
Abstract
It is common that injuries to the head are among the most frequent injuries found in pedestrian accidents, and can constitute a serious, if not fatal, threat. Brainstem lesions have only occasionally been reported in pedestrian injuries. The aim of this study has been to determine the frequency of brainstem pontomedullary lacerations (PMLs) among fatally injured pedestrians, the frequency of concomitant cranial, facial and cervical spine injuries in such cases, as well as to establish their possible underlying mechanism. In this work, PML was present in a significant number of fatally injured pedestrians from a sample of 50 out of 360 cases with head injuries (14%). When observed alone, the most frequent head impact areas were the chin, lateral and frontal (χ 2 = 14.200, df = 4, P = 0.007) in the subgroup with PML. Hinge fractures were most often seen in this subgroup (25 cases), followed by the absence of skull base fractures (χ 2 = 26.320, df = 3, P < 0.01). There are several possible mechanisms of PML in these cases. Impact to the chin, with or without a skull base fracture, could lead to this fatal injury due to impact force transmission. Additionally, lateral head impacts, the most frequent in pedestrians, with subsequent hinge fractures, PML and fronto-posterior hyperextension of the head that is associated with upper-spine fractures, may be possible mechanisms of brainstem injury in fatally injured pedestrians.
Introduction
Road traffic accidents are a global health problem claiming approximately 1.2 million lives annually. The largest group of road user fatalities includes pedestrians who are hit by motorized vehicles. 1 Motor vehicle–pedestrian accidents are a significant source of injuries leading to death and disability; hence, they are a major concern for public health, trauma medicine and traffic safety. 2 Although pedestrian injuries have decreased during recent years, they still remain a major health problem. 3 Additionally, the number of pedestrians surviving vehicle impacts with injuries far exceeds the number of fatalities. In the USA, for instance, there are more than 12 injured pedestrians for every pedestrian fatality. 4
It is common that injuries to the head are among the most frequent injuries found in pedestrians, and can constitute a serious, if not fatal, threat to life. 5 While any type of head injury may be sustained, traffic accidents are the most frequent cause of skull fracture, especially of the skull base. 6 Brainstem lesions have been reported in cases where vehicle drivers and passengers were involved in high-velocity accidents and cases where the face or forehead struck vehicle components. 7 However, they have been less frequently observed in cases with pedestrians, motorcyclists and bicyclists. 8–12 Brainstem lacerations may be either partial or complete and are associated with hinge or ring fractures as well as fractures of the cervical spine, which almost always result in immediate death. 7–12
The underlying mechanism of the pontomedullary lacerations (PMLs) is as yet unclear; however, there are several active theories. One of the most accepted mechanisms for PML postulated so far is the hyperextension of the head due to a face or forehead impact as well as anteroflexion and torsion. 8,10 One newly proposed mechanism is chin impact with the transmition of force towards the skull base. 7 Other proposed mechanisms include shearing lesions due to differences in the acceleration and deceleration of the cortico-medullar junction, a parietal, temporal or occipital impact, or sometimes even lacking any impact of the head at all. 8–12
The aim of this study was to determine the frequency of brainstem PMLs among fatally injured pedestrians as well as the frequency of concomitant cranial, facial and cervical spine injuries in such cases. A possible underlying mechanism of PML in fatally injured pedestrians might thus be established.
Materials and methods
This retrospective autopsy study was performed over a four-year period (from 2005 to 2008). The information contained in this study was derived from a review of autopsy records, police reports and hetero-anamnestic data. All the cases in which the cause of death was something other than blunt force trauma were excluded from the study, in order to make the sample as homogeneous as possible in terms of the mechanism of injury. The pedestrians included in the study were injured during a collision with a motor vehicle, but were not run-over. Children under the age of fifteen years were not included in the study because of the different biomechanical properties of their bodies.
A total of 501 autopsy records of fatally injured pedestrians were analysed. There were 378 cases that had some form of severe head injury (brain contusions, skull and other cranial fractures, i.e. head injury of Abbreviated Injury Score – AIS ≥ 3), after which an additional 18 cases were excluded that involved extensive destruction of the head (i.e. evisceration of the brain). A sample of 360 cases of fatally injured pedestrians was thus formed and further analysed.
