
Abstract
We report sudden unexpected death in a 35-year-old woman with pregnancy of seven months duration. There was an allegation by the parents of the woman that she was subjected to an assault prior to death. Autopsy examination showed an abdominal pregnancy with a dead fetus, ruptured gestational sac, massive haemorrhage and secondary placental attachment. During her antenatal check-ups, she had persistently complained of abdominal pain and loose stools, but the diagnosis of abdominal pregnancy was missed clinically and on ultrasound scan. In this paper we discuss the diagnostic difficulties and medicolegal issues in such cases.
Introduction
Maternal deaths can occur during and after pregnancy from various obstetric complications and surgical interventions. A forensic pathologist at autopsy will commonly encounter cases of deaths related to pregnancy but abdominal pregnancy is very rare. A variant of ectopic pregnancy, abdominal pregnancy occurs when the ovum is primarily fertilized in the peritoneal cavity. It can also occur when the fertilized ovum secondarily ruptures from a primary tubal, ovarian or uterine pregnancy into the peritoneum. 1 3 This condition is associated with high maternal and fetal mortality. We are reporting sudden death of a woman with an advanced abdominal pregnancy where forensic pathologists have performed the postmortem examination because of alleged physical assault by the spouse.
Case report
A 35-year-old woman, primigravida, with 26 weeks amenorrhoea, complained of sudden pain in abdomen and breathlessness at her home. She was immediately brought to the emergency department where she was pronounced dead. The deceased's parents had alleged that she was assaulted by her husband prior to her death; however, the exact date and time was not known. As per the Indian law, as death was within seven years of marriage, a magisterial inquest was conducted and a medicolegal postmortem examination was conducted.
Clinical history revealed that she had been married for two years and her conception had not been medically assisted. During the course of pregnancy she had complained of repeated pain in the abdomen and loose stools for which she was given antacids and symptomatic treatment. She had regularly visited an antenatal clinic at a government approved centre and her last visit was about 15 days prior to death. There was no bleeding per vagina at any time during her pregnancy or in the period preceding her death. There was no past history of gynecological surgery, pelvic inflammatory disease or tuberculosis. An ultrasound scan of the abdomen was done at about 3 months gestation, which reported a normal pregnancy with a single live fetus (Figure 1).
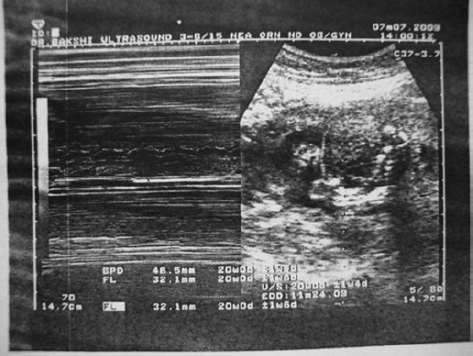
Ultrasound image at three months gestation age
Autopsy report
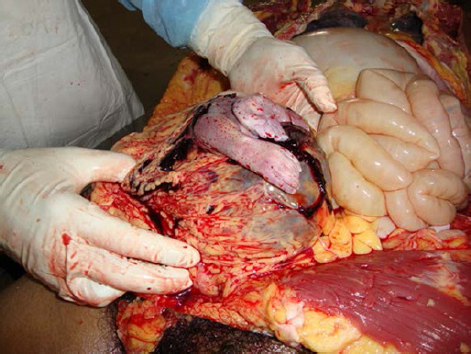
The deceased was a 35-year-old woman, of average built and stature, with obvious distension of the abdomen. Her face and conjunctivae were pale. There was no external injury present over the body. There was no bleeding or discharge per vagina. Upon opening the abdominal cavity, a dark reddish brown mass was seen underlying the transparent peritoneum which was a collection of thick mass of clotted blood overlying the abdominal and pelvic organs (Figure 2). The blood clots weighed 1314 g. On removing the clots, a gestational sac was found lying in the abdominal cavity closely apposed to the mesenteries and mesocolon of the ascending colon and the medial wall of the caecum. A fetus was found partially extruded through a rent in the gestational sac (Figure 3). The placenta was found loosely attached to the posterior and fundal walls of the serosal surface of uterus, which was easily detached from the site of implantation (abruption) (Figure 4). It weighed 320 g and was grossly normal. The uterus was found lying separately in its normal anatomical location below the gestational sac. It was dissected and removed with both the tubes and ovaries. The uterus was of non-gravid size, measuring 10.3 cm × 7.5 cm × 3.8 cm in size and weighed 135 g. On cut section, the myometrium showed slight hypertrophy and an empty endometrial cavity which appeared pale. The fundal and posterior serosal surfaces showed raw areas of denudation, indicating the site of placental attachment. Both the tubes were intact and had no gross evidence of rupture. Ovaries were of normal size and grossly unremarkable. There was no evidence of uteroperitoneal fistula. Pallor of vaginal mucosa was significant and suggested massive blood loss. The cause of death was given as haemorrhagic shock consequent upon bleeding from the placenta (abruption), in a case of advanced intra-abdominal ectopic pregnancy.

