
Abstract
There have been several attempts made to reduce the occurrence of violence in hospital settings, with most professional organizations taking a stance. The impact of violent incidence on the therapeutic environment and the cost in human terms led to the declaration by the World Health Organization that violence is a public health problem. There are strategies for reducing violence that flow out of known trends. We sought to examine the trends in institutional violence in a contextual sense. We reviewed the records of all incidents of violence, categorized by severity, victims and trends over five years in a multilevel secure forensic hospital in Canada. The rate of violence perpetrated by female patients was significantly higher than for male patients. Higher occurrence of violence was recorded in the winter months compared with any other season and was related to unstructured activities. There is a window of opportunity to develop some engaging programmes during the long winter months and improve supervision at all times of unstructured activity. The reasons for increased women perpetration and the winter peak of violence require further investigation.
Introduction
Acts of aggression intended to result in harm or injury do not only have physical, social, sexual and psychological consequences, their direct, indirect or intangible costs are enormous. Health, legal and law enforcements costs related to gunshot wounds, estimated annually at $126 billion in the USA and about a third of that in per capita cost in Canada 1 give an idea of the impact of violence in the community. Premature death, grief, pain, days lost from work and decreased morale and motivation are not easily estimated in intangible cost but add to the costs of disability, injury-related illness and loss of productivity. 2 In adopting the resolution WHA 49.25, the World Health Organization (WHO) estimated 1.6 billion lives are lost per year from violence. As a result, declaring that violence seriously compromises health. The WHO also declared violence to be a public health problem.3,4
Literature review
Broadly defined, aggression, the forceful approaching behaviour with purposeful intent towards others, can manifest unintended consequences that can result in injury.5,6 Injury itself is neither a sufficient nor a necessary condition for aggression but encompasses violence, defined as the physical force used to injure, damage or destroy. These definitions, though imprecise are arrived at by consensus and recognize the graded progression of aggression, the intended attack behaviour and violence, the intense and heinous acts of aggression. 7 To the extent that tools used to measure aggression and violence use similar concepts 8 and their summary scores jointly converted to a graded level of severity and intensity,7,9 it is hardly surprising that the two are synonymous in definition. 5 For this reason, most studies of incidents in health-care institutions employ the all encompassing term violence or violent incidents. 9 17 Aggression is preferred by a few authors18,19 and used synonymous with violence by others.5,7
The relationship between societal levels of violence and the occurrence of violence in institutional settings of psychiatric treatment has attracted the attention of researchers, professional organizations and policy-makers.15-17,20 The finding of a nine-fold rate of postdischarge violence among those with preadmission violence suggests a continuing violence despite the effect of the treatment setting. 16
There is little agreement in the definition,15,21 rates, 22 trends, aetiology, 23 correlates and characteristic predictors of perpetrators and victims 24 27 of inpatient violent incidents. Several reviews have identified the reasons to be due to variations in ascertainment of cases, 19 outcome measures, 28 methodology, rigor and the focus of study.10,11,25 A few consistent themes have emerged on certain diagnostic group of patients,25,29 similar setting of security level, 30 preattack behaviour,31,32 past history of violent episode 12 and impact on staff victims.33,34 There also seem to always be a cluster of a few patients that perpetrate the bulk of violent incidents.12,35
Previous studies have found serious morbidity for patients and staff victims.7,9,36 Injury rates resulting from violence against nursing staff have been estimated and found to be greater than the rates in high-risk occupations like mining and industrial work. 37 Because of the associated high feelings of insecurity in such environments (43%), 11 violence is considered a primary occupational risk factor. 38 Previous studies have outlined some of the characteristics of violence that occur in hospitals that manage general psychiatric patients. There appears to be some difference in the violence that occurs in these settings as compared with the nature, rates and consequences of violence in prison or in forensic hospitals.13,15,39 A recent study of incidents in an adolescent forensic unit reported a high rate of incidents with a peak at the end of the day. The legal status of the perpetrators made no difference to the rates which were directed mostly to Staff. 40 Exploring the contextual aspect of violent incidents has contributed to our understanding of the varied rates and mechanisms of perpetration. In the patient to staff violence, areas of friction, power differential and poor communication are strongly associated with eruption of violence.30,41 Patient to patient violence seems to relate to interpersonal difficulties making prediction challenging.42,43
