
Abstract
This study is an audit of the Somerset Court Advice and Assessment Service (CAAS) throughout its first year of implementation. It reports that the service successfully met the six desired objectives as set out in its Service Level Agreement. Further to this, it reports that the use of National Health Service electronic patient records within a court setting facilitated the provision of apposite and timely information to the court. Specific findings were that deliberate self-harm/suicidal ideation and mood disorders were the primary reasons for a person requiring CAAS involvement. Violence against the person, breach of orders and theft were the most prevalent categories of offending within this referred group. The prevalence of previous psychiatric history was significantly higher than found in comparable audits. It is likely that this is due to the efficacy of proactive and in vivo utilization of electronic patient records. Conclusions include the need to work in partnership with drug and alcohol agencies and the importance of recognizing that these services have significant clinical benefits for defendants with mental health problems, and the court system in terms of financial savings. We suggest ongoing audit is necessary to guide the development of other schemes in this pioneering service area.
Introduction
It is widely acknowledged that people with mental health problems can be poorly served by the Criminal Justice System (CJS). Their complex needs are often poorly recognized and inadequately managed, a deficiency that contributes to their over-representation in prisons. Imprisonment therefore represents a highly costly intervention, which is often ineffective at reducing re-offending rates in this population, 1–3 can exacerbate mental health problems 4 and is inconsistent with the Government five-year strategy for reducing re-offending.
Background to the need for CAAS schemes
It is important for courts to be aware of defendants’ mental health needs prior to sentencing for many reasons, not least because it may have implications with regard to whether a defendant is fit to plead. Improved understanding would allow courts to put appropriate supportive measures in place for vulnerable defendants to effectively participate in proceedings. They would also be enabled to consider more suitable interventions that might incorporate the input of mental health services. At present, the courts are liable to consider the defendants’ needs by way of requesting a Pre-Sentencing Report. These are generally completed by a Probation Officer and therefore mental health issues and learning disabilities are often not recognized, or are only taken into limited consideration.
On the occasions where mental health issues or a potential learning disability are detected, a psychiatric report is often requested as, for many courts, it is the only avenue for obtaining reliable expert information. There are several concerns with this approach. Firstly, in cases where a psychiatric report is commissioned, it is generally requested by someone who does not have particular expertise in mental health. This often leads to psychiatric reports being unnecessarily requested. In the majority of cases, general advice and signposting would suffice and a full psychiatric report is not required. Secondly, the compiling of a psychiatric report is generally a lengthy process, meaning that the dissemination of pertinent information, along with advice and recommendations for the court will be significantly delayed. During this delay, the defendant may not be receiving necessary mental health support, and may be placed in conditions that are detrimental to their mental state. Thirdly, the content of psychiatric reports is not always beneficial to the hearing. One reason for this is that the psychiatrist asked to prepare the report often operates from outside the area concerned and therefore is unlikely to understand the provision or availability of local services. A fourth issue is the direct cost of employing the services of very highly paid professionals. In summary, the process of requesting psychiatric reports is inherently inefficient, can result in unnecessary delays and adjournments, increase court costs and may lead to ineffective hearings.
The issues mentioned have been longstanding and were initially addressed in 1992 as part of the Reed Review of Health and Social Services for Mentally Disordered Offenders. 5 The review recommended ‘nationwide provision of properly resourced Court Assessment and Diversion Schemes’. Since then, a number of schemes have been established (120 are listed in the Nacro 2009 national directory of schemes). However, these schemes appear to have generally been developed on an inconsistent piecemeal basis, are small-scale and are insecurely funded. 2,3 In an audit by the Department of Health, 6 it was reported that only approximately one-third of Magistrates’ Courts had such schemes in place, falling well short of Reed's ‘nationwide’ recommendation.
