
Abstract
This re-audit assessed whether wards at South West London and St Georges’ mental health trust (SWLSTG) met agreed standards regarding informing inpatients about their legal status in hospital and rights, following an initial audit in 2009. Three general adult wards were re-audited, and other general and specialist wards (addictions, eating disorders, deaf services and obsessive compulsive disorder) were added. One hundred and five people (61 informal, 44 detained under the Mental Health Act 1983, revised 2007) on 10 wards were interviewed using an agreed proforma. The re-audit of wards A–C showed improvement: 81.3% of informal inpatients were aware of their legal status, versus 54.2% in 2009 (P = 0.101). Including new wards D–K, 90.2% knew their status (P = 0.0002). Of the informal patients, 65.6% knew they could refuse treatment (P = 0.0184) (on wards A–C, 68.8%, P = 0.105) versus 37.5% in 2009. Despite some improvement, the patient experience of informal admission or detention in hospital still sometimes crosses legal boundaries. This audit highlights the need to improve awareness of patient rights and demonstrated how local presentation of audit improves practice.
Introduction
The experience of being an inpatient is intended to be fundamentally supportive and therapeutic. However, certain aspects of the psychiatric inpatient experience can be highly stressful, for example, sharing facilities, attending ward rounds and restrictions on movement. In the 1970s psychiatric care moved towards unlocked wards and community care 1 and article 5(1) of the European Convention on Human Rights states ‘No one shall be deprived of his liberty save in … the lawful detention … of persons of unsound mind … ’. 2 However, services have a duty of care to protect against harm to self or others, so ward staff often face difficulties balancing right to freedom versus safety. The practice of locking ‘open wards’ has been increasing across the UK, including at South West London St George's Mental Health Trust (SWLSTG). This appears a reversal in the ethos of psychiatric care over the past three decades. The Mental Health Act Commission 3 noted that ‘Nurses spend much of their time engaged in intensive observation of a few patients, but a quarter of wards had no nurse interacting with patients at the time of the visit.’ There is an anecdotal perspective that locked doors increase the time nursing staff spend with patients rather than ‘guarding the door’, supported by an audit in York. 4
The majority of psychiatric patients are admitted informally (the MHA Commission found 70% informal patients, 30% detained in a 1998 survey). 3 Section 131 of the Mental Health Act 1983, revised 2007 (MHA) emphasizes the right of patients to be admitted without legal restrictions, and Section 132 details hospital managers’ duty to inform detained patients of their rights. There is no legal duty to inform informal patients of their rights but it seems good practice to do so. Rogers et al. found that of 516 informal inpatients, 80% felt they had not received enough information about what to expect of treatment. 5 Sugarman and Ross found only half (67/117) of informal psychiatric patients believed they were legally allowed to leave hospital and only 55/117 believed they had the right to refuse treatment. 6
At SWLSTG the ‘locked door’ policy is in place ostensibly to protect individuals within from malign external influences (such as the sale of illicit drugs). The authors were concerned that not all inpatients were aware of their legal rights in relation to the locked door, so in 2009 Lomax and Raphael audited three general adult wards at Springfield hospital, finding worrying deficiencies in the information either given to (or absorbed by) patients in relation to their status on the ward. Only 54.1% believed they were allowed ‘short time away’ from the ward, 33.3% believed they were ‘allowed to go home’ and 37.5% of informal patients believed they could refuse treatment. 7 No informal patient was actually detained illegally, in that all who had asked to leave had not then tried to do so; however, some informal patients’ explanations of why they had not asked to leave included obvious references to fear of reprisals. Actively or passively allowing a culture of letting informal patients remain under misapprehensions about their rights concerning time away from the ward is clearly poor practice, which needs challenging. The audit was presented at the academic programme and the authors planned to re-audit at one year and after wide discussion included other wards within SWLSTG.
