
Abstract
Cerebral neoplasms are uncommon in pregnancy but should be considered in any pregnant woman with new onset neurological symptoms and signs. We report a case of cerebellar haemangioblastoma presenting in pregnancy and discuss the clinical presentation, diagnosis, surgical management and medical literature surrounding the condition.
CASE
A 33-year-old Angolan woman presented to the antenatal day assessment unit (ADAU) at 28 weeks complaining of dizziness. She worked as a cleaner, was married, a Jehovah's Witness and a French speaker, with limited English vocabulary having arrived in the UK six years previously. Her body mass index was 26 and she had no past medical history of note. This was her fourth pregnancy having had a prior first trimester miscarriage and two uncomplicated spontaneous vaginal deliveries, the last of which was three years previously.
On arrival on the ADAU she reported a 1–2-week history of right-sided headache and neck pain in association with vomiting. Temperature, pulse blood pressure and physical examination were all unremarkable and thyroid function tests were within normal limits. The patient was discharged with a diagnosis of dehydration secondary to vomiting as a result of a presumed urinary tract infection. She re-presented to the ADAU one week later with persistent vomiting, dizziness and epigastric pain when a diagnosis of viral labyrinthitis was presumed. Again temperature, pulse blood pressure and physical examination were unremarkable. However, she was admitted for intravenous rehydration. The following day her symptoms persisted. Closer questioning revealed the dizziness had been present for four weeks with vomiting for two weeks and the headache of gradual onset over the preceding three weeks. There was no history to suggest middle ear disease and she was not on ototoxic medications.
On examination of the central nervous system the visual acuity was noted to be grossly intact, and fundoscopy normal. Pupils were symmetrical, reactive and accommodating. She had impairment of lateral gaze on both sides consistent with bilateral lateral rectus (or VI) palsies. There was no facial weakness or sensory loss and no bulbar signs. Peripheral nervous system examination of the upper and lower limbs was normal and she had down-going plantars. Sensation was normal. Cerebellar examination revealed moderate dysdiadochokinesis of the left hand with mild past pointing. There was marked truncal ataxia, with an unsteady broad based gait. In view of the neurological signs a magnetic resonance imaging (MRI) scan was arranged.
