
Abstract
Diaphragmatic hernias can be a pitfall for paediatric diagnostics, especially in the cases of late presentation, which can also have medico-legal ramifications as exposed. A three-year-old boy was taken to a children's hospital after an episode of abdominal pain and vomiting of food. A physical examination proved normal, with mild ketonuria being found and he was discharged. Three months later for the same signs and symptoms, he was taken once more to hospital, where he arrived in a state of cardiac arrest and died. A lawsuit was begun against the doctors who had examined him three months earlier. The autopsy found herniation of the abdominal organs into the left pleural cavity through a defect in the left hemidiaphragm. The cause of death was identified as cardiac tamponade caused by mechanical compression of multiple herniated abdominal organs. The histopathological examination revealed marked atelectasis of the left lung, with non-expansion of 60-90% of the alveoli which suggested an acute mechanism that proved fatal, and the doctors were acquitted. The features of this disease and the possible difficulties in its diagnosis highlight the need for the utmost attention in differential diagnosis, even at an age where the discovery of a diaphragmatic hernia is exceedingly rare.
Introduction
Congenital diaphragmatic hernias (CDHs) are protrusions of the abdominal organs into the chest due to the non- or incomplete formation of the diaphragm. The incidence of diaphragmatic defects is between 1/2500 to 1/4000 live births. 1 4 In most subjects, signs are evident at birth, but in some cases (2.6-45.5% of people) 5 they may be delayed with a variety of clinical manifestations interesting respiratory and gastroenteric system. 6 Most cases of diaphragmatic defects involve Bochdalek hernia (85-95%), 1 normally on the left (74-84% versus 14-20% on the right), 7 9 anterior parasternal hernias (Morgani-Larrey hernias) and central hernias (of the transverse septum) have also been described. The defect is rarely bilateral in 1% of cases. 10 The wide spectrum of symptoms characterizing late-presenting Bochdalek hernia explains the difficult of the differential diagnosis that can give rise to possible medicolegal implications. The aetiopathogenesis has been clarified only in part: it is considered to be multifactor, involving faulty embryological development of the diaphragm and genetic factors.11,12 The size of the diaphragmatic defect shows a positive correlation with mortality and morbidity, even with prompt surgical correction. Negative prognostic factors include low gestational age, low birth weight, low Apgar score and concomitant chromosome abnormalities (Turner's syndrome, trisomy 21, 18 and 13).11,13 Many of those affected also present anatomical, nerve, cardiovascular, musculoskeletal, gastrointestinal and urogenital malformations. 8 The authors describe a case of late-presenting hernia that exposed the doctors who have examined the child to medical-legal implications. This case reported is useful to explain rare pediatric situations that can expose to charges of malpractice.
Case report
A caucasian boy aged three years was taken to a paediatric Accident and Emergency (A&E) Department unconscious and in a state of cardiac arrest, where he died shortly after, despite attempts at resuscitation. His parents reported that he had had abdominal pain during the night with an episode of vomiting of food; they had administered paracetamol, domperidone and an antacid. In the morning, he presented breathing difficulties, hypertonia, trismus and subsequent loss of consciousness. He died in the A&E department at 06:50. Three months previously he had been taken to A&E for abdominal pain and cramps in the upper quadrant, with an episode of vomiting of food; he had been discharged without further signs or symptoms with a diagnosis of ketonuria (although tests had revealed only a low level of urinary ketones). Heart, lung and abdominal examinations were normal. Seventeen days before his death an insect sting resulted in palpebral oedema; otherwise, the medical examination carried out at A&E on this occasion revealed no abnormalities. A medicolegal autopsy was ordered by the Magistracy, as it was suggested that death could have been avoided with a correct earlier diagnosis. The cause of death was identified as cardiac tamponade caused by mechanical compression of multiple abdominal organs herniated into the left pleural cavity, due to a probably congenital ipsilateral diaphragmatic defect.
