a critical level of injury for approximately 16% of adults. 21 For children, a HIC = 840 has been proposed as an equivalent measure 17 and for infants (6 months) a HIC = 390. 15
By using the above HIM and threshold values, this study aims to illustrate the range of injury risk across a range of impact locations at a scene by performing in situ headform impact tests.
Method
Since the medical reports identified that the infant's head was the likely primary impact point, this study applied the methodology of Cory and Jones 1 for investigating head injury risk during impact with domestic surfaces. Impact tests were conducted at the scene, where it was alleged that a six-month-old infant sustained a complex skull fracture and subdural haemorrhage as a result of a short fall from a carer's arms. Since the importance of impact surface has previously been established, 1 a series of tests were performed to investigate whether different potential impact sites, across the scene, posed different risks of producing head injury. The scene was ‘mapped out’ into 10 × 10 cm segments and the headform, shown in Figure 2, impacted at the centre of each segment. Impacts were conducted from two different drop heights, representing the approximate fall distance described by the carer: onto (i) the upper landing and upper step area, 1.2 m (that is, mean axila (armpit) height 16 ) and (ii) the stairwell area, 1.42 m (that is, mean axila height including the step height 16 ).
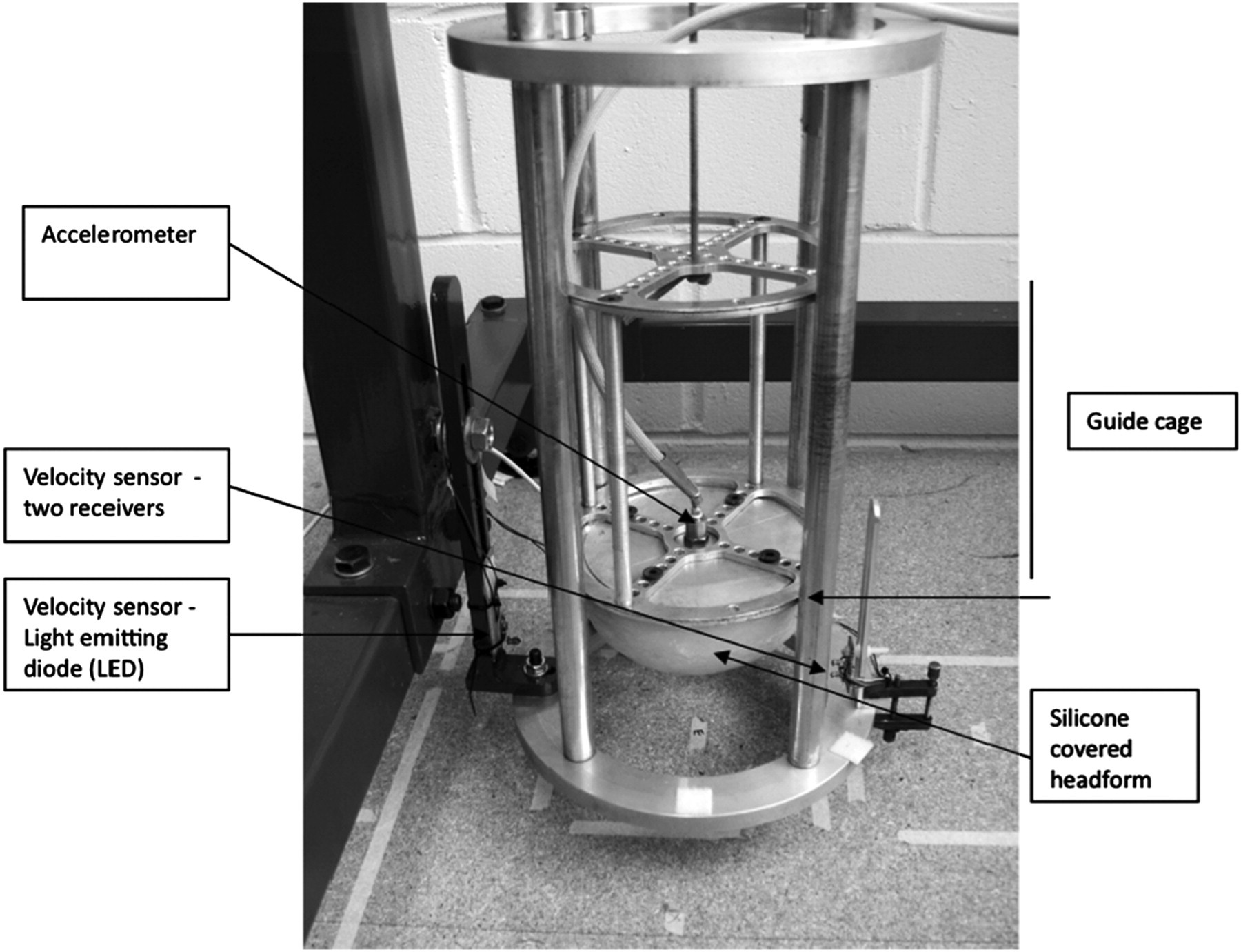
Infant head impact measuring device
The test procedure consisted of the following:
Test 1 – The headform was dropped through a fall height of 1.2 m onto:
the landing the edge of the landing step the edge of the bathroom step Test 2 – The headform was dropped through a fall height of 1.42 m onto:
the stairwell
To ensure the headform provided a human-like (biofidelic) response it was assessed using the guidelines set by Hubbard and McCloed
18
for the calibration of crash test dummy heads (Hybrid III) and the National Highway Safety Administration (NHTSA) FMVSSs
17
Hybrid III calibration values. The Hybrid III dummy is accepted as the current standard in crash test dummies. The headform was dropped 0.367 m onto a rigid temperature soaked, flat steel plate. To ensure calibration the test results must show peak g between 225g–275g and oscillations of less than 10% of the main pulse.
18
