
Abstract
Anaesthesia-related death is one of the most complex events to be studied in forensic pathology because of its rarity and its doubtful presentation. Particularly, the difficulties in assessing the cause of deaths in such circumstances are underlined. A scale must be considered in order to determine the causal role of anaesthesia in the process leading to death. Indeed, beyond deaths exclusively explained by anaesthetic care, there are deaths that are not anaesthesia-related and deaths explained by surgery and co-morbidities in which the role of anaesthetic care has to be carefully investigated. A retrospective analysis of 3138 autopsies is presented with the aim of better understanding the patho-physiological process of anaesthesia-related mortality and to determine the causal role of anaesthesiological care in the process leading to death, thus assessing the real incidence of deaths due to anaesthesia (0.16%). In the present study, the number of deaths generically anaesthesia-related (33 cases) accounts for 2.06% of autopsies due to medical malpractice claims and 1.05% of all autopsies. The number of deaths totally related to anaesthesic care is rather low with 0.32% of autopsies due to medical malpractice claims and 0.16% of all autopsies. Anaesthesia-related deaths were due to lack of or delay in intubation (2 cases), acute cardio-respiratory failure (2 cases) and anaesthetic-induced hepatotoxicity (1 case). The importance of a careful forensic investigation (clinical and familial history, medical records, complete autopsy and toxicology), which can lead to a clear understanding of anaesthesia-related deaths, is also stressed.
Introduction
Anaesthesia-related deaths are rare events and are difficult to study. 1 Despite this statement the risk of death in conjunction with surgery and anaesthesia has been studied extensively and though anaesthesia is an area in which very impressive improvements in safety have been made, 2 many questions still arise when we are dealing with these deaths. One of the most significant key points of the issue and a deep matter of judgement is deciding whether a death was a direct result of anaesthesia (death due to anaesthesia), or whether other factors caused the death, only temporally anaesthesia-related. It is noteworthy that most of the existing studies on anaesthesia-related mortality are based on clinical judgement, death certificates based on the International Statistical Classification of Diseases and Related Health Problems (ICD) classification system, and claim analyses, thus representing the epidemiological pattern of anaesthesia-related deaths, which is not completely reliable. The aim of our postmortem retrospective analysis is to study a case series of anaesthesia-related deaths for understanding the patho-physiological process of anaesthesia-related mortality and determining the causal role of anaesthesiological care in the process leading to death, thus assessing the true incidence of deaths due to anaesthesia.
Materials and methods
The clinical data and the autopsy record of the 3138 autopsies performed at the Department of Forensic Pathology of the University of Foggia over the period 1 November 1998 to 31 December 2010 were retrospectively evaluated. Altogether, 1604 autopsies were performed regarding the medical malpractice hypothesis under the Jurisdiction of the Local Prosecutor Office (Figure 1).
Reasons for autopsies being performed in a 12-year period in Foggia, Italy
For the present study, cases with a possible connection between anaesthesia and complications leading to death were selected. In all these cases, the medical and anaesthesia records were reviewed and a case abstract was prepared after collecting postmortem (gross and microscopic findings) and toxicological data.
Results
In 85 of our case series, medical malpractice claims were alleged to be due to anaesthesiological care and involved anaesthesia-related deaths (Figure 2). After the medicolegal autopsies, in 61.18% (52) of these cases any causal connection between anaesthesia and death could be ruled out, since clear morphological causes of death were evident (deaths occurring during anaesthesia). Most of the deaths in our case series are totally explained by surgery or co-morbidities; in other words, these are cases in which the medical history and the autoptic findings explained why death occurred. Overall, the most frequently encountered causes were identified in thromboembolic (18 cases) and haemodynamic events (30 cases) in which anaesthetic care did not play any causal role. Likewise, in all cases in which death occurred as a consequence of a sudden unpredictable event (amniotic fluid embolism, air embolism), no deficiencies in anaesthetic management or human error by anaesthesiologists were identified.
Statistical analysis of 85 anaesthesia-related forensic cases
In 24 cases there was the suspicion of a causal connection between anaesthesia and death (deaths to which anaesthesia contributed). Overall, the following situations have been identified in cases in which anaesthetic care could have played a role: coronary artery disease (14 cases) and obstructive or restrictive pulmonary disease (10 cases) triggered by surgical trauma, pain, hypoxemia, hypothermia, bleeding and anaemia, fasting and intubation/extubation. However, no deficiencies in anaesthesiological teamwork that could have promoted the occurrence of the events leading to death or could have played an aggravating role were found in these cases. Moreover, there were four cases in which poor postoperative care was recognized (inadequate management of postoperative blood loss associated with delayed or absent blood transfusion, lack of constant vigilance in a case of sepsis associated with intra-abdominal haemorrhage).