Results
Autopsy results
The cadaver weighed 21 kg, was 109 cm long and was in a good physical and nutritional condition with normal development. The external examination did not reveal any anatomical or other malformations or pathological features. Sectioning of the chest revealed abdominal organs in the left pleural cavity, comprising the entire stomach, part of the transverse colon and the descending colon up to the sigmoid colon, and the upper pole of the spleen (Figure 1). The herniation protruded through an oval defect at the top of the left diaphragm dome; its size was 5.5 cm and its edges rounded and regular without any infiltration of blood. The colour and consistency were uniform over the entire muscle. The ipsilateral lung was flattened in the cavity, pinkish, flaccid, without crepitation. It was significantly reduced in volume with a weight of 70 g. The heart and thymus showed a normal conformation but were displaced in the right pleural cavity. The right lung was regular (weight 180 g) and in its normal position.
Dissection revealing the pleural cavity occupied by abdominal organs (the entire stomach, part of the transverse and descending colon up to the sigmoid colon and the upper pole of the spleen), herniated through an oval defect in the left diaphragm dome
Histopathological investigation
Histopathological examination of the organs was carried out using standard stains (haematoxylin-eosin) and special histochemical stains (Masson's trichrome). Under the optical microscope, the margin of the diaphragmatic lesion showed the morphology and the organization of striated muscle fibres well preserved. The diaphragm was lined on the two upper and lower surfaces and on the margin by a thin layer of fibrous peritoneal tissue with a low cellular component, discrete vascular component and absence of inflammatory infiltrate; the left lung revealed marked atelectasis (Figure 2), producing compression and occlusion of around 60-70% of the alveoli in the upper lobe and 80-90% of those in the lower lobe, with some signs of subpleural emphysema. The final summary reported severe atelectasis caused by compression of the left lung; severe pulmonary oedema; non-specific signs of heart damage (contraction band necrosis) and a defect in the diaphragm wall of about 5.5 cm diameter with intrathoracic herniation of the abdominal organs.
Microscopic view of the left lung with marked atelectasis, causing alveoli compression and occlusion. Marked chronic inflammatory lymphoid infiltrate, presenting as lymphoid follicular hyperplasia. Haematoxylin-eosin, ×100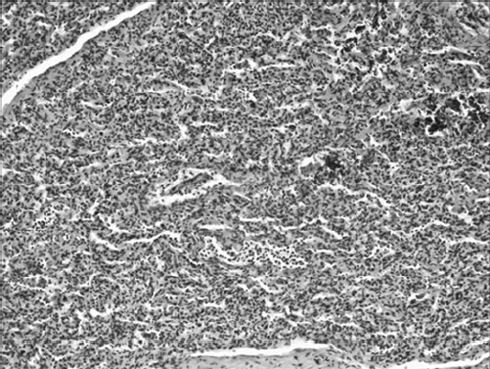
Discussion
The case herein described corresponds to a fatal paediatric diaphragmatic defect of the type of a postero-lateral Bochdalek hernia. The diaphragm develops between the fourth and 12th week of gestation from four different structures: the transverse septum, the pleuroperitoneal membrane, the dorsal mesentery and elements of the rib cage. 14 The factors involved in the diaphragmatic defect include a primary defect in the development of the ipsilateral lung, impaired closure of the pleuroperitoneal canal, impaired myoblast development and impaired innervation by the phrenic nerve. 15 Use of some drugs during pregnancy, such as anti-epileptics, 16 antimycotics 17 and antidepressants, 18 has a significant correlation with fetal diaphragmatic damage. Dietary habits and lifestyle also seem to have an important role. 19 Population studies demonstrate a lower incidence in blacks (-37%) and a greater incidence in pregnancies in women over the age of 35 (+50% in comparison with 20-24-year-olds). 9 In developed areas, survival at birth is over 80%, thanks to the role of prenatal diagnosis and neonatal intensive care. However, in many cases of intrauterine death and voluntary abortion, no postmortem diagnosis is ever made. Intrauterine and perinatal mortality varies between 20% and 70% in different caseloads,2,20 while late mortality from Bochdalek hernia is 8-18%. 21 The defect stems from an abnormality of the posterolateral portion of the diaphragmatic dome to the level of the foramen of Bochdalek, and it is always localized to the left side because such access is obstructed in the right by the liver dome; in fact, the rarity of right diaphragmatic hernia is probably linked to the presence of the liver that ‘buffers’ any breaks in the diaphragm, preventing the subsequent herniation of the viscera. 