From these 360 cases, a subgroup was formed that included 50 cases that included a laceration in the junction between the pons and the medulla oblongata – PML. In order to define the specific PML injury mechanism, cases where the rupture of this junction occurred caudally or rostrally, including distal parts of the medulla oblongata or pons as well as the cerebral crura, were also excluded. The cause of death in this subgroup was PML, and all the victims died at the scene of the incident, before their admission to hospital.
The following collected data were included in these cases: gender, age, the presence of brainstem PMLs and concomitant head injuries – brain contusions, skull, jawbone and upper-cervical spine fractures – and local soft tissue injuries of the head. To understand the mechanisms by which PML occurs, the head
The data obtained were analysed using Pearson's chi-squared test, the Mann-Whitney U test, binary logistic regression and Spearman's correlation coefficient for estimating relationships, since all the variables show non-parametric distribution (which were tested using the Kolmogorov−Smirnov test for normal distribution). A P value of <0.05 was considered significant and <0.01 was highly significant. The SPSS software version 17.0 (licence number 106454) was used for the statistical analysis.
Results
A total of 501 autopsy records of fatally injured pedestrians were analysed. Out of these, 378 (75.4%) had some form of head injury, and after the exclusion of 18 cases involving extensive head trauma, a sample consisting of 360 subjects was formed and then statistically analysed. This group was composed of 236 men and 124 women. The average age was 57.1 ± 20.6 years (range 15–95 years).
Distribution of different head injuries in the entire observed group and the subgroup with pontomedullary laceration
Distribution of skull base fractures with regard to different head impact areas in fatally injured pedestrians in the entire sample
The values in brackets represent the number of subjects with pontomedullary laceration
Partial or complete PMLs were present in 50 cases (14%) within the sample of 360 head injuries, which further breaks down to 32 men and 18 women. The average age was 56.4 ± 19.6 years (range 15–89 years).
There were statistically more males than females in the whole sample group, with the male–female ratio at 1.96:1 (χ 2 = 38.844, P < 0.01), while there was no difference of gender distribution in the subgroup with PML compared with the entire sample (χ 2 = 0.062, P = 0.803). This could mean that both genders are equally susceptible to PML occurrence. There was no statistical difference in average age between the PML subgroup compared with the rest of the sample (t = 0.258, df = 358, P = 0.797).
Discussion
Most pedestrians are struck by motor cars or trucks, and the type of vehicle makes a difference to the dynamics of the impact, which – unlike injury to vehicle occupants – is an acceleration, not a deceleration, process. The height of the car bumper bar is well below the centre of gravity for an adult pedestrian, which lies in their abdominal region. 6 When an erect body is impacted upon below its centre of gravity by the front of a car, the legs are ‘knocked away’ in the driving direction, i.e. a rapid rotational acceleration is imparted to the legs and thus to the long axis of the body. 13 The profile of the car's front section determines the movement of the body upon impact: if the bonnet-front is high and blunt, the struck pedestrian is thrown forward in the direction of travel or scooped up onto the bonnet top. If thrown forward, secondary injures will be suffered as a result of striking the ground. 6 The risk of pedestrian death is a well-known function of car impact speed; typically, the risk of fatality has been reported to be 40–90% at an impact speed of 50 km/hour. 14 If the car speed is appreciable (anything over 20 km/hour is sufficient), the body is able to be thrown into the air or knocked down flat with severe impact. The victim thereafter hits the ground sustaining secondary injuries, which may fracture the skull, ribs, pelvis, arm or thigh. If scooped up, the victim will land on either the bonnet or against the windscreen or corner supporting pillar (of the ‘A’ frame). 6 Usually, in vehicle–pedestrian accidents involving bonnet-type vehicles, the pedestrian's head strikes the vehicle in the rear part of the bonnet or on the windscreen area. 15 Violent contact with the windscreen, especially the rim or side pillars, is the most frequent cause of severe head injury from the primary impact. 6 Depending on the precise impact geometry, subsequent forces acting on the body can result in extreme motions of distension/over-extension, rotation and translation. 13
PMLs have occasionally been reported, but none of the studies dealt exclusively with pedestrians. Gunji et al.
10
describe 10 pedestrians with pontomedullary tears concomitant with upper-neck injuries and/or ring fractures out of a sample of 26 victims. Mizoi et al.
16
reported one pedestrian with PMLs associated with ring fractures in a pedestrian hit from behind at high speed by a bonnet-type vehicle, resulting in over-extension of the neck. Kondo et al.