The impact acceleration was recorded using an acceleration-measuring transducer (accelerometer, Bruel & Kjaer Type 4369) mounted rigidly on the vertical axis of the headform. The output from the accelerometer was connected to a charge amplifier (Bruel & Kjaer Type 2626) by an accelerometer cable. The charge amplifier was connected to an analogue to digital converter, which was connected to a multi-channel recorder connected to a PC. The relevant data were then input into the USD HIC software (NHTSA) to calculate the HIC.
Results
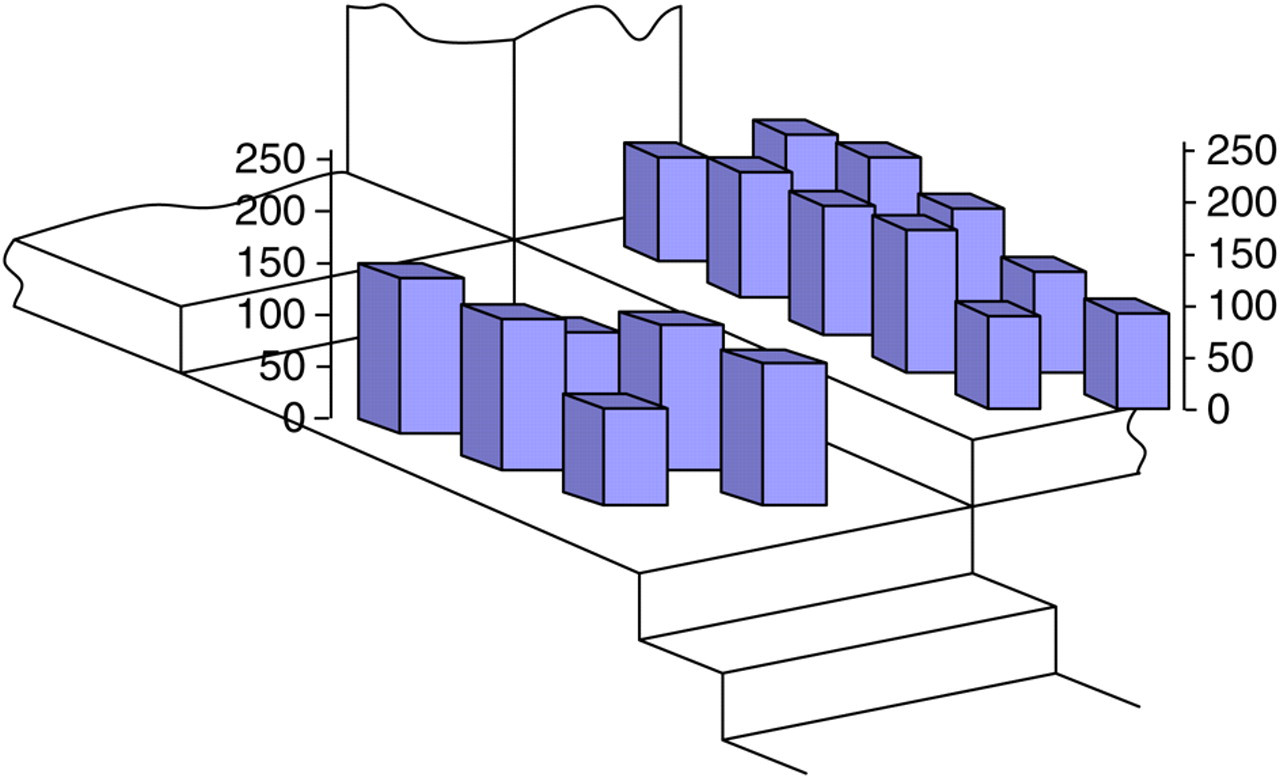
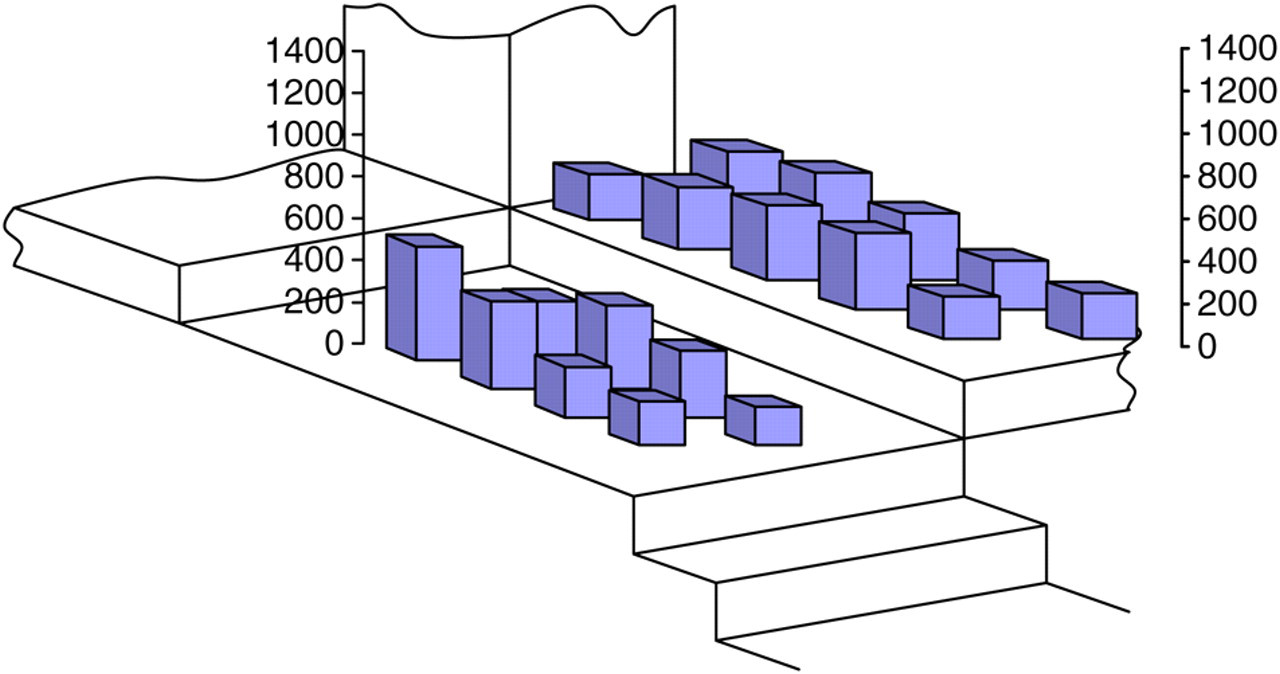
The peak acceleration of the headform was recorded on impact at each 10 cm × 10 cm segment of the area in which it was alleged that an infant had sustained significant head injuries (Figures 3 and 4). It is apparent that the acceleration is greater on the steps (Figure 3), with values in excess of 250g recorded, compared with the landing and stairwell areas (Figure 4) where the maximum acceleration was approximately 150g. A similar trend was also noted when investigating the HIC (Figures 5 and 6), with the maximum value of approximately HIC = 1400 being reported on the two steps. The greatest HIC, reported on the landing/stairwell area, was approximately HIC = 600 (Figure 6).