Clotted blood in the abdominal cavity
Fetus was found partially extruded through a rent in the gestational sac
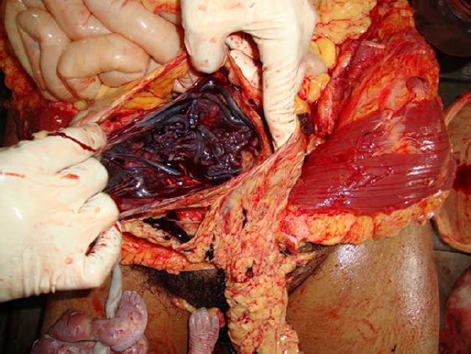
Placenta found loosely attached to the posterior and fundal walls of the serosal surface of the uterus
The gestational sac was opened and the fetus was extracted. It was a dead female fetus of about 26 weeks, with crown heel length of 32 cm, weighing 985 g. Eye lashes were present. Cyanosis was present over the extremities. The skin was reddish in colour, intact and did not show any slipping or loosening. It was stained with vernix caseosa at places. The umbilical cord was pale in appearance, measuring 41 cm in length. There was no sign of maceration. Therefore, it is opined that both mother and fetus died at same time.
Discussion
Abdominal pregnancy accounts for about 1% of ectopic pregnancy.4,5 The incidence of abdominal pregnancy is 10.9 per 100,000 births and 9.2 abdominal pregnancies per 1000 ectopic gestations in the United States. 5 It is a life-threatening condition and is associated with high maternal and fetal mortality, i.e. 4% to 29% and 75% to 95%, respectively. 6 A study by Atrash et al. 5 estimated that the risk of maternal death in abdominal pregnancy is 7.7 times greater than tubal ectopic pregnancy. However, there are cases reported, where the fetus has survived to term and there are chances of both fetal and maternal survival if timely intervention is done. 7 12
In our case, the deceased had developed abdominal pain and breathlessness for which she was taken to a hospital and pronounced dead. These symptoms were due to intra-abdominal bleed and increased intra-abdominal pressure. The deceased had symptoms of pain abdomen, loose stools through most of her pregnancy. These symptoms are seen in abdominal pregnancy during first trimester, though they are non-specific. Other symptoms can be spotting or irregular bleeding, abdominal pain, general discomfort, nausea, vomiting, flatulence, constipation and in some multiparas may state that the pregnancy does not ‘feel right’.4,13,14 It will not be wrong to state that these symptoms were missed by the clinicians during antenatal visit. Such symptoms, though also seen in normal pregnancy, should warn a clinician of a possible abdominal ectopic pregnancy.
An ultrasound scan was conducted at three months gestation, but could not detect the ectopic abdominal pregnancy. Routine ultrasound scans frequently miss the diagnosis of abdominal pregnancy. It is difficult to distinguish between an intrauterine or extrauterine pregnancy, on ultrasound if the gestational sac lies in close proximity to the uterus, within the uterine outline. Though it is helpful in diagnosing tubal and ovarian pregnancy, an abdominal pregnancy is usually missed.13,15 This can be a good defense for radiologists against negligence suits for misdiagnosis.
Other advanced diagnostic procedures and technology have been of little use in cases of abdominal pregnancy. It is reported that trans-vaginal scans can be used to confirm abdominal pregnancy to assess the uterus and establish the continuity between the cervical canal, uterine cavity and gestational sac. 13 In some cases, magnetic resonance imaging has been helpful in diagnosing abdominal pregnancy. 15 Most authors agree that for diagnosis of abdominal pregnancy, the history of risk factors and clinical signs and symptoms play a vital role in early diagnosis that enhances both maternal survival and conservation of reproductive capacity.4,6,13,14
However, in routine practice, especially in developing countries, clinicians rely heavily on their clinical findings rather than the costly imaging techniques. As abdominal pregnancy is such an uncommon entity, it can be missed even by the most skilled physician and the most advanced techniques. Considering its rarity and diagnostic difficulties, a mistake or an error of judgement can be made by a medical practitioner, but when reasonable skill and care have been exercised, will not amount to negligence. We are aiming to raise the awareness of clinicians on the possible occurrence of abdominal pregnancy, the importance of its early diagnosis and prompt management.
At autopsy, careful dissection is needed in diagnosing an abdominal pregnancy. As it is well known that abdominal pregnancies are prone to spontaneous bleeding due to abnormal placental attachment but a prior assault causing or precipitating death should be thoroughly evaluated. An assault could have cause a tear in gestational sac but there were no findings suggestive of physical trauma in this case. As per the investigation, no such assault occurred to the victim. The tear in the gestational sac could have occurred spontaneously. Hence, the role of assault causing the bleeding and death could not be substantiated and was ruled out. However, histology was not performed to date the tear or haemorrhage that could have been more helpful. To determine the primary or secondary nature of abdominal pregnancy, the fallopian tubes, uterus and ovaries should be properly examined to look for sites of primary pregnancy. 2 In this case, both the tubes were intact and had no evidence of rupture, ovaries were normal and there was no gross evidence of any uteroperitoneal fistula. However, in cases of advanced pregnancy, the evidence of a primary site, even if present, may not be appreciated. 2
Conclusions
Abdominal pregnancy is a rare and frequently fatal obstetric condition, which has diagnostic difficulties and therapeutic challenges. Modern image methods used routinely for antenatal check-ups comprise mainly of ultrasound scans which have failed to diagnose an early abdominal pregnancy in many instances or diagnosis occurred in an advanced stage. More advanced techniques like a magnetic resonance imaging is advised only in clinically suspected cases and such facilities are not available in remote communities. The outcome of abdominal pregnancy is mostly grave leading to maternal and fetal mortality. The only means of preventing such fatalities is the awareness and high index of suspicion in cases of pregnancy presenting with any of the clinical clues. Forensic pathologists should conduct thorough postmortem investigation in pregnancy-related deaths to rule out any issues of negligence and assault.