Finally, only in five cases was death due to anaesthesia alone (deaths due to anaesthesia).
In most of the deaths due to anaesthesia, anaesthesiological care was regarded as substandard. In all these cases, except for the one in which the death resulted from a complication of the volatile anaesthetic used, 3 anaesthesists were found negligent. Concerning the types of mistakes in the cases of approved medical malpractice, lack of preoperative preparation and failure to intubate the patients are the most significant criticisms highlighted in our case series.
Discussion
In the present study, the number of deaths generically anaesthesia-related (33 cases) accounts for 2.06% of autopsies due to medical malpractice claims and 1.05% of all autopsies. Allegations of human errors by anaesthesiologists are even rarer taking into consideration the total number of liability lawsuits and preliminary proceedings against physicians. A very interesting point is that in the majority of cases, based on the autopsy report, the case was settled due to the fact that the causal connection between anaesthesiological care and death could not be proved, thus confirming that autopsy is even nowadays a very efficient method of clarifying medical malpractice claims. 4 This is of special interest in anaesthetic-related deaths, which are very difficult to study. 5 In fact, one of the most significant key points of the issue and a deep matter of judgement in the analysis of mortality related to anaesthesia is assigning a death as being a direct result of anaesthesia (death due to anaesthesia), or a result of other factors, only temporally anaesthesia-related. Dealing with this matter, Lienhart et al. 1 presented an innovative approach to identifying specific causes of anaesthesia-related deaths by using a three-point scale: ‘not anaesthesia-related’ (deaths totally explained by surgery or co-morbidities and deaths explained by surgery or co-morbidities but in which anaesthetic care could have played only a minor role), ‘partially related to anaesthesia’ (i.e. deaths explained by surgery or co-morbidities but in which the role of anaesthetic care was not minor) and ‘totally related’ (i.e. deaths exclusively explained by anaesthetic care).
According to this, in our retrospective analysis the number of deaths totally related to anaesthesic care is rather low with 0.32% of autopsies due to medical malpractice claims and 0.16% of all autopsies (Figure 3). Anaesthesia-related deaths were due to lack or delay in intubation (2 cases), acute cardiorespiratory failure (2 cases) and anaesthetic-induced hepatotoxicity (1 case).
Number of autopsies and causal link between deaths and anaesthesia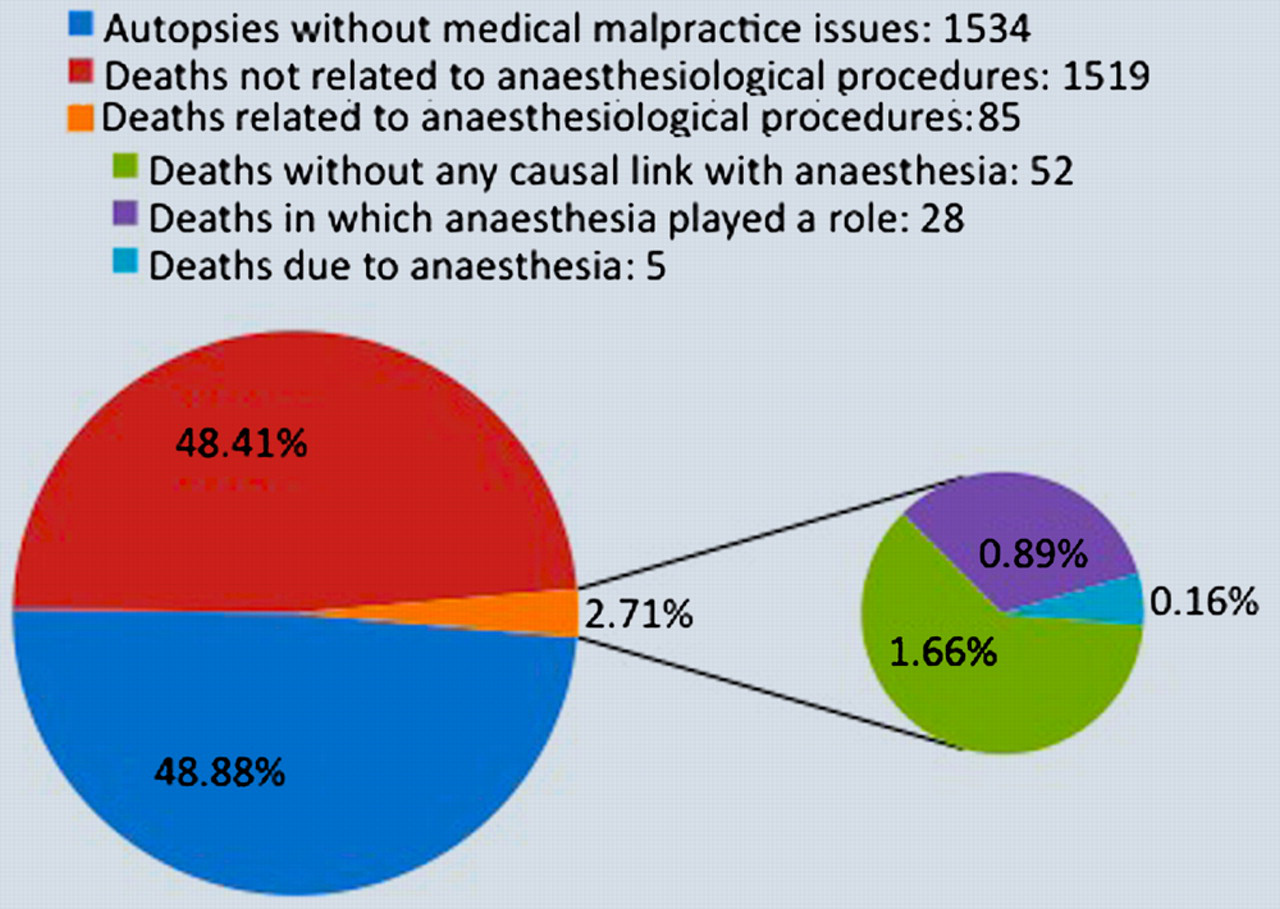