Peak acceleration (g) of the headform impacting on the bathroom and landing step (1.2 m)
Peak acceleration (g) of the headform impacting onto the landing (1.2 m) and stairwell (1.42 m)

HIC values of the headform impacting on the bathroom and landing step (1.2 m)
Peak acceleration (g) of the headform impacting onto the landing (1.2 m) and stairwell (1.42 m)
Discussion
A series of infant headform drop tests were performed at a scene where it was alleged that a six-month-old infant sustained a complex skull fracture and a subdural haemorrhage as a result of a short fall onto flooring and steps of the landing and stairwell (distances of 1.2 and 1.42 m, respectively). Two established head injury methodologies were applied to illustrate the potential variation in the risk of sustaining head injury at different impact sites across a scene. Thus, values of peak g were recorded and HIC calculated.
The peak g data presented in Figures 3 and 4 indicate that a broad range of impact accelerations were recorded across the scene. The flooring of the steps leading to the bathroom and landing areas (Figure 3) produced accelerations on impact, with values ranging typically between 150g–250g. Conversely, the landing and stairwell areas (Figure 4) had greater impact attenuating properties, with impact data generally considerably lower, ranging between 100g and 150g. Since there is general agreement within the literature that the threshold for grave injury is 200g,
10–12,17
then:
Sixty-seven percent of headform impacts from a fall height of 1.2 m onto the bathroom step (Figure 3) exceeded the threshold for grave injury; Seventy-five percent of headform impacts from a fall height of 1.2 m onto the landing step (Figure 3) fell within the range of moderate-definite risk (that is, 150g) and grave risk; 100% of headform impacts onto the landing and stairwell from a fall height of 1.2 and 1.42 m, respectively (Figure 4), fell within a range where risk of serious injury is considered small (that is, <150g).
Hence, the peak g values suggest a wide range of potential risk for head injury across the scene: grave head injury from a head impact with the bathroom step, serious head injury from impact with the landing step, while impacts with the landing and stairwell flooring are not of sufficient magnitude to produce a serious risk of head injury.
The HIC data, obtained in this study, are compared with injury assessment reference values (IARVs) published in the literature. The IARVs associated with adult head injury include the HIC = 1000 injury tolerance/percentage life-threatening head injury risk curve; 17 HIC = 840, 19 the threshold for sustaining a critical impact in children and specifically for a six-month-old infant the HIC = 390. 13,15
The headform impact onto the bathroom step (Figure 4) produced a range of HIC values, which, when compared with the HIC = 1000, 17 equated to a 2–30% risk of life-threatening injury being predicted. Comparison with the HIC = 840 threshold 19 showed that 83% of the impacts exceeded the critical load value. Headform impacts onto the landing step corresponded to a 2–12% risk of life-threatening head injury, 17 with 75% of the impacts exceeding the critical load value. 19 HIC values for the headform fall height of 1.42 m onto the stairwell represented a considerably reduced risk of sustaining serious head injury 17 (0–1%), with no HIC values exceeding the critical load level. 19 Impacts on to the landing presented no risk of life-threatening head injury.
Since no empirical values exist specifically correlating infant head impact acceleration data with head injury outcome, the experimentally derived acceleration-time data were compared with two head injury models. Experimentation on infants is neither possible nor desirable; therefore, the head injury models were derived from simulations based on animal experiments, mathematical modelling, accident investigation and reconstruction, adult volunteer and cadaver studies. Caution should be exercised when applying models to represent humans particularly, as in this case, when they are further scaled down to represent human infants. Even with these limitations in mind, both the peak g and HIC serve to illustrate that a significant range of accelerations and therefore injury risk is demonstrable across a domestic scene and that these data can be applied to investigating and establishing causal links between injury mechanisms and injury outcomes.
Conclusion
By using two HIMs (that is, peak g and HIC) this study has established that the risk of head injury appears highly dependant on the area of floor onto which an infant's head might have impacted. The point of the paper is not to attempt to explain what exactly did cause the infant's injuries, but rather to demonstrate the variation which potentially exists within a suspected crime scene, with respect to the potential for producing injury. Thus, caution should be exercised when expressing opinions based solely on verbal, written or photographic evidence of head impact surfaces, without due consideration of the specific area onto which a head might have impacted.