Reviews of studies of patients in general psychiatric hospitals who perpetrate violence suggest lower rates range between 6% and 20%, with a mean of about 15%12,44,45 than secure units.9,46 Through the study of institutional violence many studies have identified a few patients that perpetrate most violence in inpatient settings.32,35 Within a study of 752 violent incidents, 12% of the 855 patients were responsible for 69% of the incidents. Men with organic brain syndrome and women with personality disorders were reported as being the major perpetrators of these incidents. 7 A similar finding among personality disordered adolescent women was reported recently. 40 Within institutional settings men are known to assault more at the point of admission whereas women assaults occur frequently sometime during their inpatient stay. 10 Some studies have identified meal times, the use of restraints, excessive demands on patients, the presence of students on the ward as particularly higher risk events that aggravate the occurrence of violence.27,47
Seasonal variations
Previous studies of trends and situational differences in psychiatric disorders have been influential in guiding the focus of treatment or intervention. Not only have studies of trends helped the identification of the seasonal pattern of mood disorders for example, such studies have been instrumental in elucidating the neuroendocrinological, neurotransmitter and genetic explanations of mood disorders. 48 Melatonin, for instance, has been implicated in several psychiatric disorders, given to its seasonal manifestation in relation to the length of days.49,50 Although the high rates of suicide occurring in the spring and fall in different studies have not been found to be significantly different from other times, the trend is compelling. The relationship between schizophrenia and influenza is based on a seasonal variation. Some obsessive-compulsive disorders and anorexia 51 are also said to have a seasonal component. 48 The import of seasonality of violence has been linked in patients with Affective Disorders who manifested violent behaviours at specific seasons of the year compared with other diagnoses. 52
The growing interest in the seasonality of violence is evinced by the several studies on the link widely reported from Scandinavian countries, 53 55 the UK 40 and a study involving four continents. 56 The report of the association between seasons and violence is variable, with some finding a positive relationship,53,57,58 and some finding no relationship. 59 In one study, assault, the precursor to homicide was found to follow a seasonal pattern but homicide did not. 60 Explanations for the relationship are anchored on meteorological, environmental, calendar events, sociological and biological models including the findings of the seasonal variation of cholesterol and serotonin metabolism and neurotransmission.53,61,62 The effects of the ozone layer, the presence of increased temperature and air pollution and especially the interval during a 24 hour period during which one is exposed to light (photoperiod) have been extended as potential links in the explanation. Apart from the environmental factors seen as the causes of the seasonal patterns, serotonin known for its relationship to depression, violence, impulsivity and alcoholism, has been implicated because it is affected by the length of day. This length of day, in effect, affects the amount of light and, thus, affects the biological system.51,63 Since the impact of violence is higher, identifying causes and possible associated features that result in violence are important for prediction and prevention.
Contextual violence
Identification of the characteristics of patients or the environment and situational differences that result in violence is important, if preventive efforts are to be successful. Understanding environmental and situational differences are best obtained through the study of the trends of violence. Unfortunately the contextual aspect of violence in institutions that helps complete the picture has received little attention in previous studies.
A 25-year review of the literature of inpatient unit violence was conducted to explore the relevance of relational and cultural factors that could mediate violence. 30 Violence was best conceptualized as a complex interaction involving components contributed by the relational parties and the contextual culture of a setting. Despite the potential of its contribution, it is this later aspect that has been studied less. Recognition of the location, 64 ward design and ambience, 23 atmospheric conditions associated with,65,66 overcrowding 67 and unit specific culture models 68 and multi-layered level 69 of most incidents resemble epidemiological risk factors 70 but lend themselves to better and improved reduction strategies.