One of the greatest difficulties in determining the causal role of anaesthesia in the process leading to death derives from the fact that many of the existing surveys examine the epidemiological pattern of anaesthesia-related deaths. Data are generally collected from death certificates based on the ICD system 6 and from insurance companies’ files. Many limitations arise when these kind of data are used. First of all, only a minority of adverse events result in malpractice claims 7 and the data are gathered by insurance organizations for the purpose of resolving malpractice claims. The incompleteness of specific detailed information regarding the sequence of events or mechanism makes the claim analysis system ineffective. Moreover, when root causes are searched from questionnaire analysis or through discussion with experts, differentiation between deaths partially related to anaesthesia and deaths not related to anaesthesia in which anaesthetic care could have played only a minor role was indeed often difficult. 1 Finally, the validity and reliability of the multiple-causes-of-death data remain a concern. Although previous research has shown a high reliability of the multiple-causes-of-death data for some diseases (such as cancer and external causes), their sensitivity and specificity for detecting anaesthesia-related deaths have not been rigorously examined. It is likely that these estimates of anaesthesia-related mortality missed a portion of anaesthesia-related mortality, particularly those deaths in which complications and adverse events of anaesthesia/anaesthetics played only a contributory role. On the other hand, some of the deaths associated with anaesthetics or analgesics identified through death certificates may not be related to anaesthesiological practice. 8,9
Conclusion
In conclusion, in the issue of medical malpractice, the data from epidemiological research are not completely reliable and such estimates of mortality are also susceptible to bias. Data on malpractice cases are furthermore available from the files of the institutes of forensic medicine representing the best available data source on lethal cases, 10 since autopsy provides unique paramount information concerning the cause of death. As has been highlighted, 10 autopsy is a valuable tool to reveal and prove medical malpractice. Specifically, in the issue of anaesthesia-related deaths, 11 failure to perform autopsy, which could provide valuable supplementary information concerning the medical condition of the patient, as well as the reason and condition under which the operation was undertaken, constitutes a problem. Based on our study no data on the incidence of anaesthesia medical malpractice can be given since the autopsy rate and total number of cases are too low to measure incidence and prevalence rates of errors and adverse events, but our results reinforce the need for a complete postmortem investigation in all cases of anaesthesia-related deaths.
As Cook et al. 12 suggest, establishment of a rigorous process for examining anaesthesia-related events in all countries, which would be likely to illuminate the cause of sentinel events, would improve learning and, more importantly, have the potential to benefit patients by improving patient care.