Audit standards
100% patients should know whether they are informal or detained under a section of the MHA, and if detained, they should know which section; 100% informal patients should have been offered a leaflet and explanation about their rights (regarding leave, confidentiality, treatment); 100% patients detained under the MHA should have been offered a leaflet and explanation about their rights; 0% informal patients should have been kept on a ward against their will without MHA assessment and an explanation of this; 100% informal patients should understand they have the right to refuse treatment; 100% patients should have been offered a ward welcome pack.
Methods
The sample population was all current inpatients on 28 March 2010 on the four general adult wards at Springfield Hospital, two at Tolworth Hospital and inpatients in the national adult deaf service, the national obsessive compulsive disorder (OCD) service, the addictions service and the national eating disorders service. All inpatients who verbally consented and were available were interviewed. Individuals lacking capacity to consent to the interview (e.g. those suffering dementia, a lowered level of consciousness or learning disability) were excluded. It was not feasible to include patients who were on leave during that period, and a small number of patients were discharged before the authors were able to interview. Deaf service patients were interviewed with a British sign language interpreter. Questions were asked using an interview proforma based on the standards above. Results were analysed using ‘Graphpad’ software, using χ 2, or if any value was 5 or less, Fisher's exact test.
Results
The sample comprised 91 women and 96 men. Fifty women, 55 men were available, suitable for and consented to interview. Reasons for not interviewing are displayed in Figure 1. Sixty-one informal patients (of 100, 61% response) and 44 detained patients (of 87, 50.6% response) were interviewed. The mean age was 41.4 years.
Reasons for not interviewing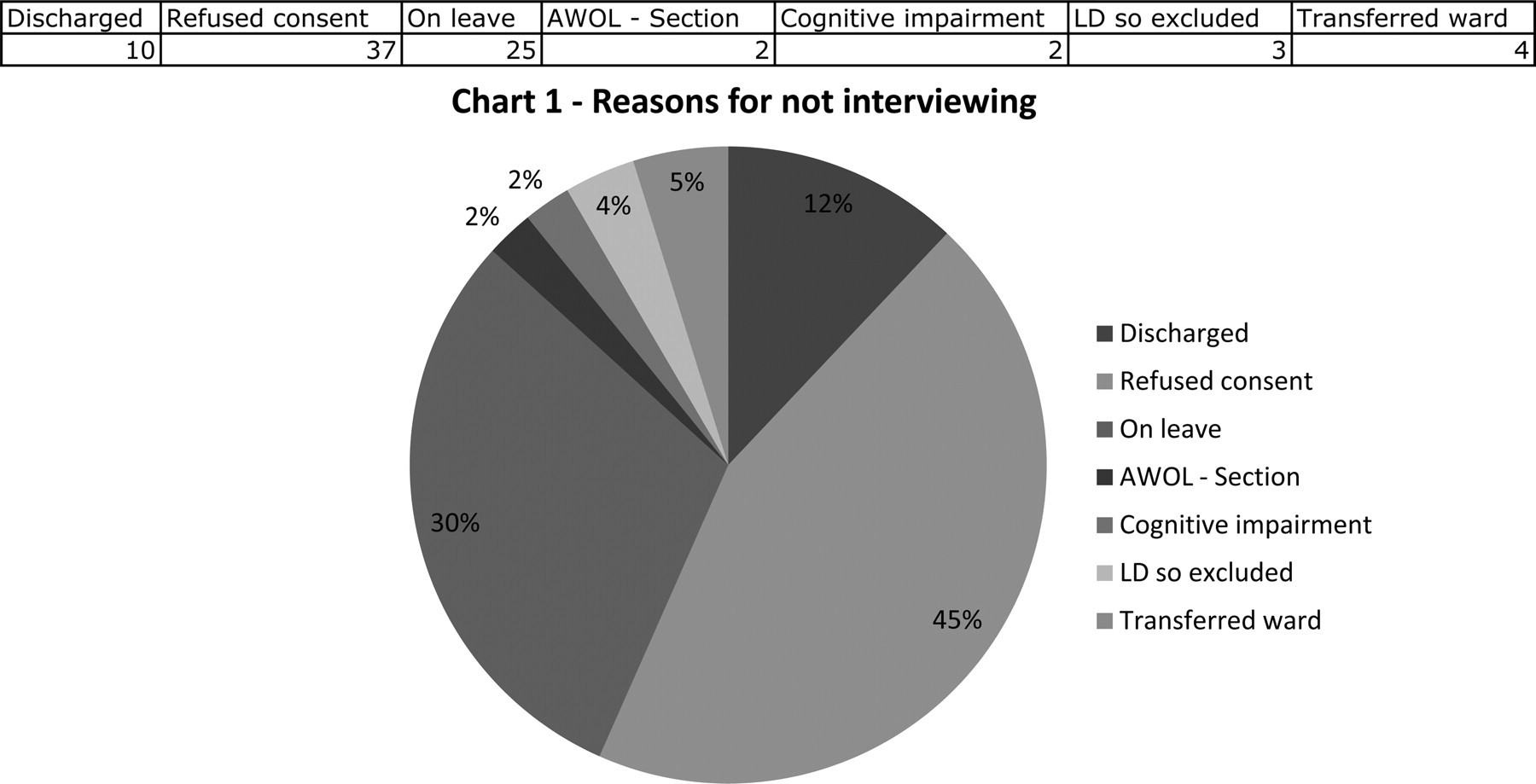
Standard 1: 100% patients should know whether they are informal or detained under a section of the MHA
