
Abstract
Deaths occurring during and/or in close proximity to physical restraint have been attributed to positional asphyxia, a conclusion primarily based on opinion and reviews of case studies. This review sought to identify the current scientific evidence available in regard to the aetiology of adverse events or death occurring during or in close proximity to physical restraint. A systematic search of electronic databases (SPORTDiscus, AMED, CINAHL, MEDLINE, PsycINFO) for papers published in English, between 1980 and 2011, using keywords that related to restraint, restraint position and cardiovascular function resulted in 11 experimental papers being found for review. The term positional asphyxia as a mechanism for sudden death is poorly understood. The literature shows that restraint position has the ability to impede life-maintaining physiological functions, but that the imposed impediment is not uniform across all restraint positions/techniques. Further research is required to ascertain the risks posed by struggling during restraint for more prolonged periods of time and in different positions using varied techniques of restraint. This research should seek to and rank known or future risk factors of adverse events occurring during restraint, seeking to understand the interactions and if present the cumulative effect of these risk factors. Finally, future research should focus on populations other than apparently healthy male adults.
Introduction
Aggression and violence occur in many human service settings, representing a significant risk to staff, service users and/or members of the public. The use of restraint defined as ‘the restriction of a person's liberty of movement’ (p. 105) 1 is an accepted risk management strategy for the short-term management of aggressive and violent behaviour. 2–6 Restraint can take the singular or combined form of physical (using hands), mechanical (e.g. handcuffs), chemical (using medication) or environmental (e.g. prisons, offenders' institutes and secure hospitals) methods of application. Physical restraint has in a small number of cases been cited as a contributory factor in the death of restrained individuals 3 due to breathing restriction and/or subsequent cardiac stress (‘positional asphyxia’). 7 Given the potential for such fatal consequences, there is a need for scientific evidence upon which restraint guidelines should be based. This review sought to establish the extent of the current scientific evidence in regard to the physiological impact of restraint.
Method
Search terms entered into electronic databases
Each term in the respective column was combined with ‘or’ and the final search resulted from terms ‘cardiovascular response’, ‘position’ and ‘restraint’ being combined with ‘and’
Inclusion criteria
Human studies relating to the physiological consequences of physical restraint.
Exclusion criteria
Duplicate papers and papers not published in English were rejected.
Review method
The title and abstracts of the selected articles were reviewed by two authors (RB, CS) and only articles that matched the review criteria were selected. The selected articles were fully reviewed independently by two authors (RB, CS) with disagreements being arbitrated by the third author (AP), and data were then extracted for this review.
Results
Summary of the physiological effects of restraint position compared with baseline
Effect size (ES) and 95% confidence interval calculated where possible for ventilatory volume measurements, where calculations were not possible the % decrease in volume is shown
FVC, forced vital capacity; FEV1, forced expiratory volume in one second; MVV, maximal voluntary ventilation; HR, heart rate; =, no physiological difference between restraint position and control position; ↓ restraint impaired;↑ restraint improved – physiological function compared with control position
*Seated flexed restraint BMI < 25
†Seated flexed restraint BMI > 25
Not all of the 11 experimental studies found fully reported demographic data. Of the data available, 174 adults (83% male) were studied, with an age range of 18–59 years (mean 28). A range of positions were used to investigate the physiological effect of restraint: ‘hog-tie’
7–10,13,15
(Figure 1a), side lying
10
(Figure 1b), prone using physical holds
12,16
(Figures 1c and d), prone with thoraco-abdominal compression,
11
upright with hands handcuffed either in front or behind the back,
14
weight applied to the torso whilst in prone
11,12,13,15,16
(Figures 1c and e) and flexed sitting
17
(Figure 1f).