The purpose of this study is to describe the pattern and trends of five-year accumulated violent incidents in a multilevel secure forensic inpatient hospital. It is hoped that the pattern identified will be used to institute various unit specific preventive measures. Preventing such violence can be seen as a first step in encouraging management of violence for those being treated in the centre. Their release into the community in the context of these preventive measures will assist in ensuring a safer re-integration in society, thus creating a safer environment.
Methodology
The study was approved by both the institutional Ethics Review Committee and the Regional head quarters of the Correctional Services of Canada which oversees the running of the Regional Psychiatric Center where the study was conducted. The Regional Psychiatric Center is a multilevel secure forensic treatment hospital with 206 beds. It operates under an affiliation agreement with the University of Saskatchewan as a tertiary institution. It admits mentally disordered offenders in the Canadian Prairies. The patients in this psychiatric inpatient centre are federally sentenced Canadian Mentally Disorder Offenders serving more than two years’ sentences for various offenses. There are four different units for the treatment of aggressive, sexual, chronic mental disorder and female offenders, respectively. Incidents reporting for all events are recorded in an observation report sheet. This entails a detailed description of the event leading to the incident, the exact occurrence and the aftermath of the intervention. These incident reports are collected and compiled as institutional infractions record on a database. Training and upgrading is available and mandatory for the staff involved in recording the incidents on the database. Incidents that get recorded usually are serious enough to comprise of a forceful physical aspect. The hospital is staffed by multidisciplinary mental-health professionals, correctional officers and parole officers. The correctional officers are enforcers of dynamic security on the unit. This form of dynamic security ensures that most incidents are reported and recorded. The patients are admitted to this psychiatric hospital from various penal institutions in the Canadian Prairies. This region is notable for its protracted winter period extending from October to April of the next year. The winters are known to record unabating falls of snow and low temperatures at below freezing.
Classification of incidents
After reviewing the recorded incidents, a classification system categorizing the incidents was adopted to include the following:
Mild-consisted of verbal threats or verbal aggression, including physical contact with no injury; Moderate-when property is damaged and mild injury sustained requiring no major intervention; Severe-these violent incidents have resulted in bodily harm that required medical intervention. For instance, significant self-harm or attack with a weapon.
Two research assistants, involved in data collection, conducted a blind pilot recording of the levels of severity of the incidents before categorization. Self-harm was included as a violent incident and classified according to the injuries sustained in line with the classification above. For each of the incident reports various demographic variables and situational factors like use of a weapon were recorded. The location, the time, the day, the month and the activity surrounding the occurrence of the incident were all recorded and transposed into the SPSS version 13.0 for analysis. Descriptive statistics were employed to compare different rates and proportions for possible correlations using t- and z-test.
Results
The patient population at risk of perpetrating violent incidents during the period of study (1996-2000) was 1845. The ratio of men to women during this study period was 15:1. A fifth of the patients (394) (age range 18-81) were involved in perpetrating some violent incident or the other. Although the women were younger, there was no difference in the mean age for the female- and male-violent perpetrators (F = 32.4; M = 35.1). Among the patients that perpetrated violent incidents, the ratio of men to women was 7.5:1. The proportion of male perpetrators (20%) was statistically and significantly lower than the female perpetrators (40%) (P < 0.01).
The moderate incident category (37.1% of the total incidents) was the most frequent form of violent incident. However, it was not significantly different from the mild (35.5%) or the severe (27.4%) forms.
Situational variables
Seventy percent of the incidents occurred at the unstructured leisure time. Weapons were used to perpetrate 28.8% of the total violent incidences. Figure 1 describes the time of day when violence was most likely to occur, with the morning accounting for 21% of the incidents and the evening and afternoon equal at about 40% of the incidents each.