Figure 2 shows that there was improvement on wards A–C: 81.3% of informal inpatients were aware of their status versus 54.2% in 2009 (P = 0.101). When results were expanded to include the new sample of wards D–K, 90.2% knew their status (P = 0.0002). Clinically there was a poorer awareness among detained patients, with only 60% of ward A–C patients knowing which section they were detained under versus 80% in 2009, but there was no statistically significant difference (P = 0.298) (wards A–K also not a statistically significant difference, P = 0.738). There were four detained patients who thought they were in hospital voluntarily, and two informal patients who thought they were detained under the MHA.
Awareness of inpatient legal status (relates to standard 1 in the Results section)
Standard 2: 100% informal patients should have been offered a leaflet and explanation about their rights
On wards A–K, 24 informal patients (39.3%, P = 0.0723) felt they had had their rights explained to them versus 12% in 2009. Twenty had received a leaflet (32.8%, P = 0.0644) versus 4% in 2009. However, on wards A–C in 2010 only two had had explanations (P = 0.0723), and two received leaflets (18%, P = 0.1323) – no significant difference. Fifty-five percent of the people who had received leaflets about their rights were on the OCD and substance misuse wards.
Standard 3: 100% patients detained under the MHA should have been offered a leaflet and explanation about their rights
There were no significant differences on re-audit. Twenty-seven said they had been informed of their rights (61.4%, P = 0.452), 13 on wards A–C (52%, P = 0.905) versus 50% in 2009. Twenty-two (50%, P = 0.351) of wards A–K said they had been given a leaflet explaining their rights under the MHA, 13 (52%, P = 0.458) on wards A–C, versus nine (64.3%) in 2009.
Standard 4: 0% informal patients should have been kept on a ward against their will without MHA assessment and an explanation of this
There were improvements; however, following feedback questions were changed between the two audits, so the results cannot absolutely be compared.
‘Are you allowed out of the ward?’: 40 informal patients (65.6%) said ‘yes’ compared with 54.2% saying they were ‘allowed time away’ or would be ‘allowed a short time out for example to shops or café’ in 2009 (P = 0.329), a clinical but not statistically significant difference.
‘Would you be allowed to go home if you asked to go?’: 37 (60.6%, P = 0.0538) informal patients on wards A–K said they would be (9, 56.3% on wards A–C, P = 0.749). This was an improvement from 2009 in which 33.3% thought they would be allowed home.
