
Abstract
The authors describe the case of a 28-year-old patient who died from an extensive intracerebral haemorrhage due to disseminated intravascular coagulation (DIC) which occurred a few days after delivery. Access to an emergency department of gynaecology on three separate occasions in the three days preceding hospitalization made judicial evaluation of the case necessary. The case was studied with a methodological approach based on the following steps: (1) examination of clinical records; (2) autopsy; (3) study of the placenta; (4) anatomo-histopathological observations concerning particular organs and structures potentially involved in postpartum maternal death; and (5) evaluation of physicians’ behaviour, in the light of necroscopic findings and a review of the literature. The causes of death most frequently described in the postpartum period were excluded; a mediastinal nodular sclerosing Hodgkin's lymphoma with transdiaphragmatic diffusion, not diagnosed in life, was demonstrated. The cause of death was identified as intracerebral haemorrhage following DIC, Hodgkin's disease and recent delivery by caesarean section. Analysis of the physicians’ conduct, together with a review of the literature, revealed a medical error. However, no causal relationship between the error and the death of the patient was considered to exist. The interest of the case lies in the unusual cause of DIC discussed in relation to a hypothesis of obstetric–gynaecological liability.
Introduction
Disseminated intravascular coagulation (DIC), an acquired haemostatic disease, occurs as a secondary complication of many medical conditions, including sepsis, severe trauma, and solid and haematological malignancies. 1 In obstetrics, the onset of DIC may also result from specific complications such as placental abruption, amniotic fluid embolism, retention of a dead fetus, and pre-eclampsia/eclampsia. 2
The authors report a case of DIC which arose in the course of pregnancy as the first clinical expression of Hodgkin's lymphoma not diagnosed in life. The interest of the case lies in the unusual cause of DIC, discussed in relation to a hypothesis of obstetric–gynaecological liability.
Case report
Clinical documentation
During the 36th week of a normal gestation, a 28-year-old patient, primiparous, complained of non-specific symptoms (swollen legs, asthenia and muscle pain) on accessing an emergency department of gynaecology on 16 January. During examination, blood pressure (127/75 mmHg) and urine tests were normal. Physical examination excluded pathological obstetrical findings (in particular no bleeding) and ended with the prescription of rest, repeated measurements of blood pressure, urine tests, 24-hour proteinuria testing and blood tests to evaluate the coagulation profile and renal and hepatic functions.
The following day, 17 January, due to the persistence of symptoms, the patient returned to hospital. After examination (blood pressure [134/82 mmHg], heart rate [102 bpm] normal cardiotocographic tracing, no abnormal bleeding or proteinuria), the patient was discharged.
On 18 January, there was another access to emergency obstetrics for reported aggravation of the symptoms of the previous days, and the patient reported painful but not rhythmic or intense uterine contractions. Cardiotocography, performed over a recording time of about 35 minutes, was considered normal. The patient had no hypertension or proteinuria. Urine and blood tests were again prescribed, preferably to be carried out the following day. The patient was then again discharged.
At 05:00 in the morning on 19 January, the patient was hospitalized for genital bleeding and the beginning of spontaneous labour. Peripheral oedema was noted, and blood pressure was normal (133/83 mmHg). The cardiotocography tracing was smooth and the placenta showed no signs of abruption, but blood tests revealed coagulopathy with the following values: haemoglobin 115 g/L (normal range [n.r.] 125–150), neutrophilia 21.06 × 109/L (n.r. 1.9–8.0), lactate-dehydrogenase 918 IU/L (n.r. up to 480), alkaline phosphatase 400 IU/L (n.r. 30–120), prothrombin time 18% (n.r. 67–110), international normalized ratio 3.80 (n.r. 1.27–0.90), platelets 163 × 109/L (n.r. 150–400), activated partial thromboplastin time 72.8 seconds (n.r. 26–36), fibrinogen 0.41 g/L (n.r. 2.0–4.0), antithrombin III activity 6% (n.r. 85–120) and D-dimer 21,500 μg/L (n.r. up to 200). Renal and hepatic functions were altered (creatinine 202 umol/L, n.r. 58–86; aspartate aminotransferase 45 IU/L, n.r. up to 31; alanine transaminase 29 IU/L, n.r. up to 34).
