
Abstract

Pregnancy outcome in women with mechanical prosthetic heart valves treated with enoxaparin
C McLintock MD*, L M E McCowan MD*, C Eagleton MD† and R A North MD PhD*
*University of Auckland; †Middlemore Hospital, Auckland, New Zealand
Background
Pregnancy for women with mechanical heart valves presents a challenging dilemma. Warfarin is the preferred option for maternal health, but for the fetus anticoagulation that does not cross the placenta, such as enoxaparin, is preferable.
Aim
To determine the efficacy and safety of enoxaparin in women with mechanical heart valves during pregnancy.
Methods
Pregnancy outcome data were collated on a prospective (1997–2008) cohort of women with mechanical heart valves managed with enoxaparin ± aspirin. Women were classified as: group 1 enoxaparin commenced by six weeks gestation and continued through pregnancy; group 2 enoxaparin commenced 7–19 weeks; group 3 warfarin → enoxaparin (6–14 weeks) → warfarin or warfarin →enoxaparin ≥ 34 weeks.
Results
Antenatal thrombotic and hemorrhagic complications
*Pregnancies continuing after 12 weeks group 1 n = 14, group 2 n = 12, group 3 n = 11
†TIA = Transient Ischemic Attack, CVA = Cerebral Vascular Accident
‡Antepartum haemorrhage, placental abruption, haematoma, haematemesis
Conclusion
Successful pregnancy can be achieved with therapeutic-dose enoxaparin, with enoxaparin-attributable thrombotic complications in 4.4% of pregnancies and haemorrhagic complications in 17.8%.
Pregnancy outcome in women with antiphospholipid syndrome
Kate Bramham MRCP, Sarah Germain MRCP PhD, Irene Calatayud MD, Beverley Hunt FRCPath MD, Susan Bewley MD, Munther Khamashta MA FRCOG MD and Catherine Nelson-Piercy MA FRCP FRCOG
Lupus Pregnancy Clinic, Guy's and St Thomas' Foundation Trust, London, UK
Background
Pregnant women with antiphospholipid syndrome (APS) may have adverse maternal and fetal outcomes; treatment with aspirin ± low-molecular-weight heparin (LMWH) reduces the risk of adverse outcomes. Systematic review has shown that women with previous thromboembolic events have worse pregnancy outcomes than those with other forms of APS.
Objectives
To assess pregnancy outcome in women with APS treated with aspirin ± LMWH within a multidisciplinary specialized clinic and according to an agreed protocol. To determine whether previous thromboembolism is associated with increased risk of adverse events.
Design
Retrospective analysis of 91 pregnancies in women with a diagnosis of APS made prior to pregnancy.
Results
Pregnancy outcome of 91 pregnancies with APS
SD = standard deviation, SGA = small for gestational age, HELLP = hemolysis, elevated liver function, low platelets
P value = 0.01*
<0.01†
Conclusion
Women with APS have good outcomes in pregnancy when treated with aspirin ± LMWH within a specialized clinic. Women with previous thromboembolism have significantly higher rates of preeclampsia and small for gestational age (SGA) babies than women without previous thromboembolic events. Women with recurrent miscarriages had significantly higher rates of SGA than women with adverse obstetric histories.
What is the best imaging of lower-limb venous thromboembolism in pregnancy?
A Banerjee*, S Clarke †, K Harding †, A McCarthy ‡, G Rottenberg † and C Nelson-Piercy †
*Hammersmith Hospital; †St Thomas' Hospital; ‡Queen Charlotte's Hospital, Hammersmith Hospital, London, UK
Venous thromboembolism (VTE) remains a leading cause of maternal mortality. Doppler-ultrasound is the most convenient and accepted first-line imaging for lower-limb VTE. We report three cases where repeated Doppler-ultrasound was negative, but magnetic resonance imaging (MRI) confirmed the high clinical suspicion of VTE.
A 32-year-old P0 at 22/40 gestation presented with left leg swelling, Doppler-ultrasound found no evidence of VTE. She represented with left-sided back pain radiating down the leg. A second Doppler-ultrasound was inconclusive. MRI-scan confirmed an external and common left iliac vein thrombus.
A 33-year-old P0 presented at 28/40 gestation with back pain. Doppler-ultrasound showed no evidence of VTE. She represented with left leg swelling. Again a Doppler-ultrasound was negative. She represented with increased left leg pain and a further Doppler-ultrasound was negative. MRI-scan confirmed >8 cm thrombus in the left common iliac vein extending to the left external iliac vein.