As a result of concerns from Her Majesty's Courts Service around obtaining mental health advice and reports that are timely, fit for purpose, and within proportionate costs, a number of national pilot projects were implemented. In 2009, Lord Bradley conducted a review of this issue and considered the impact of the pilot projects. 7 The Bradley Report recommended that Criminal Justice Mental Health Teams are made mandatory in National Health Service (NHS) contracts for mental health and learning disability services. It was also recommended that all probation staff and judiciary should receive mental health and learning disability training.
Lord Bradley's report explored diversion at all stages of the offender pathway, including early intervention (i.e. prevention, pre-arrest and point of arrest), criminal justice and decision-making, and through care and recovery (i.e. custody/detention or community care). The main focus of this paper is on schemes and services that are available to defendants with a mental health problem or learning disability who have reached the criminal justice and decision-making stage and who are due to appear in court.
The types of schemes and services that are currently available can be considered in four broad categories:
8
Diversion schemes: Nacro describes diversion as ‘a process of decision-making, which results in mentally disordered offenders being diverted away from the criminal justice system to the health and social care sectors.’ Such schemes facilitate and accelerate transfer to a health or social care setting if appropriate under the Mental Health Act (MHA);
Diversion panels: These bring representatives from a range of agencies (i.e. police, health, social care, probation, housing, drug services, etc.) together in order to consider and put forward a co-ordinated package of care for the court or CPS to consider;
Assessment schemes: These are concerned with assessing people at the court prior to their appearance, with a view to assisting the court personnel when considering disposal options;
Liaison schemes: These aim at working with multiple agencies on behalf of the defendant in order to provide or facilitate a continuity of services and care and avoid duplication of tasks and roles, whether in the CJS or the community.
However, the reality is that many schemes that are currently available are providing elements of all of these categories depending on the profession of the staff members involved and on the individual cases themselves.
The Somerset CAAS aims to provide elements of both assessment and liaison schemes. It was developed as a result of examining existing schemes, and creating a service based on their functioning and the lessons learnt from them.
The Somerset CAAS has six desired objectives as set out in the Service Level Agreement (SLA):
An improved service to individuals who suffer from mental illness and who have come into contact with the Criminal Justice System; A service that provides the relevant courts with appropriate and timely advice on defendants with mental health problems; Reducing the number of requests for inappropriate psychiatric reports; Reducing the number of adjournments needed to obtain information about defendants who may have mental health problems; Improving the timeliness and usefulness of the information requested; A service that provides value for money.
The Somerset CAAS commenced in September 2009 as a pilot service and operates in Taunton Magistrates Court, Taunton Crown Court and The Specialist Domestic Violence Court sitting at Bridgwater. It provides a service for half the Trust's catchment area, equating to a population of 530,000. Clients can be referred to the service by any member of court personnel, Adult and Children's Social Care Agencies, via self-referral, or by families/carers.
The CAAS practitioners have access to the NHS Trust's electronic patient records (RiO), installed in the courts. This enables them to proactively screen the defendants appearing before the courts in terms of whether they are known to the Trust's mental health services and if they are, it provides them with both historical and up-to-date information regarding their care plan.
The CAAS practitioners are therefore in a position to produce a screening report on referred clients, based on a face-to-face assessment (if the client participates) and/or information available on RiO. The screening report outlines whether the defendant is currently known or has been previously known to mental health services. It will also draw attention to any diagnoses, level of co-operation with the care plan and any further assessment that may be recommended. The role of the practitioner is not to make Criminal Justice recommendations, but to inform the court of the defendant's mental health and associated needs. Where appropriate, they will make onward referrals to other Trust teams or appropriate agencies, such as primary care level counselling, housing, drug and alcohol services, etc. If the defendant does not have identifiable mental health needs, this will be made clear in the screening report.
Further medical reports (Psychiatric reports and/or Health and Social Circumstances reports) are requested if (1) the practitioners cannot provide sufficient information regarding the client's mental health to assist the court with sentencing and it is an offence that carries the possibility of a substantial prison sentence; (2) for specific types of offending, in particular arson; or (3) if there are deemed to be concerns around the client's fitness to plead.