Antithrombin III infusion was started at 07:00. Due to the lack of improvement in haematochemical parameters and the onset of signs of acute fetal distress detected by cardiotocography, an urgent Caesarean section was performed at 08.50, with the birth of a healthy baby. A transfusion was given to the mother for blood loss (750 mL) during surgery and after childbirth; she was then transferred for intensive monitoring to the intensive care unit at 10:00. She was treated with packed red blood cells, albumin and fresh frozen plasma; after persistent blood loss and evident cardiovascular and respiratory deterioration, the patient was intubated and underwent an exploratory laparotomy associated with abdominopelvic cleansing and bilateral hypogastric artery ligation (at 04:30 on 20 January). Factor VIIa was administered, and a total quantity of 3000 mL of blood, partially clotted, was aspirated. No specific sources of bleeding were discovered; in particular, there were no signs of bleeding in the breach of the uterus. At the end of the operation, multiple drains were emplaced. Neurological status after the surgical procedure was characterized by an abnormally prolonged reduction of consciousness. For this reason, on 21 January, brain scan, electroencephalography and magnetic resonance imaging were performed but showed no abnormalities. At 11:00 on the morning of 22 January, with fixed dilated pupils, no reaction to pain and absence of trunk reflexes, the patient underwent a brain scan, and an extensive left fronto-parietal haemorrhage, tetraventricular flooding associated with swelling brain and obliteration of the subarachnoid space were detected.
The patient was pronounced dead at 12:00 on 23 January, after ascertainment of irreversible cessation of all brain functions.
Necroscopic findings