A 30-year-old P0 presented at 33/40 gestation with left leg swelling. Doppler-ultrasound showed no evidence of VTE. She represented on two further occasions with increased left leg pain and on both occasions Doppler-ultrasound was negative. MRI-scan confirmed expansion and thrombosis of the left femoral vein extending into the pelvis and occluding the left common iliac vein.
These cases highlight the importance of further imaging for lower-limb VTE where the index of suspicion remains high and, though none had any family or personal history of VTE, one case was later found to be lupus-coagulant positive and the other had a rare congenital vascular anomaly.
Medical antecedents of stillbirth in Western Australia
Catherine Douglass MBBS FRACGP DRCOG*†, John P Newnham MD FRCOG FRANZCOG DDU CMFM*†, Adrian Charles MD FRCPA*† and Barry N J Walters FRACP FRANZCOG*†
*The University of Western Australia; †King Edward Memorial Hospital for Women, Western Australia
Aim and Methods
The Perinatal and Infant Mortality Committee of Western Australia (WA) examines and classifies all late-gestation perinatal deaths in WA using the Perinatal Society of Australia and New Zealand Perinatal Death Classification (PSANZ PDC). This study aimed to define the contribution of maternal medical disorders to stillbirth.
In 2000–2001, stillbirths after 31 weeks gestation, and in 2002–2006, the majority after 25 weeks were examined in detail by one of three appointed medical investigators given full access to case-notes and empowered to make further enquiries of treating clinicians. Other cases were coded using limited clinical information (death certificates, midwifery notification forms and autopsy results).
Results
There were 180,808 livebirths and 1327 stillbirths in WA in 2000–2006 (7.3/1000 births). The hierarchical PSANZ PDC requires one ‘principal diagnosis code’. By this system, maternal medical disorders were judged the primary cause of stillbirth in 229 cases (17.3%; 1.3/1000 births), comprising 99 due to antepartum haemorrhage, mostly abruption (7.5%), 74 to hypertension (including preeclampsia and HELLP syndrome 5.6%), 33 to diabetes mellitus (2.5%) and 23 due to ‘other maternal conditions’, including SLE and thrombotic disorders (1.7%). In no case was stillbirth attributed to cholestasis of pregnancy. Further, 27.5% were due to congenital abnormality, 19.5% had no cause found, 12.3% were due to spontaneous preterm birth, 9.1% were attributed to a specific perinatal condition, 6.7% to fetal growth restriction and 4.5% to perinatal infection.
Conclusion
Using the ‘single diagnosis’ PSANZ PDC, 17.3% of stillbirths in WA were attributed to maternal medical disorders.
Venous thromboembolism in pregnancy-risk factors and treatment outcomes in Singaporean women
J Y L Tan MRCP and J George MBBS MRCP
Tan Tock Seng Hospital, Singapore
Aim
To study the risk factors for venous thromboembolism in pregnant Singaporean women and the outcomes of treatment.
Methods
This was a retrospective study based on data collected from the medical records of 20 pregnant women with objectively confirmed deep vein thrombosis (DVT)/pulmonary embolism (PE) 1999–2007.
Results
Of the 20 pregnant women with DVT/PE, 14 (70%) were Chinese, four of 20% were Malay and one (5%) Indian. One woman had previous history of DVT and two had positive family history. Eighteen (90%) women presented antenatally and two of 10% presented postnatally. The majority (17) presented with DVT (predominantly in the left lower limb) and were treated with subcutaneous low-molecular-weight heparin (LMWH). Four women presented with PE–two of whom were treated with thrombolytic, one with intravenous heparin and one with emergency embolectomy.
Complications of treatment with LMWH included cutaneous hypersensitivity reaction and osteopaenia. Pregnancy loss occurred in one woman treated with streptokinase and maternal death in the patient who underwent emergency embolectomy. Identified risk factors included age > 35 years, multiparity, obesity, hyperemesis, ovarian hyperstimulation syndrome, prolonged bed rest, air travel and the presence of thrombophilia.
Conclusion
Important risk factors for venous thromboembolism in pregnant Singaporean women include thrombophilia and obstetric factors such as hyperemesis gravidarum and ovarian hyperstimulation syndrome. Thrombophilia screening should be carried out in pregnant women who develop DVT/PE. Appropriate thromboprophylaxis should be prescribed for women with known obstetric risk factors. Treatment for DVT during pregnancy with subcutaneous LMWH is effective, but may be associated with complications such as hypersensitivity reaction and osteopaenia/osteoporosis.