‘Have you ever asked to leave and not been allowed?’ (new question 2010): 47 (77%) said no. The 12 patients who said ‘yes’ generally said they had agreed to stay when staff explained they were too unwell and would be medically advised to stay. When asked why they would not be allowed, one said ‘I'm just not’, another ‘If I argue they'll section me anyway’. These statements were distinctly less filled with fear of reprisals (e.g. rapid tranquillisation) than in 2009. No one interviewed described ever having been physically stopped from leaving the ward against their will without MHA assessment, or believed they could not leave because the door was locked.
Standard 5: 100% informal patients should understand they have the right to refuse treatment
Forty of all informal patients (65.6%, P = 0.0184) knew they would be allowed to refuse treatment (on wards A–C, 68.8%, P = 0.105), a significant but incomplete improvement from 37.5% in 2009.
Standard 6: 100% patients should have been offered a ward welcome pack
Eight (21.1%) patients were offered a welcome pack in 2009, five read it (13.2%) versus 32 of all patients in 2010 (30.5%, P = 0.267) with 25 having read it (23.8% P = 0.245). In 2010, on wards A–C four (9.8%, P = 0.215) had been offered one, three read it (P = 1.00), showing variation in ward practice, but no statistically significant change over time. The largest number of people who received welcome packs came from wards F and H (eating disorders, OCD and alcohol wards).
Specialty results
At Springfield the alcohol and OCD services share a ward, a nursing team and ward culture, but have different medical teams. Hundred percent patients on this ward were informal and knew their status and 100% knew they could refuse treatment. Fifty percent were not allowed out, but it is the alcohol team's policy that people do not leave during alcohol detoxification for health and safety purposes (this is made clear on admission, and if people choose to leave detoxification ends). These results perhaps reflect the specific illnesses on this ward and a greater drive to seek treatment, but 80% had received a welcome pack and 60% felt they had had their rights explained to them. On the drug rehabilitation ward, 100% patients were informal and 100% knew their status. Hundred percent felt they had had their rights explained and 83.3% had received a leaflet about their rights, 33.3% a welcome pack. Hundred percent knew they could refuse treatment and 100% said they would be allowed home if they asked.
Discussion
This audit showed clinically significant improvement in patients’ understanding of their rights and hence the information given to them, although the relatively small numbers of patients involved in the 2009 audit means many results are non-statistically significant. The strengths of this audit are that it was a brief snapshot of all inpatients on a particular date, meaning no time over which patients could learn from other participants, inflating or deflating results. Staff were not warned exactly when the audit would take place, so they could not alter practice specifically around the audit period. In terms of limitations, the study was small compared with studies by Rogers et al. 5 and Sugarman and Moss, 6 and achieved only a 61% response rate among informal patients and 50.6% response rate among detained patients. The two audits are not directly comparable given the inclusion of highly specialist tertiary wards in 2010. These wards include more planned admissions and a more structured ward routine. Due to the nature of the illnesses, patients with OCD or eating disorder may be more likely to ask more questions, and absorb more information than patients with other psychiatric illnesses.
The differences between 2009 and 2010 are unlikely due to the information leaflet designed during the 2009 audit because the leaflet has not been widely distributed (due to cost implications). However, the 2009 audit influenced other practical changes such as signs by ward doors indicating informal patients were allowed to leave. The differences may reflect the wider variety of illnesses and patients in this audit, and difference in ward practice; however, it also may reflect greater understanding and awareness in staff due to presentation of audit locally. This audit highlights the need to improve awareness of patient rights. It does show modest improvements, demonstrating how presentation of audit improves practice. However, patient experience of informal admission or detention in hospital still sometimes crossed legal boundaries, with significant numbers of informal patients believing they were not allowed to leave hospital or refuse treatment. This audit led to a SWLSTG multidisciplinary staff survey of mental health law, and the results will be used to influence the content of induction and training programmes. Future research is needed on the most effective methods of verbal and written communication to improve patient knowledge about rights.
DECLARATIONS