Examples of the restraint positions investigated by the current literature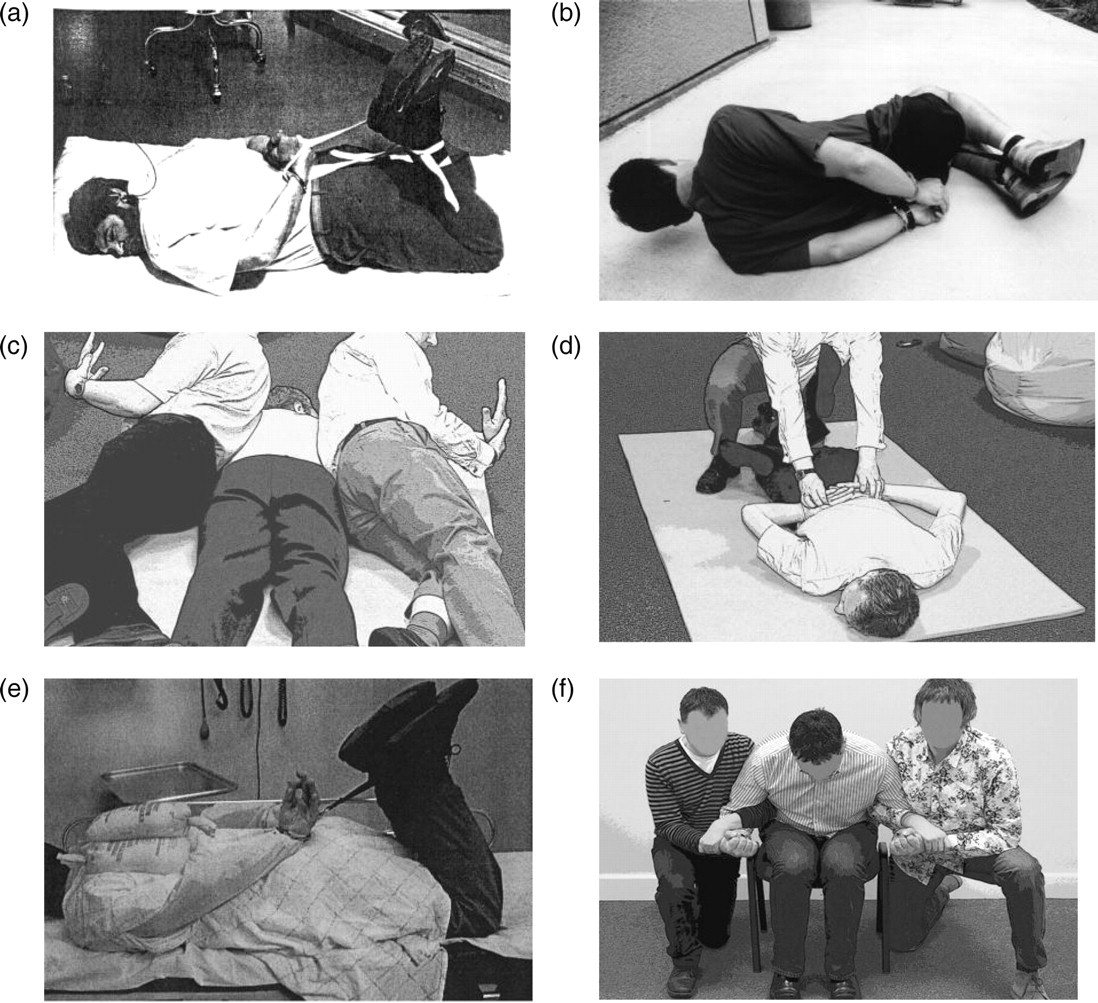
Spirometry was the most common method used to measure the physiological impact of restraint positions. 8,9,11,13,15–17 Forced vital capacity (FVC) and forced expiratory volume (FEV1) reduced by 31% and 35%, respectively in prone restraint with abdominal compression; 11 and by 13.6% and 31% for those with a body mass index (BMI) <25 and by 44.7% and 51% for those with a BMI >25 when restrained in a flexed seated position. 17 No reduction in capacity was seen in upright restraint positions. 8,17 Three studies 9,11,15 measured maximal voluntary ventilation finding that it is reduced by between 23% and 35%. Reductions observed in ventilatory capacity were proportional to the degree of external restriction imposed upon participants either by having weight applied to the back when lying prone, 12,13,15,16 lying prone with abdominal compression, 11 sitting in a flexed position, 17 sitting flexed and being increasingly obese. 17 One study 13 found that a longer duration of hog-tie restraint (5 minutes vs. 1 minute) resulted in a further ≤5.1% decrease in spirometry values. Since spirometry measures were the variable that showed the most dramatic and consistent reduction as a consequence of restraint, we calculated where possible the effect size (ES) and 95% confidence intervals. The percentage reductions given above and the ES calculations of −3.1, −0.8, −0.5 and −1.5 for FVC and −3.9, −1.2, −0.7 and −1.5 8,9,13,16 for FEV1, respectively, and tidal volume ES of −0.4 11 shows the restraint positions investigated can be expected to reduce lung volumes.