Venous thrombosis in pregnancy over 25 years in the Scottish population: evidence of benefit from thromboprophylaxis?
I A Greer MD FRCP FRCOP FMedSci*, C Calderwood MBChB MRCOG†, R Dobbie PhD‡ and C Morris PhD‡
*University of York, York; †St John's Hospital; ‡Healthcare Information Group, Edinburgh, UK
Risk factors for VTE
OR = odds ratio; CI = confidence interval; VTE = venous thromboembolism
These data support and quantify known risk factors and the temporal relationship, showing a reduction in risk in recent years, raises the possibility of benefit from routine thromboprophylaxis.
Iliac vein compression during twin gestation: a case report
Meghan Hayes MD, Ghada Bourjeily MD, Courtney A Woodfield MD and Lucia Larson MD
Women and Infants' Hospital and Rhode Island Hospital, The Warren Alpert Medical School of Brown University, Providence, USA
A 30-year-old gravida 2 para 1001 at 26 weeks with twins presented with one day of
severe left pelvic pain without dyspnoea, chest discomfort or leg oedema (Figures
1 and 2). She was a healthy non-smoker without recent travel,
personal or family history of venous thromboembolism. Examination revealed prominent
left vaginal varicosities. Magnetic resonance venogram (MRV) of her pelvis without
gadolinium showed complete extrinsic compression of the left common iliac vein (LCIV)
without demonstrable flow or visualized thrombus. Bilateral leg ultrasound was
negative. Thromboprophylaxis with low-molecular-weight-heparin (LMWH) was initiated.