8
reported eight pedestrians who had been hit from behind, also resulting in either traumatic brainstem rents or high cervical cord lesions due to hyperextension. In their study, Ohshima and Kondo showed that pedestrians were the most frequent victims (followed by car drivers themselves) in a group of 134 victims of brainstem injury, which was also often concomitant with upper-spine injuries or ring fractures.
12
PML was present in a significant number of fatally injured pedestrians in the sample of the paper presented here, where 50 out of 360 cases had head injuries (14%) (Figures 1–3). When the subgroup with PML was observed in and of itself, the most frequent head impact areas were the chin, lateral and frontal (χ
2 = 14.200, df = 4, P = 0.007). However, there were two pedestrians without any notable sign of direct impact to the head. Hinge fractures were most often seen in this subgroup (25 cases), followed by the absence of any skull base fractures (χ
2 = 26.320, df = 3, P < 0.01).
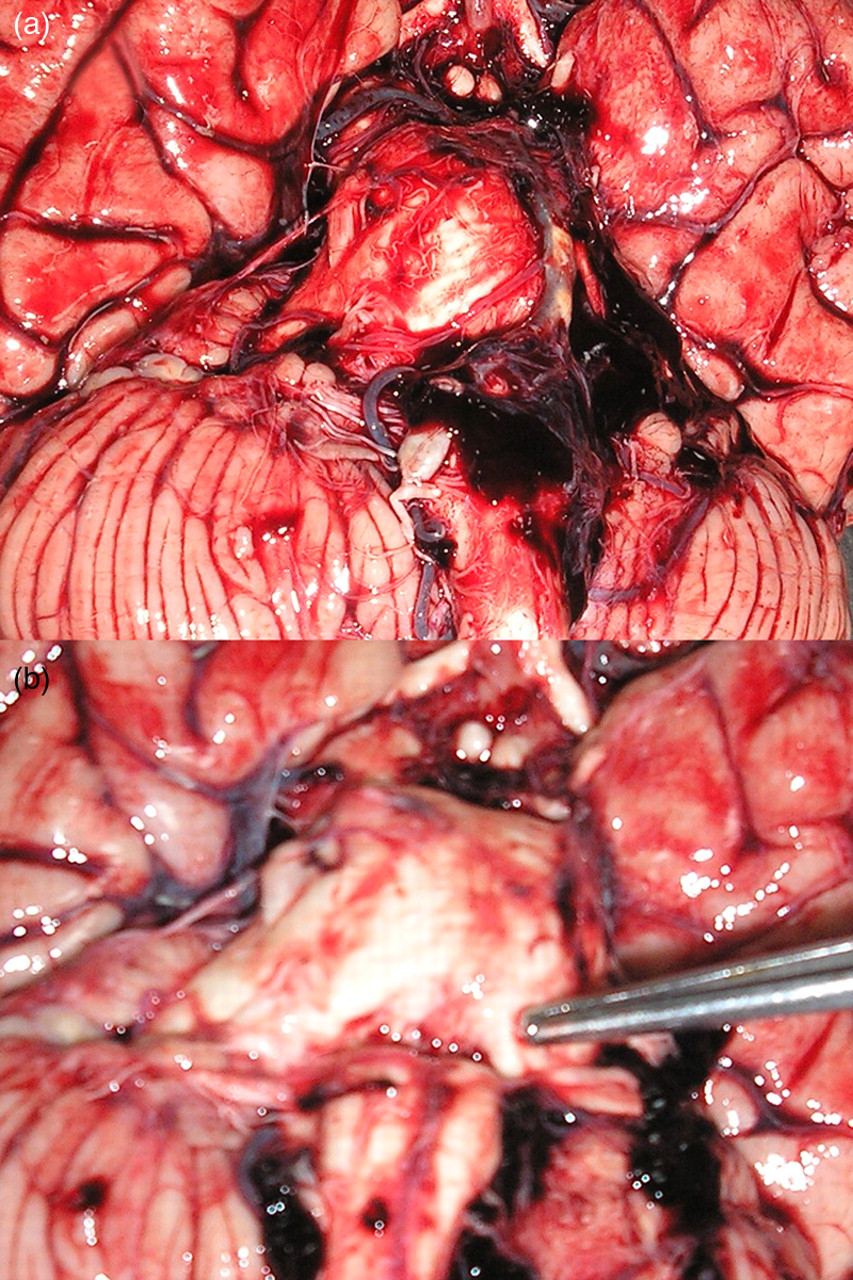
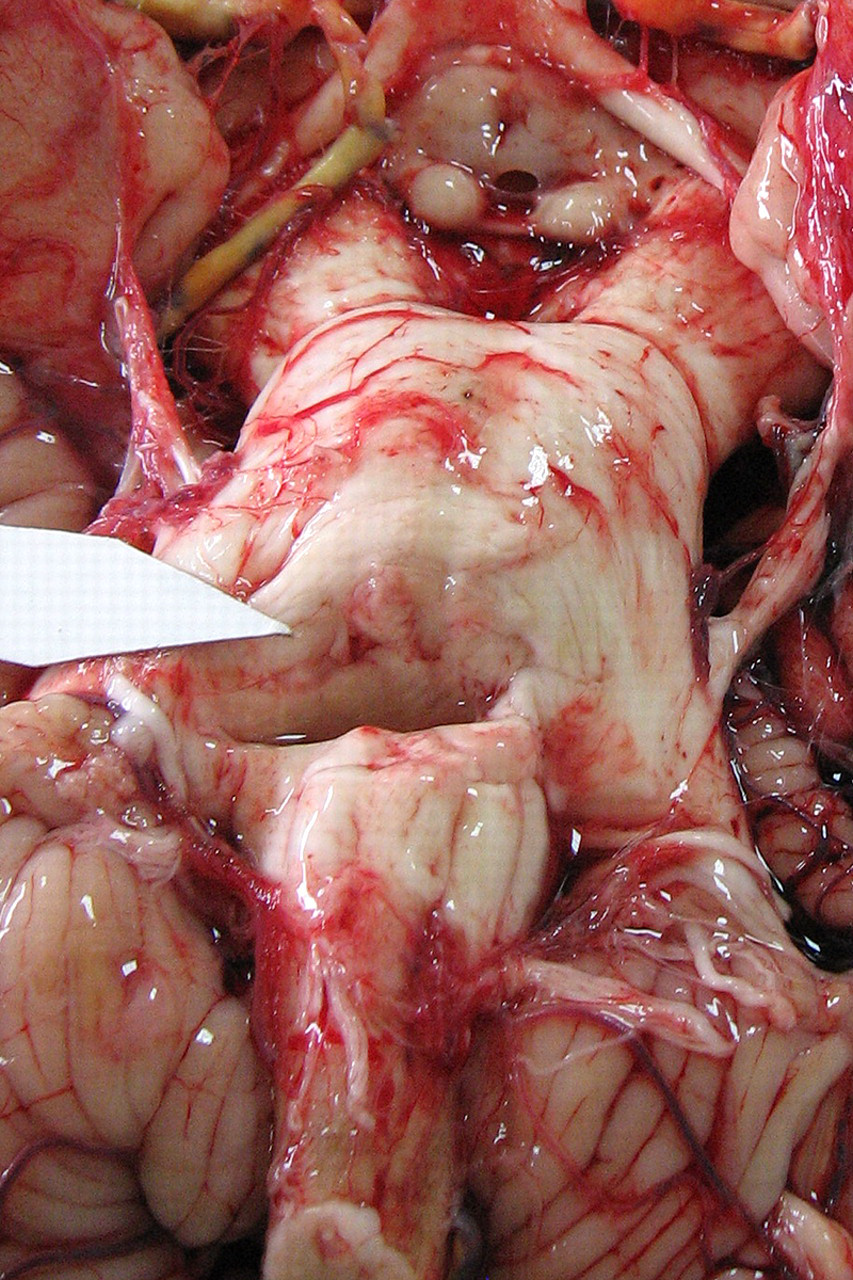
Minimal pontomedullary laceration in a 46-year-old woman, after chin impact, with atlanto-occipital dislocation and no skull base fracture (a) Pontomedullary laceration in a 53-year-old man before removing subarachnoidal blood clot, posterior head impact, with hinge fracture of skull base. (b) Same subject after removing blood clot from pontomedullary junction Almost complete pontomedullary laceration in an 89-year-old man, after chin impact, with hinge fracture of the skull base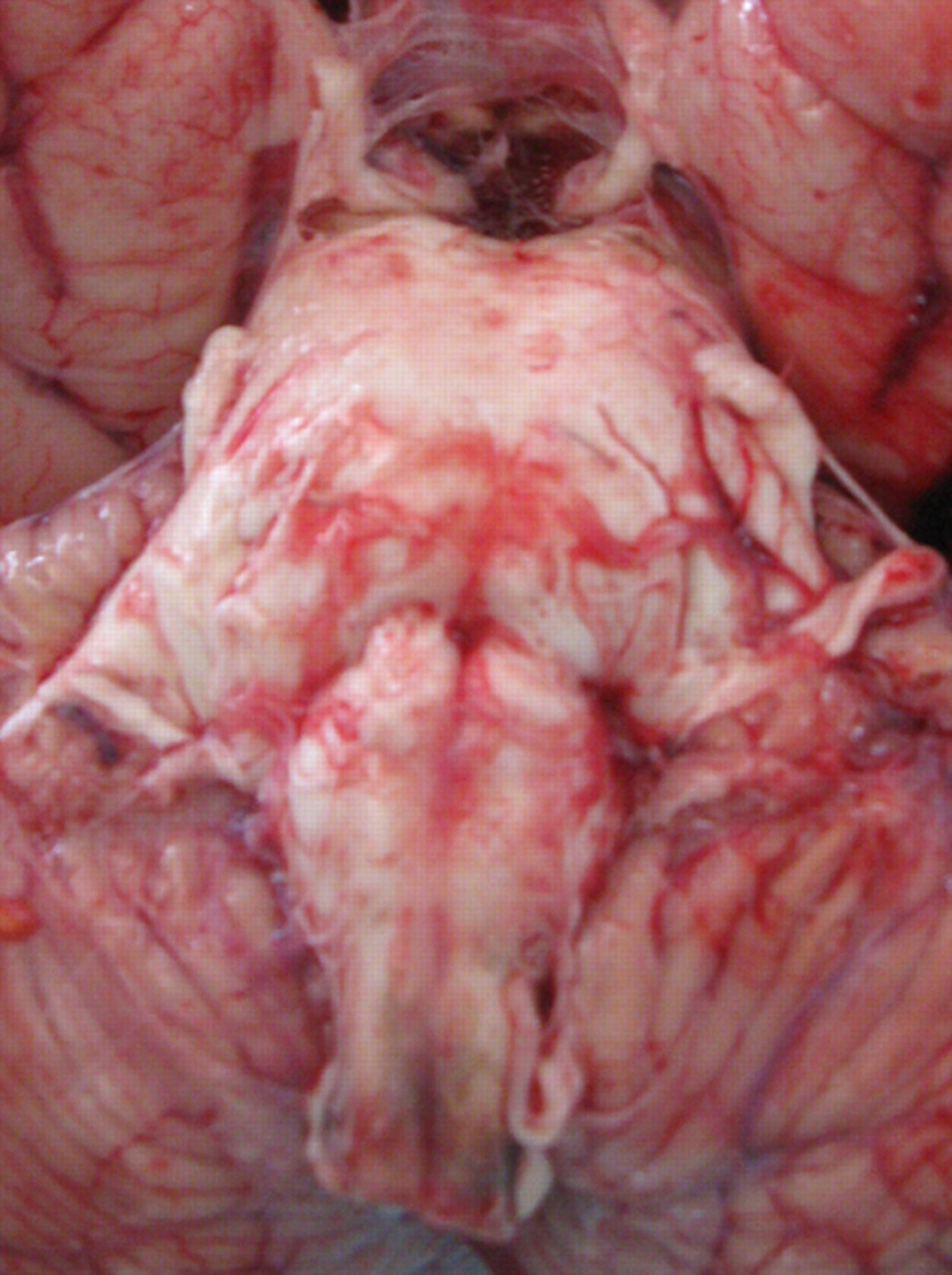
A logistic regression analysis has shown that an impact area on the head together with a specific skull base fracture type were the best predictors of either PML occurrence or absence (Wald = 142,760, B = −1,821, P < 0.01 for the whole model). Skull base fractures were a slightly better predictor than the impact area (for skull base fractures Wald = 89.426, df = 4, P < 0.01; for the impact area Wald = 80.819, df = 5, P < 0.01). Impacts to the lateral, frontal and posterior parts of the head were predictors of PML absence. On the other hand, chin impacts were a reliable predictor of PML occurrence (Table 2). Chin impact leads to violent movements of the head, causing instantaneous craniocervical dislocation, which leads to the indirect lesion of the brainstem, most often PML. This arises from the junction of the pons and the medulla oblongata, anatomically being the thinnest part of the brainstem and thus the weakest spot. 7 Among the 50 cases of PMLs, there was a similar distribution of chin (18 cases), lateral (11 cases), frontal (12 cases) and posterior impacts (7 cases).