Several studies investigated blood gases via indirect measures. Restraint positions caused a slight increase in end expiratory CO2 (etCO2) 8,11,13 (a measure of hypercapnia – excess CO2 in the blood) but not to the clinically significant level of etCO2 ≥45 mmHg indicating hypercapnia. Seven studies investigated the effect of restraint on blood oxygen saturation (SPO2) using pulse oximetry 7–13 with only two reporting that restraint position reduced SpO2 7,10 by as much as 15% and 1%, respectively. Only one study 9 measured blood gases directly (arterial blood) where following four minutes of vigorous cycling blood oxygenation (PO2) increased over 90 seconds of measuring from the post exercise level of 109–114 mmHg, but PCO2 did not differ at any time point.
Heart rate (HR) recovery was measured during restraint and was found to be unaffected by restraint position, 9,10,12,14 although one study 7 observed a 68% mean increase in recovery time following moderate exertion and being placed in the hog-tie position compared with seated recovery.
Two studies investigated the effects of continued struggle during restraint measuring SpO2 and HR. The first study 10 involved running as fast as possible for 250 m, wrestling for 60 seconds and then being placed in a side lying hog-tie position (Figure 1b above) where participants continued to struggle for 30 seconds. Results showed no difference in HR recovery but there was a statistically significant difference in SpO2 between seated recovery and hog-tie–side lying recovery where mean five-minute SpO2 was 97.3 and 96.8, respectively. The second study 15 investigated the extent to which 60 seconds of maximal struggle physiologically stressed the participant. HR response was found to reach 84% of heart rate maximum and O2 consumption reached 40% of maximal capacity (VO2max), values of capacity had been established prior to restraint via a maximal treadmill test.
All of the studies used restraint positions that imposed a restriction to the torso, except one which replicated hand cuffing positions placing the upper limbs either in front of or behind the subject's torso while they performed incremental exercise on a cycle ergometer concluding that limb position did not alter HR or blood lactate response. 14
Discussion
The phenomenon of sudden death during and/or in close proximity to restraint has long been recognized; however the physiological sequelae that leads to death remains poorly understood with a range of possible causes having been identified. 18–23 Causes of death include excited delirium (hyper-arousal), cocaine use, compromised cervical circulation and/or air entry, psychological stress, psychiatric disorder, psychotropic medications (CNS suppression and arrhythmia), anticholinergic medications (tachycardia, hyper-pyrexia) and aspiration causing asphyxia. Case histories also reveal increased numbers of deaths among men aged 30–40 years. The scientific literature has focused on the effect of restraint position on physiological variables using apparently healthy adults free from the effects of drugs, alcohol, medication, physiological and/or psychological pathology meaning they lack ecological validity, although gaining ethical approval for studies with children, and/or those with known risk factors would be extremely difficult to obtain. 4,12
In order to avoid asphyxia a patent airway is required 18 permitting air to be inhaled and exhaled via the action of the diaphragm, ribs and sternum (‘bellows’ mechanism(p 7)). 4 The bellows mechanism raises and lowers intrathoracic pressures by increasing and decreasing internal thoracic volume. The restraint positions investigated imposed a restrictive (external) limitation to ventilation not an obstructive (internal) limitation as measured by the FEV1:FVC ratio. The restraint positions limited the downward excursion of the diaphragm due to the inability of the abdominal contents to displace. This subdiaphragmatic mechanism of limitation was shown most markedly when obese individuals were restrained in a flexed seated position 17 with several subjects reporting an inability to breathe. Limb position was not found to be additive to imposed ventilatory restriction 14,17 due to the restraint positions investigated. The evidence that restraint position can reduce ventilatory function is unequivocal (supported by medium to large negative ES), what is equivocal is to what extent those reductions may prove harmful and in what confluence of circumstances risks may occur in a ‘perfect storm’ scenario.