22 In most cases, respiratory signs of CDH emerge between an hour and a few days after birth. Prolonged compression of the fetal lungs by the herniated organs in the chest impairs lung development and causes pulmonary hypoplasia produced by mechanical compression and non-mechanical factors (embryological and genetic defects), 23 affecting the blood vessels, and persistent pulmonary hypertension, responsible for the high perinatal and neonatal morbidity and mortality. Hypoplastic lungs in CDH present a decreased number of airways, thickened alveolar walls, increased interstitial tissue and markedly diminished alveolar air spaces.24,25 Vascular abnormalities consist of reduced vascular bed and fewer pulmonary vessels, with increased medial and adventitial pulmonary artery thickness and increased arteriole muscularization.14,26-29 Signs, and consequently diagnosis, are delayed in between 5% and 25% of all cases of CDH. In these cases, it is generally discovered by chance, during investigations or surgical procedures carried out for other purposes. These patients are often asymptomatic for long periods or have non-specific signs and symptoms 30 (chronic, acute or even intermittent), erroneously attributed to other paediatric respiratory 31 or cardiocirculatory 32 diseases. CDH may therefore remain unrecognized or not be taken into consideration 33 in differential diagnosis. The anatomical features of late-presenting CDH (absence of hernial sac) are similar to those in subjects showing immediate signs (originating in early gestation); however, hernias diagnosed at a later date are almost never associated with other defects or abnormalities 34 and the finding of pulmonary hypoplasia is inconstant. In cases where previous diagnostic procedures have proved negative, numerous authors consider the hernia to be ‘acquired’, i.e. having occurred at a later time in the presence of a congenital diaphragmatic defect.21,35 The most important cause of chronic or acute signs seems to depend on the type of herniated organ: chronic lung signs are best attributable to protracted mechanical compression of the ipsilateral lung, while acute signs may be due to the rapid displacement of the organs or distension, displacement or torsion of the herniated organs (stomach, intestinal loops). Intermittent signs 36 could be due to recurrent herniation (e.g. due to the temporary cover of the defect by the liver or spleen). 37 In this case, the autopsy showed the partial herniation of a single solid organ, the upper pole of the spleen, which has not undergone any morphological distortion, not being evident in any inflammatory or fibrotic phenomena. The remaining herniated viscera consisting of stomach, transverse colon and descending colon, which are hollow organs with a large elasticity and deformability then hardly subject to distortion of the morphology.
Conclusions
The clinical features, anatomical and histopathological results and clinical course of this case reflect the difficulties involved in the medical management of late-presenting diaphragmatic hernia. The pitfalls involved in these cases can easily lead to medical decisions being contested and may have medicolegal implications. These conditions should thus always be taken into consideration in differential diagnosis in the presence of certain signs, even if non-specific. The features of the case in question account for the diagnostic difficulty and fully justify the non-diagnosis of CDH at the previous visit to the A&E department: the diagnostic formulation was motivated by the finding of nothing but abdominal pain with ketonuria in the context of a normal medical and physical condition. In fact, the performance and very detailed description of the chest and abdominal examinations (both found to be completely normal) were the key elements enabling the expert witness to absolve the doctors of any malpractice and the case to thus be dismissed by the judicial authorities. Although it was claimed that the doctors should have carried out a chest and abdominal X-ray, the deciding element in the expert witness’ evaluation was that a highly sensitive, thorough and expert physical examination had been performed, the results of which gave no indications of any need for an X-ray under those clinical conditions. Furthermore, the finding of pulmonary atelectasis - proof of early herniation and the lack of development of a large part of the lung - suggests the death resulted from a sudden, unpredictable change in the anatomical condition. However, the case was highly significant and is a useful demonstration of situations in which extreme prudence is required on the part of the paediatrician, especially during differential diagnosis, which must be carried out through a careful and thorough analysis of the patient (medical history and physical examination, as full as possible), without forgetting to consider conditions that might be considered uncommon and are not always cited in the main clinical guidelines, in the light of possible legal repercussions.