Pelvic pain resolved. Repeat pelvic MRV in two weeks again found no LCIV flow and new
LCIV expansion suggesting interval intraluminal thrombus. Therapeutic anticoagulation
with LMWH commenced. She delivered vaginally at 36 weeks, induced for growth
restriction of twin A, female, 2350 g with activity, pulse, grimace, appearance, and
respiration (APGAR) 9 and 9; twin B was male, 3090 g with APGAR 9 and 9. Therapeutic
LMWH was resumed postpartum. Dilatation and curettage were performed postpartum day
11 for retained products of conception and persistent vaginal bleeding. She was then
transitioned to warfarin, to complete six months total anticoagulation. Repeat pelvic
MRV six weeks postpartum (Figures 3
and 4) showed left internal iliac vein
(LIIV) occluded 1 cm beyond its origin without acute thrombosis. Repeat pelvic MRV
and magnetic resonance angiogram with gadolinium performed six months after the first
study showed stable LIIV chronic occlusion and mild LCIV extrinsic compression by
right common iliac artery (anatomic variant known as May-Thurner syndrome).
Thrombophilia evaluation was unrevealing. As the patient remained asymptomatic,
further intervention was deferred. Twenty-six weeks gestation – axial unenhanced time-of-flight magnetic
resonance imaging demonstrates extrinsic compression of the left common
iliac vein (arrow) without evidence of thrombus. Patent right common iliac