Metabolic acidosis (low pH due to acid–base balance disruption) has been postulated as a cause of sudden death due to induced cardiac failure where prolonged and/or extremely physically demanding restraint 3,19,20 (particularly so in the presence of cocaine, psychosis or delirium) exceeds the body's physiological capacity for acid buffering. The two studies 10,15 that investigated the effect of struggling during restraint did not clarify the issue of metabolic acidosis; however, they demonstrated the physiologically demanding nature of restraint. Sixty seconds of maximal struggle in the hog-tie position was too much for most participants to sustain 15 and one can only speculate the physiological strain of a prolonged restraint scenario. The second study 10 tried to replicate the ‘real world effort’ of being apprehended and restrained; however, participants were not placed in the prone ‘hog-tie’ position (as they had been in phase 1 of the study), but were placed in side lying, and seated participants did not struggle as the restrained participants had been asked to.
As well as the inability to consume oxygen, 8 the inability to expire CO2 during restraint is critical. Physical exertion increases the production of CO2, and as CO2 levels rise blood pH drops (increased acidosis), with this acidosis stimulating a compensatory increase in respiratory drive to expire the CO2 (respiratory alkalosis). Restraint positions which restrict normal ventilatory function may have a negative impact on the capacity to develop a compensatory respiratory alkalosis. Unfortunately, none of the studies that investigated hypercapnia 8,9,11,13 took measures while participants struggled in restraint. The role of metabolic acidosis in restraint-related adverse events as proffered by Hicks et al. 4 remains unconfirmed by current scientific literature. However, one could speculate that where decreased ventilatory capacity occurs simultaneously with increased intense physiological effort anaerobic energy pathways would be more readily utilized with a concomitant further increase in CO2 production which cannot be readily expired; this scenario could result in a harmful metabolic acidosis.
The single report of increased HR recovery times 7 was at odds with other studies, 8–10,12,14 which may be due to measurement error and/or peculiarities of the 10 subjects measured since one participant reduced their recovery time by 49% in the restraint position while two increased their recovery time by 148% and 469%. The quicker recovery time of values in lying compared with seated are to be expected when subjects remain passive, although what would be of value is to investigate the effect of struggling while in the restraint position. Similarly reporting recovery times over 15 minutes 9 is perhaps not as informative as reporting the effects during the initial minutes of recovery. The last comment on HR is in regard to a study where the two phases of investigation imposed unequal workloads on participants and although HR data were reported in the abstract, this information was not shown in the body of the article; 10 these issues limit the usefulness of the findings.
Risk is inherent in all vigorous physical activity with a death rate of 1:133,869 for men and 1:751,880 for women reported in young adults. 24 The cause of sudden death during vigorous physical exertion is typically related to cardiovascular-respiratory pathology either acquired through lifestyle choices (diabetes, high cholesterol, obesity, hypertension, lung disease) or is genetic, e.g. cardiomyopathy. 24–26 This highlights the need (where possible) for robust screening and risk stratification measures to be applied to those who may be subject to physical restraint in order to reduce the likelihood of adverse consequences.
Conclusion
The scientific literature shows that certain restraint positions can impose a restrictive effect on respiratory function as measured by spirometry, but the effects on other physiological parameters are less clear. The reduction in spirometry measures was proportional to the extent of the restriction imposed by position, increasing weight applied on the torso and increasing obesity in the seated flexed position. The literature did not report that the reductions seen were clinically significant except for Parkes et al. 17 who reported the reductions seen in the flexed seated position with obese individuals were operationally significant. The lack of a clinically significant effect is incongruous with case study history and anecdotal evidence which suggest a link between restraint position and death. Future research should seek to better understand the phenomenon of metabolic acidosis by taking measurements while participants struggle in different restraint positions so as to ascertain which positions and/or techniques of restraint impede physiological function and pose the greatest risk of metabolic acidosis and subsequent dysrhythmia. 3 This future research would be particularly important to understand, in prolonged restraints where fatigue may be induced further increasing the reduction in spirometry measures 13 and/or where there are high levels of physiological arousal (delirium) present. ‘Some, but not all, prone restraint positions cause significant restriction of lung function [and] some restraint positions are demonstrated to present a greater risk than others’ (p. 141). 16 The stresses imposed during restraint (physical, pharmacological, psychological) need to be considered as cumulative with future research seeking to tease out the exact contribution of each element. Future research should also seek to investigate the effect of other restraint positions/techniques on populations other than apparently healthy male adults.
Key finding
Restraint position negatively affects ventilatory and other physiological functions, but to what extent in ‘real world’ restraint situations is unknown.