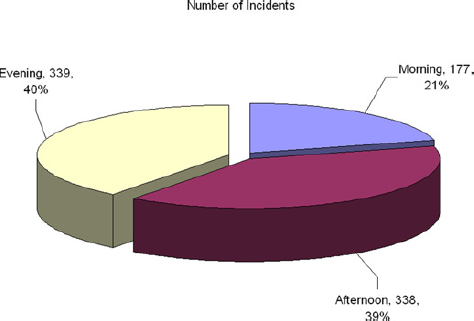
The number and percentage of incident according to time of day
Figure 2 describes the number of incidents during the five years occurring on each day of the week. The incidents were highest on Tuesday with an elevation on Wednesday and Thursday and the weekends tended to record the lowest number of incidents.

Five years average number of violent incidents per day of the week
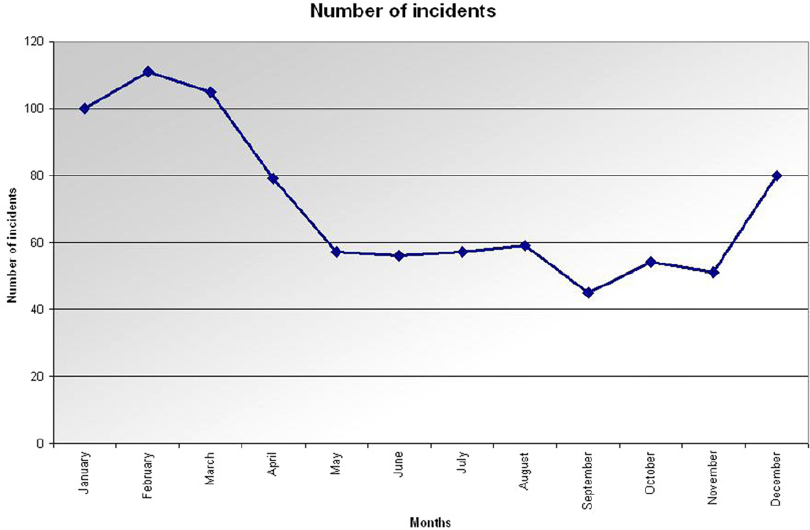
The five-year mean winter incidents (17.8/month) were statistically significantly higher than the spring to summer incidents (10.8/month) (P < 0.05).
The trend displayed in Figures 3 and 4, respectively, depict the monthly variation and average per month of the number of incidents over the five years. The trend leveled off from May to August (spring/summer). There is a fall (autumn) dip at about 45 (5-year total) incidents in the month of September. Beginning from the end of November (winter) there is an increased number of incidents per month and a peak five-year total of 110 incidents in the month of February. This begins to reduce over the next period of months until the beginning of spring in April when the five-year monthly total drops to 80, the same level where they began to rise from in December (winter).

Trend of the violent incidents per month for the five years separately
The five-year total number of incidents averaged per month of the year
With regard to the target of violence the patients constituted 50% of the targets of violence. The rates of violence to self, staff and property were 27%, 17% and 6%, respectively.
Discussion
The seasonal trend and the significantly higher proportion of female perpetrators of violence in a population of mentally disordered offenders in a multilevel secure treatment centre are the main findings of this retrospective study. Our descriptive results of rates and perpetrators bear some similarities and some differences with general hospitals, forensic treatment centres and prison population studies reporting similar variables. The rates of 21% (1/5th of the patients) involved in perpetrating violent incidents is similar to studies completed in general psychiatric hospitals12,17,71 and medium- and high-secure forensic treatment units.32,46 Hospital violence has self-directed targets and staff targets at higher rates than the rates reported in our study.7,24,25 This may reflect the level of psychopathology in which non-forensic units house patients that are out of touch with reality, 35 gender differences bringing out more self harm 72 along with deficits in cognition, coping skills and inappropriate admissions. 71 There are different psychosocial risk factors associated with the risk of violence in different groups of patients along with a mixture of psychopathology and antisocial traits. 73 Some factors like staff job satisfaction, female staff presence, unlocked units and patient voluntariness, commoner in forensic units may combine to protect the attacks against staff.5,74,75 Moreover, the institutional code of behaviour frowns against attacks towards staff members, especially female staff members. The forensic hospital staffed with female nurses benefits from this code of behaviour.