vein (arrowhead) Twenty-eight weeks gestation – axial unenhanced time-of-flight magnetic
resonance imaging reveals new low signal intensity expansion of the left
common iliac vein (LCIV) with the absence of flow in keeping with interval
development of LCIV thrombus (arrow). Patent right common iliac vein
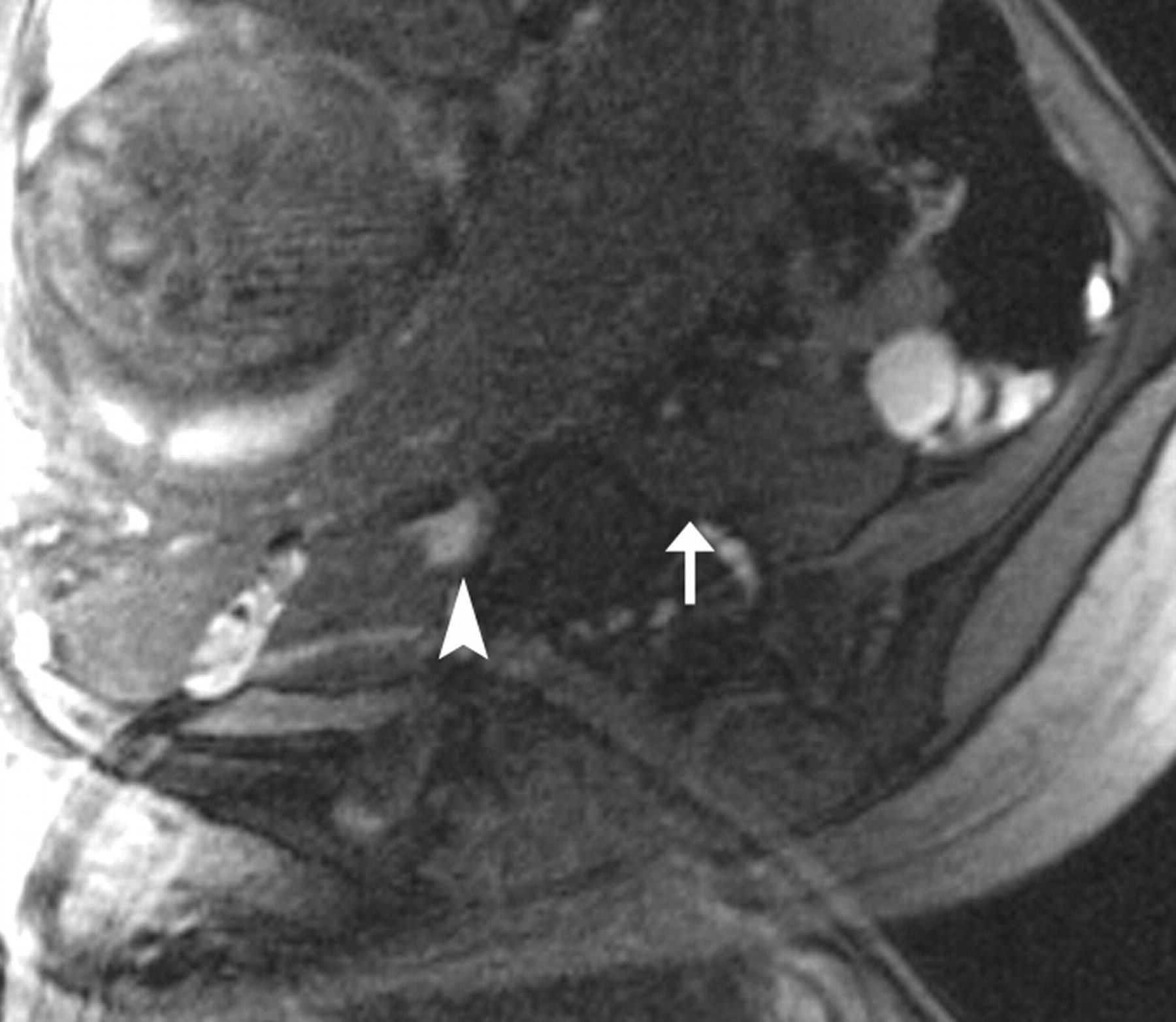
(arrowhead) Six weeks postpartum – axial unenhanced time-of-flight magnetic resonance
imaging shows left internal iliac vein occlusion (arrow), patent right
internal iliac vein (arrowhead) and patent bilateral external iliac veins
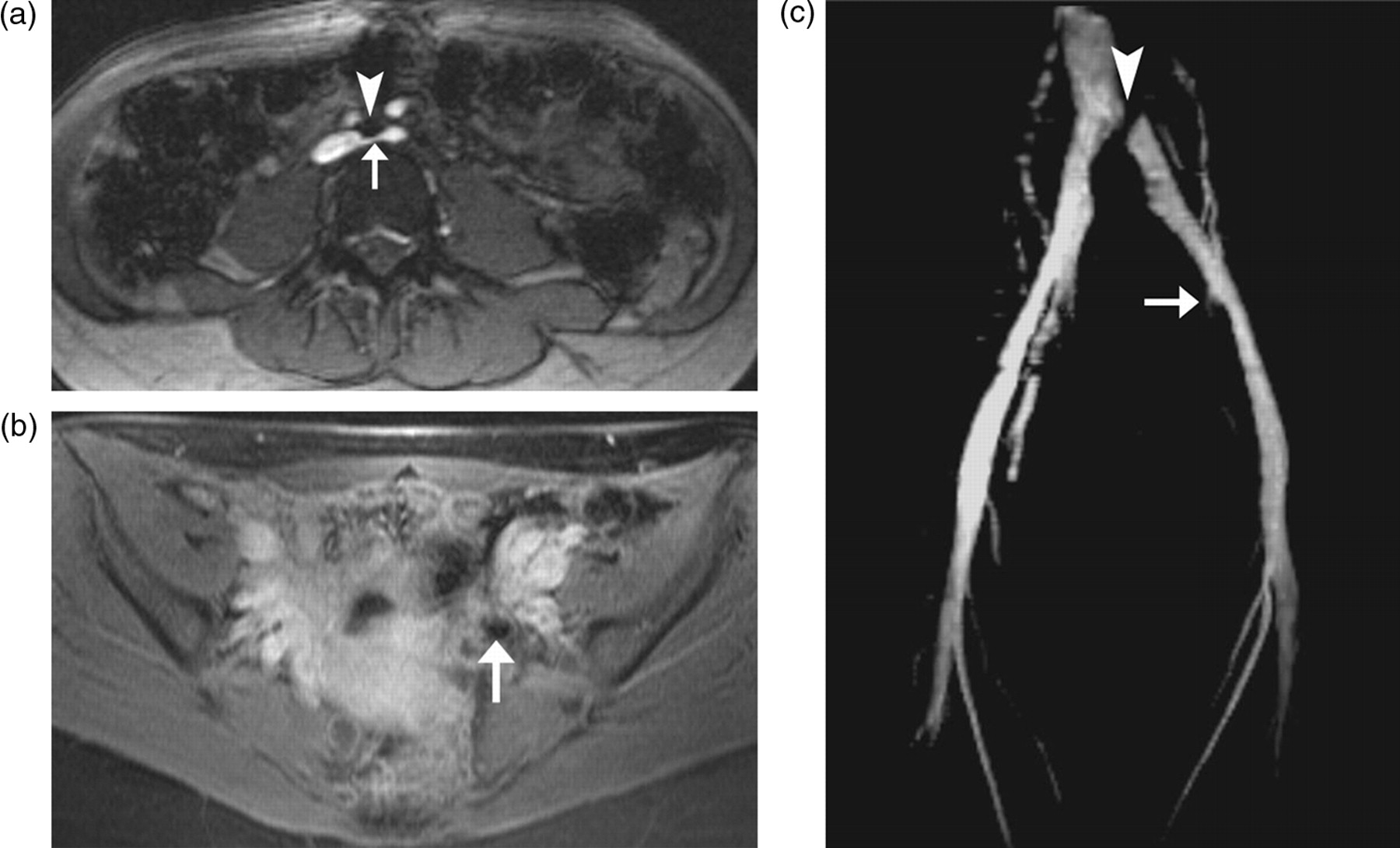
(curved arrows) Six months postpartum – axial unenhanced time-of-flight magnetic resonance
imaging (MRI) (a) demonstrates extrinsic compression of the left common
iliac vein (LCIV) (arrow) by the right common iliac artery (RCIA)
(arrowhead). Axial T1-weighted postcontrast MRI (b) reveals the absence of
left internal iliac vein (LIIV) enhancement due to chronic thrombosis.
Coronal postcontrast maximum intensity projection MRI (c) illustrates both
compression of the LCIV (arrowhead) due to the crossing RCIA and occlusion
of the LIIV just after its origin (arrow)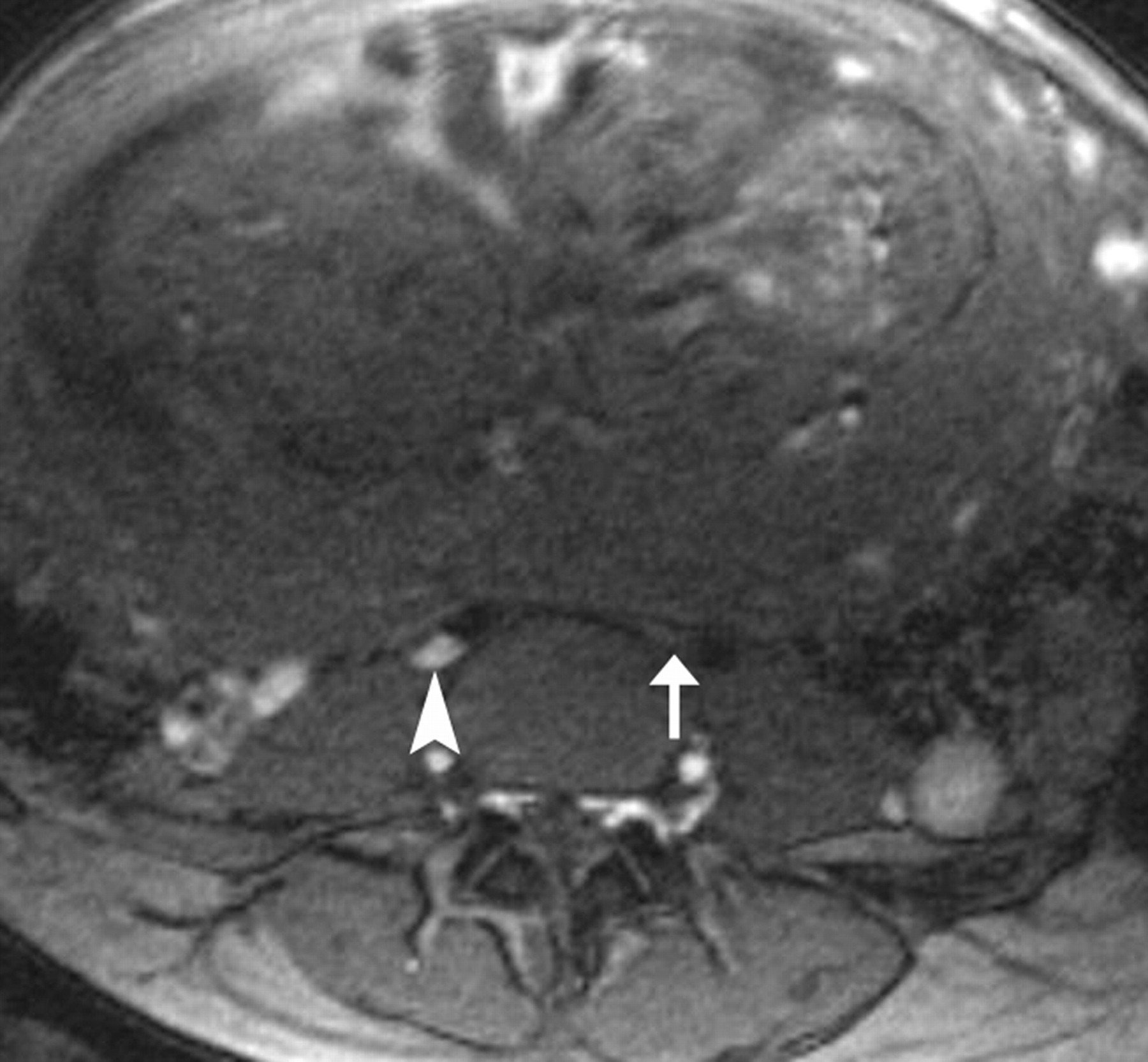

Preeclampsia a prelude to cerebral venous thrombosis
Nageena Mahmood
Corniche Hospital, Abu Dhabi, UAE
Background
Cerebral venous thrombosis is usually seen postnatally in patients with an underlying thrombophilia, no relationship with preeclampsia has previously been reported.
Case 1