Autopsy was performed six days after death. Examination of the brain confirmed the picture described intravitam, with evidence of cerebral oedema (weight 1540 g), subarachnoid haemorrhage spreading with preferential location in the left parietal lobe, subarachnoid microbleeding in the cerebellar hemispheres and massive tetraventricular haemorrhage. In the left frontal lobe, the haemorrhage appeared to dissociate the white matter of the semi-oval centre and the corona radiata extensively, to the point of emerging on the surface at the upper and middle frontal gyrus; large areas of haemorrhage also involved the bilateral ganglia and thalamus, extending to the brainstem and marginally to the cerebellum. Atherosclerotic lesions and/or malformation of cerebral vessels were not found.
Dissection of the thorax showed a firm, voluminous, whitish mediastinal mass (Figure 1) and four swollen lymph nodes (diameter 2 cm).
Mediastinal mass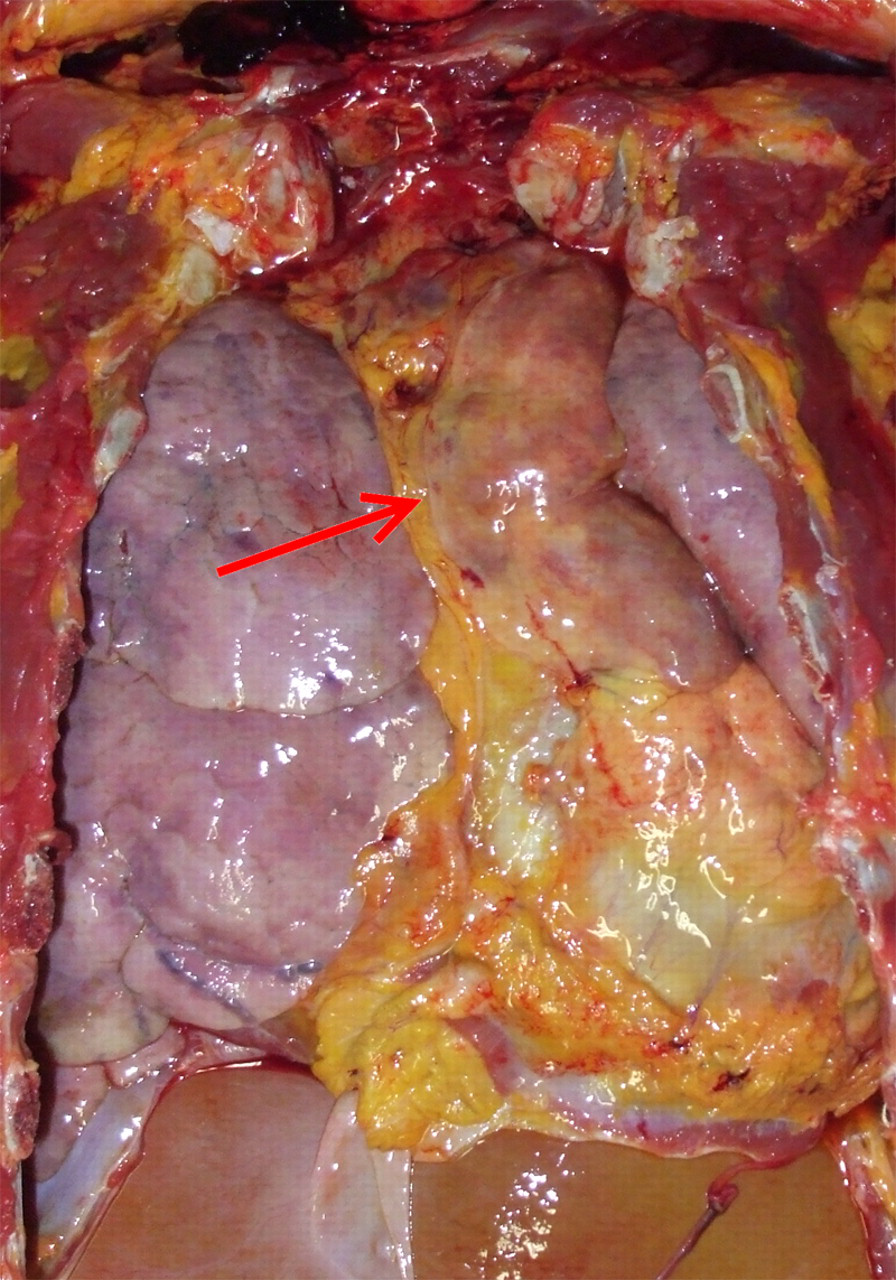
Histological examination revealed a classic Hodgkin's lymphoma, variety: scleronodular (according to World Health Organisation) (Figure 2). Immunohistochemical staining showed that the lymphocytes were positive for CD20, CD3, Reed–Sternberg cells for CD45, CD15 and CD30, negative for epithelial membrane antigen (EMA) with presence of eosinophils. The neoplasm was classified in the third stage, with mediastinal–hilar and sub-diaphragmatic lymph node involvement; Reed–Sternberg cells were observed in spleen sections. Bone marrow examination showed normal myelopoietic and erythropoietic lines.
Histological section of Hodgkin's lymphoma, scleronodular variety. Note: Reed–Sternberg cells (haematoxyline–eosine, ×40)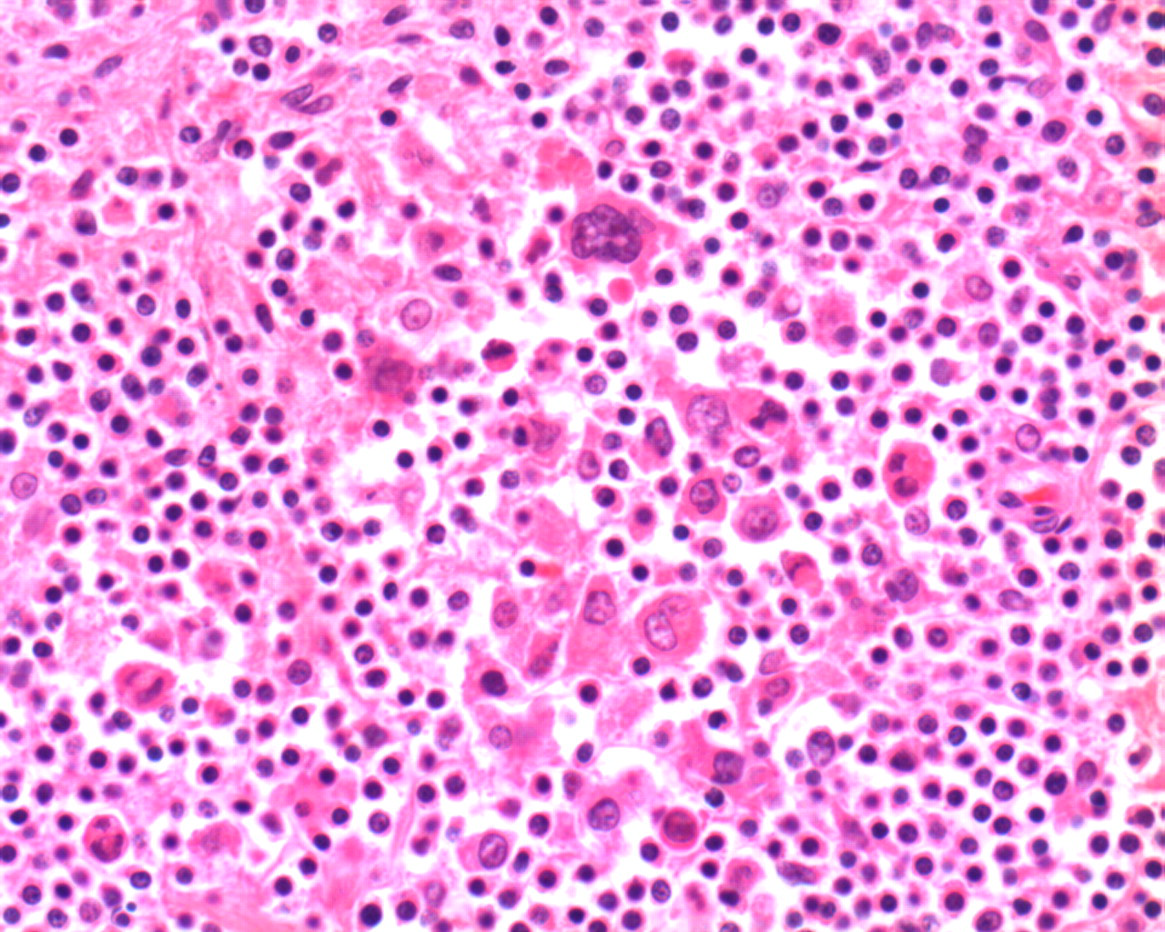
Other findings included oedema and pulmonary congestion, and biliary thrombi in the liver. Thrombi were present in small vessels of the subcutaneous adipose tissue. The kidneys presented a histopathological picture of acute tubular necrosis, with an absence of thrombi in glomerular arterioles and capillaries, and absence of intimal hyperplasia, glomerular necrosis or segmental infarcts. The uterine body showed muscle hypertrophy of pregnancy, areas of congestion and diffuse thrombosis of the uterine vessels.