Method: audit data collection
Comprehensive auditing of the service is undertaken to ensure that objectives and targets/timescales as detailed in the SLA are being met. Data regarding referrals, screening report recommendations, practitioner coverage of courts and feedback from professionals referring to the service are routinely collected. Audit data from the first year of operation of the CAAS were reviewed.
Results: audit data from the first year of operation
In the first year of operation, there have been 128 referrals made to the CAAS relating to 97 individuals. Thirty-seven of these referrals did not result in a screening assessment. The main reasons for this were: client refused (41%); no practitioner at court (16%); client did not attend court (11%); and not within the remit of CAAS SLA (11%). On average, 11 referrals (range 4–16) were received per month during the first year of operation with the modal figure being 12. The majority of the referrals (74%) were from Taunton Magistrates’ Court with 16% from Taunton Crown Court, 7% Bridgwater Domestic Violence Court and 3% Bridgwater Magistrates’ Court. Proactive screening from the daily court list using RiO accounted for 22% of the referrals. Referrals were received from Custody Staff (27%), Defence Solicitors (16%), Trust Care Co-ordinators (13%), other Trust Staff (16%), other CJS staff (19%); psychiatric liaison staff and self-referral (2%). Ninety percent of the people referred to the service had had previous contact with mental health services in Somerset, prior to their current court case, and over half were currently involved with mental health services.
Identified presenting problem for clients referred to the Court Advice and Assessment Service
It is evident that the main presenting difficulties were deliberate self-harm/suicidal ideation, depression and associated mood disorders, and anxiety and associated disorders. Seven percent of screened referrals presented with psychosis and four percent were identified as having no presenting difficulties.
With respect to substance misuse, it was found that 36% misused both alcohol and drugs; 23% misused alcohol only; 17% misused illicit drugs only; and 25% were identified as having no substance misuse problems.
Figure 1 illustrates that the majority of those screened by the service have committed violent offences against the person (i.e. assault, ABH, etc.), have committed theft, or a public order offence, or have breached their conditions/orders (i.e. breach of bail/community order/conditional discharge).
Types of offence committed. Note: some clients may have committed more than one offence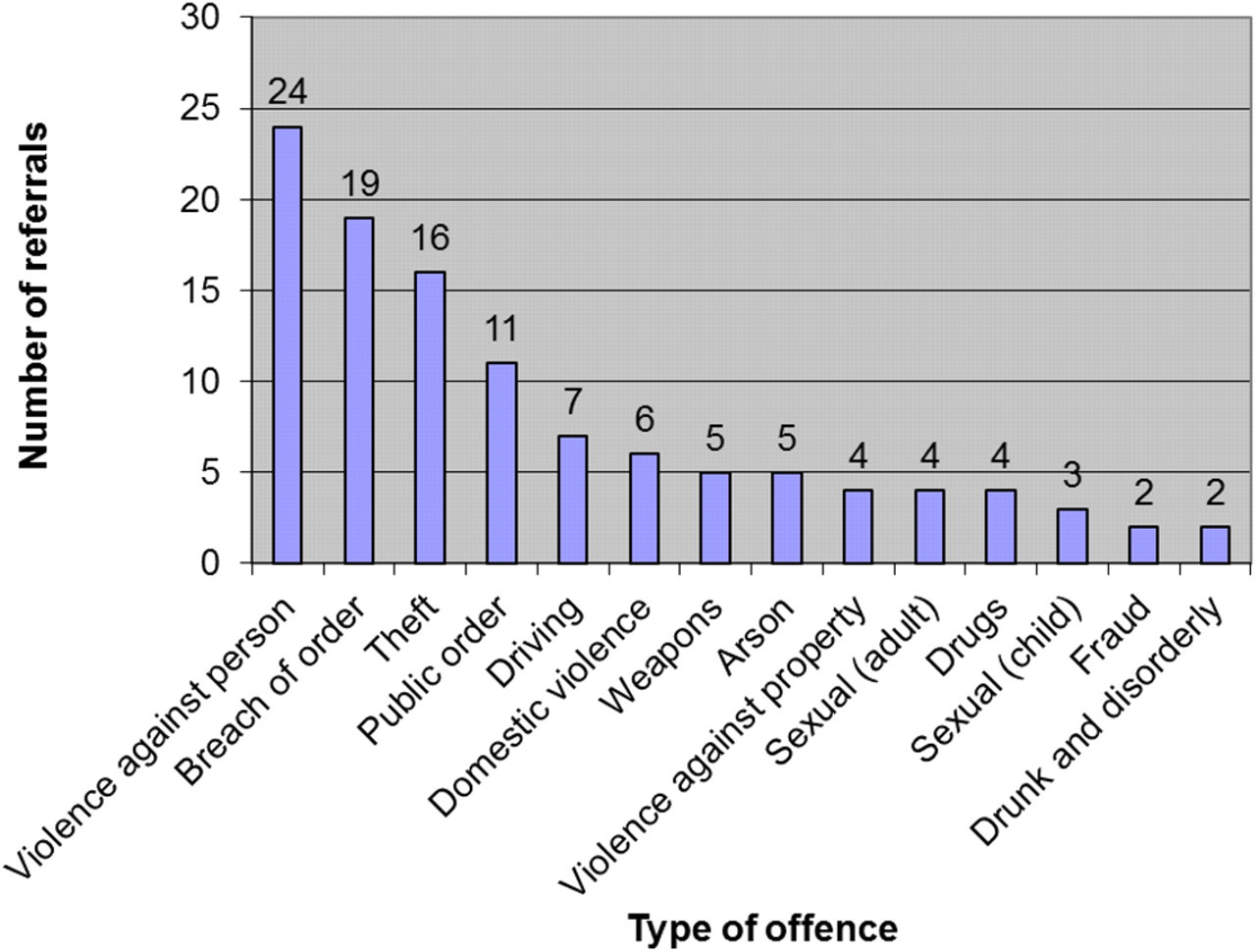