A 32-year-old Indian lady who had preeclampsia in her second pregnancy, delivered at term by a vaginal delivery. She was discharged on day five postnatally, re-admitted on day 15 with headache, vomiting and seizures. Cerebral venous thrombosis was diagnosed on computed tomography (CT) brain and anticoagulation commenced.
Case 2
A 32-year-old Mexican-American had four uneventful pregnancies with her first husband. She then had severe early onset preeclampsia in the first pregnancy with her second husband. Had induction of labour and delivered vaginally at 35 weeks gestation. On the second day postnatally, she had severe headache that did not respond to analgesia. Presented to hospital on day 15 with severe headache, right-sided hemiplegia and aphasia, later had seizures. CT revealed an extensive superior sagittal thrombosis with extension into the internal jugular vein. Commenced on enoxaparin and later warfarin.
Case 3
A 30-year-old Indian lady who developed severe early-onset preeclampsia with intrauterine growth restriction requiring termination of pregnancy at 29 weeks of gestation by caesarean section. Presented on day 21 with severe occipital headache and hallucinations, CT scan showed partial occlusion of the posterior two-thirds of the sagittal sinus by a thrombus. Treated with therapeutic doses of enoxaparin.
Conclusion
In all three patients, the thrombophilia screen was negative, but a history of preeclampsia in the index pregnancy was elicited.