Histopathological analysis of samples of the placenta showed chronic mild hypoxic injury.
Cause of death
The cause of death was identified as ‘left fronto-parietal haemorrhage, associated with tetraventricular haemorrhage in disseminated intravascular coagulation, Hodgkin's disease scleronodular variety, recent delivery by Caesarean section’.
Discussion
DIC is an acquired disease, characterized by uncontrolled activity of the haemostatic coagulation system, triggered by the release of circulating tissue factor or thromboplastin type substances and/or extended endothelial damage, which initially involves the formation of widespread microthrombi in the microcirculation. With aggravation of the disorder, consumption of platelets, fibrin, clotting factors and the secondary activation of mechanisms of fibrinolysis cause haemorrhages. 3,4 Clinically, various forms may be observed: silent forms, appreciable only by alteration of laboratory tests; forms characterized by thrombotic events, with clinical manifestations depending on damage to the microvasculature (renal dysfunction, respiratory distress, neurological signs, central adrenal insufficiency, peripheral acrocyanosis, gangrenous alteration of fingers, genitals, nose and focal skin necrosis) and/or bleeding (bruising, haematomas, epistaxis, haematuria, digestive bleeding and brain haemorrhages). 1,5
Laboratory tests may confirm the clinical suspicion of DIC showing, in order of frequency, thrombocytopaenia, increased fibrin degradation products (D-dimer), prolonged prothrombin time (PT) and activated partial PT and reduction of fibrinogen. 6 A reduction of antithrombin III and schistocytosis with microangiopathic haemolytic anaemia may also be detected. 6 Owing to postmortem blood degradation, these tests can be performed only in life.
Many diseases may cause DIC, with different clinical manifestations and prognosis. 3 Treatment of this pathology, when possible, is based on arresting the triggering disease. 5 For this reason, it is essential to identify the cause of the coagulopathy as soon as possible.