Almost all (93%) of clients’ screening reports were completed on the same day as the referral was made, and 7% were completed between two and five working days following the referral. Screening report recommendations varied widely, with many clients receiving more than one recommendation. The most common recommendation (29%) was referring the client to other mental health teams within Somerset (i.e. assessment, recovery, assertive outreach and crisis/home treatment). Other recommendations included discharging to general practitioner, providing self-help literature, referring to other agencies such as external drug and alcohol services (Turning Point), and referring to prison mental health teams. The practitioners recommended that nine clients should receive further psychiatric reports and that two clients required an assessment under the MHA.
Discussion
Few studies have been published in this area which, given the diversity in services (i.e. liaison, assessment and diversion), makes comparison of audit data difficult. However, it is likely that the literature on such schemes will increase following the Bradley report and the expansion of services.
Key findings from auditing CAAS are:
CAAS facilitates the ‘follow-up’ care of service-users from mental health teams: Following the development of the Somerset CAAS, concern from local Community Mental Health Teams centred on an anxiety that there would be a significant increase in new referrals to their services. The audit data have demonstrated this to be an unfounded concern. Indeed these data show that over 50% of the referrals to CAAS are in current contact with mental health services, and 90% have had previous contact. This corresponds to the findings of Orr et al.
8
who report that the most common reason for referral is a history of past psychiatric contact. In their audit, they found a past psychiatric history in 27% of their referrals in 1997 and 35% in 1998, which is significantly less than this audit. Nonetheless, their interpretation that Court Liaison Services seem to be effectively catering for the follow-up care of individuals in current contact with mental health services is applicable to the findings presented here. We therefore conclude that CAAS appears to be fulfilling a key function: that of maintaining and re-establishing contact between service users and the mental health support they require.
Efficient and accurate screening through the use of electronic patient records in the court: The use of proactive screening, via electronic patient records (RiO) in the court setting accounted for 22% of the referrals. This may account for the much higher number of referrals with a past psychiatric history, compared with the audit by Orr et al.