There is a disproportional over-representation of women who perpetrate violent incidents over the men in our study. Previous studies in hospitals point to the identification of more violent behaviours in female inpatients as compared with male inpatients whose violent behaviours occur more during the admission process. 72 Identification of factors that increase the likelihood of female-perpetrated violence is still being studied. Hormonal changes have received some attention. The occurrence of violence during the peri-menstrual period in the context of premenstrual syndrome is worthy of mention, 76 as are psychosocial differences. There may also be other environmental causes that require closer observation. When incarcerated and separated from family members, irritability among women is known to be higher compared with men. 77 Trauma and personality composition have been advanced as mechanisms for violence in women. This could be important in a potentially re-traumatizing environment. 78 The rates of substance abuse and consequent withdrawal symptoms perpetrating the likelihood of violence are equally on the rise among women. Women in forensic settings, similar to the Regional Psychiatric Center are said to manifest higher and more complicated personality characteristics as well as manifest higher rates of self-harm considered in our study as a violent incident. 79 The relevance of a higher rate of childhood sexual abuse among women and its implication in the perpetration of violence is recognized. 80 In a study of 186 female prisoners, reasons for increased aggression included being over-controlled and the hostile manifestation of violence towards close relatives. 81 Women as well as adolescent women are recognized to perpetrate more physical violence separate from self harm.40,72,82
The lower rates of staff assaults or staff victims in our study contrast with a high rate in general psychiatric hospitals 7 and in a medium secure unit. 83 Staff protection from the institution code of behaviour may be in play as well as the increased surveillance and presence of dynamic security staff. Those who work in a high secure unit take more training for protection and the presence of correctional officers on the units of this centre may have some protective value. There were increased violent incidents outside the structured periods of mealtimes, educational and programmed activities. While some studies report that most general hospital violence seems to peak during mealtimes, our results show a low (1%) rate of violence during mealtimes. 84 It is at mealtimes that staff members are in close proximity with the patients. Cutlery is considered a weapon and calls for closer observation and monitoring on the part of the staff. There is a culture whereby settling scores among forensic patients and prisoners including fights that could be classified as a moderate or even severe incident are secretly kept between the parties involved. This may lead to some under-reporting and underestimation of the violent incidents. 85 The use of weapons in 26.8% of the study patients contrasts with lower rate in psychiatric units, for instance, 3-8% in some studies.11,24 Our result may be due to the culture of violence, the antisocial personality, higher rates of paranoid personality disorders and the need to protect self from gang activities, all known to be associated with the acquisition and possession of weapons. 32 Long sentences of incarceration provide for sufficient duration for planning and manufacture of weapons compared with shorter duration of admission in general psychiatric hospitals.
When the days of the week are considered, the weekends appear to be a down time in the manifestation of violence with Fridays and Saturdays having a total rate lower than most other days. The finding of the highest violent frequencies on Tuesdays and Wednesday may not be unconnected with conflicts associated with financial settlement. The patients are paid their weekly stipends on those days. It is possible that settling financial debts especially those that arise from gambling activities, a common occurrence in this setting, may result in disagreement that turn violent. This could not be directly inferred from the observation reports because patients would not reveal the cause of their irritation and incidents in most instances. However, support for this interpersonal based violence comes from the finding of half of the target of violence being the other patients. The lower rate over the weekend may also be as a result of the absence of staff members or the reduced levels of staff members. 86 Unsupportive staff attitudes and friction in miscommunication between staff and patients aggravates violent incidents. 41 As unstructured as the weekend may be, the patients are not involved in the active and usually intensive psychoeducational programmes. These programmes, with their emotion triggering focus and tendencies to uncover past hurt, are known to be a source of stress and disturbed behaviour which could spill over to violent incidents. The patients are allowed to sleep longer, in effect taking it easy and this may account for the lower rates of violence over the weekends. Equally, since there are fewer staff members during the weekend, a reduced level of vigilance is inferred and as such reducing further the detection and reporting of violent incidents over the weekend.