Acquired and inherited thrombophilia disorders in formerly preeclamptic women
Robbert Oppenraaij MD*, Durk Berks MD*, Meeke Hoedjes MSc*, Willy Visser MD PhD*, A Franx MD PhD†, Eric Steegers MD PhD* and Johannes Duvekot MD PhD*
*Erasmus Medical Center, Rotterdam; †Saint Elisabeth Hospital, The Netherlands
Introduction
Formerly preeclamptic women are at increased risk of venous thromboembolism. This study was designed to determine the prevalences of acquired and inherited thrombophilia disorders in different clinical subtypes of preeclampsia (PE).
Methods
Three months postpartum the following thrombophilia factors were determined: hereditary factors (factor V Leiden mutation [FVL], factor II mutation [FII], activated-protein C-resistance [APC], protein S deficiency [PS] and protein C deficiency [PC]), antiphospholipid antibodies (lupus anticoagulant activity, anticardiolipin [AC] antibodies and anti-β2 glycoprotein I antibodies) and hyperhomocysteinaemia (HH). If abnormal, except for the genetic factors, tests were repeated three months later. Severity of PE was defined according to American College of Obstetrics and Gynecology (ACOG) criteria (mild or severe), early-onset PE was defined as delivery <34 weeks, intrauterine growth restriction (IUGR) was defined as birth weight below the fifth centile, Hemolysis, elevated liver function, low platelets (HELLP) syndrome was defined as platelet count <100 × 109/L, aspartate aminotransferase = 70 U/L and lactate dehydrogenase = 600 U/L.
Results
A total of 110 women were included: 31 with mild PE and 79 with severe PE. In four women of the mild PE group thrombophilic disorders were found: one heterozygous FVL (3.2%), one APC, one PS, one AC, one FII and one HH. In 22 women of the severe PE group thrombophilic disorders were found: four heterozygous FVL (4.9%), six APC (7.4%), 10 PS (14.8%), one PC (1.2%), nine antiphospholipid syndrome (11.1%) and two HH (2.4%). The prevalence of thrombophilic disorders was higher in the severe PE group compared with the mild PE group (27.8% versus 12.9%, P < 0.05) and in early-onset PE compared with late-onset PE (30.4% versus 16.7%, P < 0.05). Differences in prevalence were found between severe PE in combination with only HELLP (5.9%), severe PE in combination with only IUGR (34.8%, P < 0.05) and severe PE with neither HELLP nor IUGR (30.8%, P = 0.05).
Conclusion
The prevalences of acquired and inherited thrombophilic disorders were higher in women after severe PE and women after early-onset PE. In particular, in women after severe PE in combination with only IUGR, the prevalence of thrombophilic disorders was higher than after severe PE in combination with HELLP without IUGR.
Thrombophilia and pregnancy complications: maternal and fetal outcomes
Alexander Makatsariya MD PhD, Victoria Bitsadze MD PhD, Baimuradova SM MD PhD and Svetlana Akinshina MD
M Sechenov Moscow Medical Academy, USSR
Objectives
To determine genetic thrombophilia, and to evaluate maternal and fetal outcomes in women with history of pregnancy complications receiving preconception treatment.
Material and methods
One hundred and fifty patients with fetal loss syndrome, 56 patients with preeclampsia, 37 patients with venous thromboembolism (VTE), 46 patients with placental abruption and 150 healthy controls were tested to have genetic thrombophilia and antiphospholipid antibodies. Women with a history of pregnancy complications received treatment in the preconception period and during pregnancy, including low-molecular-weight heparin (LMWH) guided by D-dimer, aspirin in low doses, antioxidants, vitamins of B group, folic acid (up to 4 mg in women with hyperhomocysteinaemia and MTHRR C677T).
Results
Thrombophilia was found in 82% women with fetal loss syndrome, in 96.4% women with recurrent preeclampsia and in 100% women with placental abruption and VTE. In women with fetal loss syndrome methylenetetrahydrofolate reductase (MTHFR) C667T, anticardiolipin antibodies, FV Leiden, prothrombin G20210A, multigenic thrombophilia were found in 41.3%, 29.3%, 15.3%, 4% and 20% respectively; in women with preeclampsia, in 44.6%, 16%, 17.8%, 3.6% and 73.2%; in women with placental abruption and VTE in 71%, 25.3%, 25.3%, 37.4% and 96.4%; and in controls in 12%, 4%, 2%, 1.3% and 4% respectively. Prevalence of thrombophilias in study group was higher versus controls (P < 0.05). In the study group nobody had moderate or severe form of preeclampsia, mild preeclampsia was observed in 16%, all babies were alive. Preconception therapy allowed preventing recurrent fetal loss syndrome in 66%; 96% patients were delivered after 37 weeks. Patients did not have recurrence of placental abruption or VTE and all babies were alive.