8
Indeed, they cite lack of access to patient records in the courts as a resource issue for Court Liaison Schemes, and recognized the need for such information to be readily available. Proactive screening using electronic records facilitates the identification of suitable referrals who may otherwise have been undetected by court personnel and solicitors. Electronic patient records in the courts allow information to be gathered quickly, thereby making the screening process efficient and minimizing court delays. Furthermore, it allows onward referrals to be completed swiftly.
Mood disorders and agitated/aggressive behaviour most prevalent presenting problems: The most prevalent identified mental health problems for those referred to CAAS were deliberate self-harm/suicidal ideation, depression and/or anxiety, and agitated/aggressive behaviours. It is difficult to make direct comparisons with audits of other court assessment/liaison services due to differences in the data collected and variation in categories to record data. Nevertheless, the findings of this audit correspond with earlier findings by Orr et al.,
8
which also discovered suicidal behaviour as the leading reason for referral. Orr et al's
8
study, which audited referrals between 1993 and 1998, found that psychosis as diagnosis for people referred to their service fluctuated over their audit period between 19% and 32%. However, the results of this audit indicate that the percentage of defendants referred to the service presenting with psychosis is considerably lower (7%). Such significantly discrepant figures may be due to geographical variation, methods of data collection or changes in practice over time improving management of people with psychosis (i.e. increasing services offering crisis resolution/home treatment, assertive outreach), and reducing the likelihood of them coming into contact with the Criminal Justice System. Audit figures for referrals to Court Assessment Liaison Services with no mental health diagnoses or presenting mental health problems have varied: 23%,
10
12%
11
and 6–28% across the different years audited.
8
This audit found only 4% of referrals had no presenting mental health problems, and this low figure may be attributed to effective pro-active screening, utilizing electronic patient records. In other words, objective evidence is available through the Electronic Patient Record to guide referrals as opposed to subjective opinion often from those with little or no mental health experience or training.
High rates of dual diagnosis: Similar to other audits of Court Assessment/Liaison Schemes, this audit identified high rates of drug and alcohol misuse in those referred to CAAS. Commenting on individuals with drug and alcohol problems alone, Orr et al.
8
proposed that there was a need for increased involvement of drug and alcohol services in Court Liaison Schemes. The high rates of dual diagnosis within the findings of this audit support that proposal, highlighting a clear need for partnership working between CAAS and local drug and alcohol agencies.
Auditing central to service development: Thorough auditing of CAAS has been integral to the running of CAAS and enabled the service to demonstrate in a challenging economic environment that it is meeting its SLA objectives. The data presented here highlight that CAAS has been a cost-effective service to both the NHS and the Criminal Justice System. We have noted that Magistrates have largely accepted the recommendations made by CAAS practitioners, which has resulted in defendants receiving an appropriate and informed disposal, with mental health needs as central. It is our observation that there appears to be a corresponding marked reduction in the number of psychiatric reports commissioned. Unfortunately, a baseline comparison is not currently possible due to the unavailability of data prior to CAAS. However, we feel able to conclude that fewer resources, both in time and money have been misdirected to the commission of inappropriate reports. Finally, with respect to the efficiency of the court, it is possible to assert that proceedings are less likely to suffer from unnecessary adjournments when apposite mental health information is presented at the most opportune time.
In summary, court assessment/liaison/diversion services are expanding following the recommendations made in the Bradley report. These services have significant clinical benefits for defendants with mental health problems, and the court system in terms of financial savings. The inclusion of electronic patient records into such services clearly improves the efficiency, and adds to the clinical and economic value of the service. The need to effectively audit burgeoning schemes and share findings is clear. In this way, it is hoped that the ongoing critical analysis of the developing Somerset CAAS will benefit both courts and clients far beyond the boundaries of our county.
9
Footnotes
ACKNOWLEDGEMENTS
We acknowledge the input of Dr Chris Clinch and Susan Harrison in preparing this article, and the CAAS practitioners in collating the data.