Seasonality
The rate of violent incidents reached its peak in the month of February. This relates to the total frequency per month in the five years under study. This may be linked to the impact of the winter. The winter stretches between the months of November until April. February is conveniently in the middle. There is the likelihood of a feeling of protraction of winter after three months and a delay in the feeling that spring is not forthcoming. This psychological frustration combined with the longer period spent indoors due to the avoidance of the cold on the outside, not only increases overcrowding but can explain some of the irritations that result in the occurrence of more violent incidents. This is particularly relevant for violence emanating in the context of interpersonal conflict. Although there is a difference in the years involved separately, for instance, a higher number of incidents in the month of June in 2000, all the records point to an increased rate from late October to the end of March. This coincides with the period of winter. Apart from the environmental factors described above, biological factors, such as the duration of the photoperiod and its effect on the neural system concerned with aggression, may be at play as reported in other similar studies,.54,87 The length of days, by extension the length of light exposure, is shorter during the winter and its effect on reducing serotonergic neurotransmission may contribute to increased irritability, impulsivity and the resulting violent incidents.88,89 When seasonality is examined in the context of violent suicide, the effect of the circadian rhythm assumes a significant role in the explanation of the association. 90 There have been some differences in the seasons implicated between Northern and Southern Hemispheres. In the study of violent incidents occurring in the seclusion unit of a Finnish forensic psychiatric hospital, most violent incidents occurred between July and August. 53 As well, in a population study of all violent incidents in Norway, May-June registered the highest rates of violent incidents. The authors concluded that ‘the monthly frequency of violence correlated with the absolute value of monthly change in length of day from the previous month. 54 In another Finnish study on homicide and seasons of the year, a lower rate was found during the winter. There are no other similar studies looking specifically on violence to compare with these Scandinavian studies. Although several authors have invoked the role of the length of day and the exposure to light, its relationship to serotonin neurotransmission and consequently its triggering effect on impulsivity,56,58 more studies are still needed to explain the precise reasons for the variation and the hemispheric difference.53,90
The implication of the trend of higher rates of violent incidents during winter is its preventive potential of planning for the causes and averting the incidents. Such plans could include more staff training, monitoring and vigilant observation. The patients could be cued in to be aware of the potential season triggering emotional changes and encouraged to seek help when irritable and stressed. Identification of the patients at an increased risk of perpetrating violent incidents during the winter season could be easier from such awareness training and will help to prevent the occurrence of the incidents. Proactive plans of increasing outdoor activities and increasing the period of structured programmes so that patients are not left without supervision are likely to reduce the frequency of violent incidents. These results suggest the need to study potential biological correlates of violent incidents during the seasons to establish any relationship between the seasons and the incidents of violence.
Limitations
The records in a retrospective study like this cannot be complete due to the secretive nature of violent incidents in a setting with forensic patients. The accuracy of the reporting is also usually in question as patients usually do not reveal the exact incidents and their causes. The numbers used for the calculations may not be precise given that the population at risk may have been variable during the five years. Temperatures used to explain this occurrence were not checked with the meteorological centre to confirm if, indeed, the temperatures were high or low enough. Equally, the lengths of days were not calculated because of the retrospective nature of the study.
Declarations
Footnotes
Acknowledgement
The authors thank Dr Gu Depiang for the statistical support in conceptualization, as well as the Research Unit of the Regional Psychiatric Center for research support in data collection.