Similar mechanisms after chin impacts also lead to specific skull base fractures; namely, ring and hinge fractures. Skull fractures, especially skull base fractures, are common in pedestrians. 6 As just mentioned above, the sample of skull base fractures represented in this paper were reliable predictors of PML occurrence or absence (Wald = 89.426, df = 4, P < 0.01). Although the number of cases was relatively small from the overall sample, the best predictor of PML occurrence was ring fractures (6 out of 6), followed by hinge fractures (25 out of 67). The absence of skull base fractures, as well as any group that included other types of skull base fractures were accurate predictors of PML absence (17 out of 125; 2 out of 160, respectively) (Table 2). However, among the 50 cases of PMLs, hinge fractures and the absence of skull base fractures were most frequently observed.
The impact area of the head was correlated with its type of skull base fracture using a multiple regression model, which showed a statistical significance (F = 5.081, B = 0.221, t = 2.254, P = 0.025). This means that a specific impact area to the head was associated with specific skull base fractures. Due to the high kinetic energy transfer after hitting either a vehicle or the ground, a skull fracture can occur in any part of the head of the pedestrian, but most often in the temporoparietal region, possibly with subsequent hinge fractures. 6 In the present study, these fractures were most often associated with lateral impacts (38 cases) over the entire sample, as well as in cases with PML (11 cases) (Table 2), where it (PML) followed the fracture line that separated the skull base into two halves, and probably was less dependent upon the energy of the impact. On the other hand, it can be seen in cases of chin impact that most were associated with the absence of a skull base fracture and some were even associated with hinge or ring fractures, yet less often with other fractures of the skull base. Most of these cases were associated with PML, which may mean that the impact energy was often sufficient to produce PML, but was insufficient to produce a skull base fracture.
Studies that deal with facial fractures and concomitant brain injuries are controversial. Some show that facial bone fractures reduce the risk of traumatic brain injury since they act as an energy-absorbing cushion and thus protect intracranial organs, while others state that facial fractures indicate that brain-damaging energy transfer might have occurred. 17–19 The study presented here has shown that the statistical analysis was borderline significant in the case of chin impact where mandibular fracture decreases the possibility of PML occurrence (Fisher's exact test P = 0.072). However, quite the opposite result was obtained when mandible fractures and skull base fractures were analysed: they occurred conjointly (Fisher's exact test P = 0.047). In those cases with frontal and facial impact, the fracture of other facial bones was not statistically significant in showing any PML occurrence (χ 2 = 0.554, P = 0.457). Since the data in this study have been somewhat self-contradictory, it cannot be concluded as to whether facial bones act as either shock absorbers or indicators of energy transfer to the brain.
The correlation between upper-cervical spine fractures and brainstem injury in pedestrians has already been demonstrated in several studies, especially with atlanto-occipital and atlantoaxial dislocations. 8,10,12 In the present study, fractures and dislocations of the upper spine, including the atlanto-occipital joint, were significantly associated with PML in cases of frontal impact (χ 2 = 21.698, P < 0.01). This presents a fronto-posterior hyperextension of the neck as a possible mechanism of brainstem injury, which is also supported by previous studies. 8,10,12 This result is statistically significant, regardless of the fact that posterior neck dissection was not routinely performed during the autopsies in all of the examined cases. Some authors have suggested the possibility that injuries to the cervical spine or ring fracture at the base of the skull result from the over-extension of the neck at the first stage of car–human contact. After 60 ms or less from the initial car–human contact, the inertia force to the head can be estimated using a simple equation of the law of motion in physics and can be calculated to be 3 tons or more. This tremendous force is sufficient to produce momentary dislocation of the atlanto-occipital joint, causing violent retraction of the brainstem in pedestrians. 16
The study presented here has shown that PML was present in a significant number of fatally injured pedestrians (14%). There are several possible mechanisms of PML in such cases. Impact to the chin, with or without any skull base fracture, most often led to this fatal injury due to the impact force transmission. Additionally, lateral head impact – the most frequent in pedestrians – with subsequent hinge fracture, PML and fronto-posterior hyperextension of the head associated with upper-spine fractures could be one of the possible mechanisms of brainstem injury in fatally injured pedestrians.
DECLARATIONS