Conclusion
Thrombophilia might be the main pathogenetic mechanism of recurrent pregnancy complications. Due to thrombophilia involvement in trophoblast invasion and placentation, early treatment is essential. Preconception treatment with LMWH, antioxidants and vitamins allows preventing recurrent pregnancy complications and fetal losses in most cases.
Low–molecular-weight heparin versus no treatment in women with previous severe preeclampsia, FGR <5th percentile, severe placental abruption, stillbirth >20 weeks inherited thrombophilia: a retrospective study
Michael Kupferminc MD, Isca Landsberg MD, Ariel Many MD, Joseph Lessing MD and Eli Rimon MD
Tel Aviv Sourasky Medical Centre, Israel
Objectives
To investigate the effect of low-molecular-weight heparin (LMWH) on adverse outcome in women with thrombophilia and severe pregnancy complications.
Methods
The study included 116 women with history of severe preeclampsia (PET), fetal growth restriction (FGR) ≤5th percentile, severe placental abruption and stillbirth >20 weeks who delivered between the years 2001 and 2006 in our institution, and in whom factor V Leiden or prothrombin mutation or protein S or protein C deficiency were found. All women were referred to our outpatient clinic or for delivery. Our policy is to treat women with previous severe pregnancy complications and thrombophilia with LMWH (enoxaparin) in the following pregnancy. Therefore, women referred to us for follow-up were treated with LMWH starting from weeks 5–15. Women who were referred after 15 weeks were treated, but excluded from the study. Women who were treated with low-dose aspirin were also excluded.
Results
Eighty-seven were treated with LMWH (group A). Twenty-nine women were followed elsewhere and were not treated and were referred only for delivery in our institution (group B). The incidence of severe PET, FGR, stillbirth and placental abruption in previous pregnancies was similar in groups A and B. The incidence of severe PET in the treated group (A) was 4.6% compared with the non-treated group (B) 21%, P = 0.007. Similarly, the incidence of FGR was 2.3% in group A compared with 21% in group B, P = 0.03. The incidence of stillbirth or placental abruption was 0% in group A compared wtih 7% in group B, P = 0.06 for both. The +total incidence of adverse outcome was 7% in group A compared with 55% in group B, P = 0.0001.
Conclusion
In women with severe pregnancy complications and thrombophilias, treatment with LMWH dramatically reduces the rate of recurrence.
Thromboelastometry as an adjunctive test in thrombophilia screening for adverse pregnancy outcome
Leonie Flach, Joris Lenglet, Herman van Geijn and Antoinette Bolte
VU University Medical Centre
Objectives
Thrombophilia has been associated with adverse pregnancy outcome. Thromboelastometry is an easy, rapid and reproducible test that offers the opportunity to investigate all phases of coagulation and fibrinolysis in whole blood. The purpose of this study was to determine if an additional group of women with coagulopathy could be found with the use of thromboelastometry, that are not yet identified with routine thrombophilia screening and that are at risk of adverse pregnancy outcome.
Study design
Included were women that had been referred for routine thrombophilia screening because of their complicated obstetric histories. The routine thrombophilia screening includes testing for protein S, protein C, antithrombin III, activated-protein C resistance, factor V Leiden, prothrombin mutation, antiphospholipid antibodies and methionine loading testing. Thromboelastometry was performed with ROTEM® Gamma (Pentapharm GmbH, München, Deutschland). Studied are the kinetics of clot formation, clotting time, clot formation time and the maximum clot firmness. Screening was done for research purposes.
Results
Eighty-four non-pregnant women with a history of previous severe preeclampsia, Hemolysis, elevated liver function, low platelets (HELLP) syndrome, intrauterine growth restriction, placental abruption, fetal loss and recurrent miscarriage were included. In 27 (31%) women, thrombophilia was diagnosed by routine testing; in this group, 15 women also had abnormal thromboelastometry. In 57 women, no thrombophilia was found; in this group, 32 women had an abnormal thromboelastometry.
Conclusion
Thromboelastrometry does detect a group of women with abnormal coagulation that are not detected by routine thrombophilia screening. Additional studies are warranted to determine if thromboelastometry identifies a subset of women with a prothrombotic tendency that are at an increased risk of recurrent adverse pregnancy outcome.