In the case presented here, the existence of DIC was demonstrated by clinical and necroscopic data, which excluded the causes of maternal death frequently described in the postpartum (postpartum haemorrhage, thromboembolic disease, pre-eclampsia/eclampsia, sepsis and complications related to anaesthesia) 7–11 and highlighted clinical and necroscopic features consistent with a diagnosis of DIC. Diseases in differential diagnosis 3 with DIC, especially haemolytic uremic syndrome and hemolysis, elevated liver enzymes and low platelet count (HELLP) syndrome, were also excluded.
In particular, the HELLP syndrome was excluded for several reasons: from the clinical viewpoint owing to the absence of hypertension and proteinuria and the lack of remission of coagulopathy after delivery; from the laboratory viewpoint owing to the absence, in the initial phase, of thrombocytopaenia, the presence of hypofibrinogenaemia and transaminase levels slightly above normal; and from the histopathological viewpoint, because of the absence of placental abnormalities (decidual arteriopathy, infarcts in the central portion, retroplacentar haematoma or intervillar thrombosis were not found). 12
With regard to the underlying triggering disease, there was no evidence of obstetric complications (placental abruption, amniotic fluid embolism, retention of a dead fetus, pre-eclampsia/eclampsia), which might have explained the DIC. The only possible causative factor was identified, by necroscopic examination, as a third-stage Hodgkin's lymphoma, the role of which in causing coagulopathy was confirmed by the lack of improvement, despite treatment (not aetiological) of that state. This is not surprising, considering that decisive treatment of DIC consists of arresting the triggering factor.
Hodgkin's disease affects between 1/1000 and 1/6000 pregnancies around the age of 30 years, but does not seem to interfere with gestation, nor does pregnancy seem to interfere with the course and prognosis of the disease. 13 However, because of the potential teratogenic effects of diagnostic and therapeutic methods, the best approach to treatment must be evaluated case by case, depending on gestational week, patient's condition and the rapidity of development of the disease. 14
The disease usually begins with a picture of local painless lymphadenopathy, which in most cases involves the lateral cervical, supraclavicular and/or mediastinal lymph nodes and then spreads to adjacent structures and, by means of haematogenous dissemination, to extranodal structures, particularly the spleen, lungs, liver and bone marrow. Only one-third of patients have systemic symptoms characterized by fever, night sweats, itching and weight loss. In the case of major mediastinal impairment, cough or dyspnoea may be present. 14,15
The diagnosis is based on lymph node biopsy. 15 The most frequently diagnosed histological type is the classical variant, subtype nodular sclerosis. 15 In the case presented here, the course of the lymphoma was not characterized by any clinical manifestations preceding the DIC. In particular, there were no detectable superficial enlarged lymph nodes, the mass did not show a mediastinal compression syndrome, and systemic symptoms were not present.
The only symptoms of which the patient initially complained were general malaise, muscle pain and swelling in the legs, which could be considered compatible with a physiological course of pregnancy, in the absence of hypertension and/or proteinuria.
DIC, presenting acutely with abundant vaginal bleeding, changes in laboratory test results, and ending with fatal intracerebral haemorrhage, was the first clinical manifestation of lymphoma. Neoplasia, especially when advanced, predisposes to abnormalities of coagulation. 16,17 Although an unrecognized solid or haematological malignancy as a cause of DIC in pregnancy is rare in the literature (only two cases of the onset of DIC in pregnancy as the first manifestation of metastatic carcinoma of the stomach 18 have been described), after excluding obstetric complications and sepsis, the possibility of a neoplasia should be taken into account in the differential diagnosis.
In the case described, evaluation of the physicians’ conduct revealed a diagnostic error made on 18 January not requesting haemochromocytometric tests, and the consequent possibly erroneous decision not to hospitalize the patient. However, there was no causal relationship between the physicians’ conduct and the death of the patient, because it was not possible either to affirm or to exclude with certainty that a DIC had occurred or was ongoing on the three occasions when the patient was examined prior to hospitalization, and therefore that haemochromocytometric tests could have highlighted pathological changes. It is important to recall that, as DIC is a dynamic process, the results of laboratory tests, and also the patient's clinical condition, may change very rapidly over time. 6
In all probability, even if it had been possible to diagnose DIC and intervene with supportive therapy and Caesarean section on the evening of 18 January, the patient's life could not have been saved, because of the difficulties in diagnosing and treating the pathogenic factor – lymphoma – responsible for DIC in the last few days of gestation.