The MRI scan showed a cystic lesion with a peripheral nodule within the cerebellum with no evidence of bleeding, the features being consistent with a haemangioblastoma (Figure 1). Gadolinium was not administered because of the pregnancy. Transfer to an obstetric unit with neurosurgical services on site was arranged. Steroids were given to promote fetal lung maturity in the event of a subsequent premature delivery.
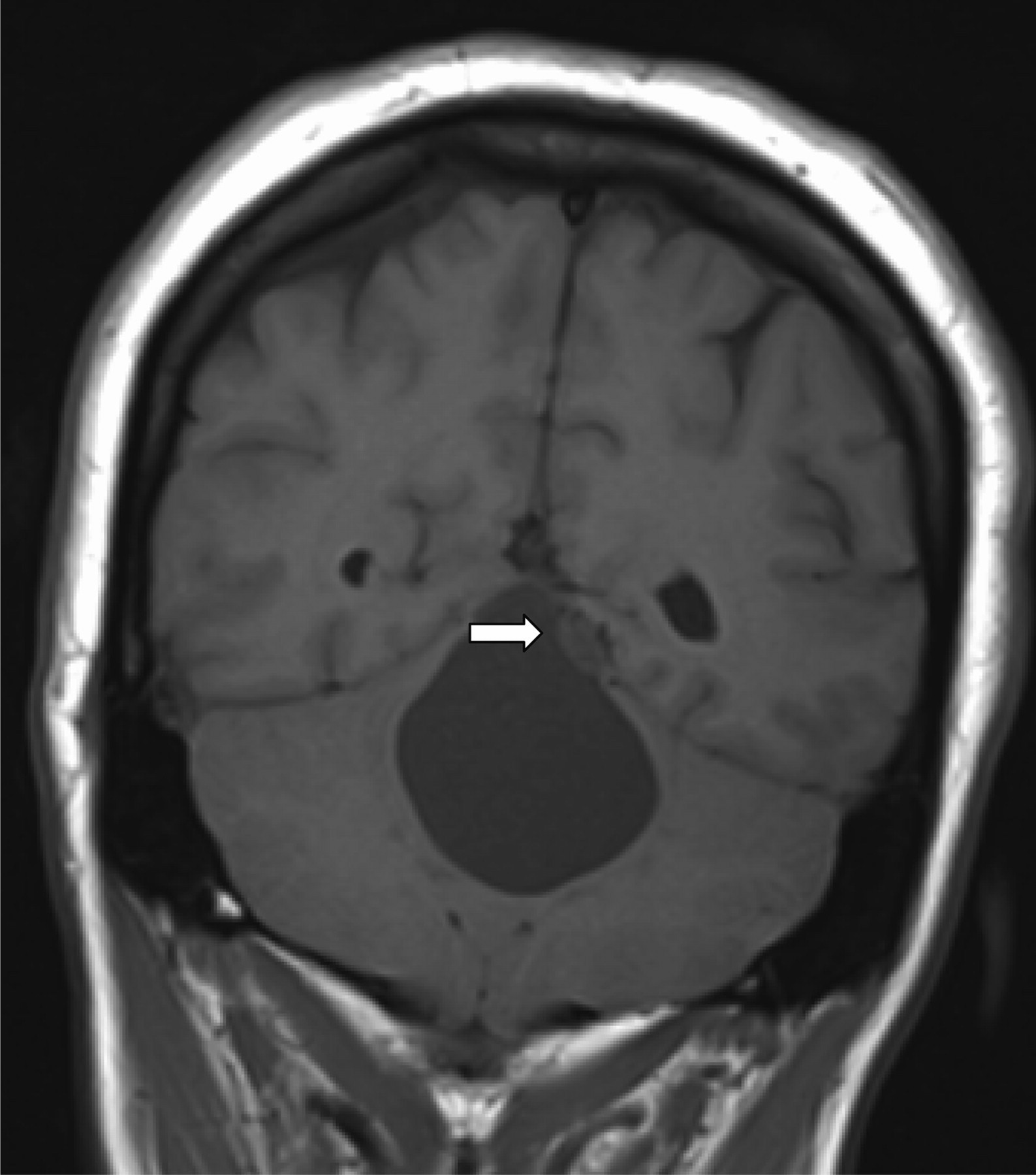
T1 weighted coronal MRI scan showing the large cyst within the cerebellum and the peripheral nodule (arrowed). MRI = magnetic resonance imaging
Following discussions about management options with the patient, a posterior fossa craniectomy was performed under general anaesthetic at 29 weeks gestation. In view of the patient's advance directive regarding objection to blood transfusion, cell saver equipment was available in theatre. The obstetric and neonatal teams were on standby throughout the operation. The procedure was done in the lateral position (right side up) as this was felt optimal in a pregnant patient. The tumour was identified under the tentorium cerebelli. Given the location of the tumour and the position of the patient, long instruments were required to allow safe approach to the tumour. The nodule was resected in total and the cyst drained. There was no significant blood loss. The tumour was confirmed as a haemangioblastoma.
Postoperative recovery was uncomplicated and the patient was discharged home. Ophthalmic screening for concurrent retinal haemangioblastomas was performed and no abnormality detected. Subsequent antenatal care was unremarkable and a male infant 3190 g ultimately delivered at 39 weeks and six days gestation following spontaneous onset of labour. As agreed antenatally, routine management of the second stage was employed. At postnatal review mother and baby were well. An MRI scan six months after the surgery showed complete resection of the tumour (Figure 2). The patient will remain under long-term neurosurgical follow-up.
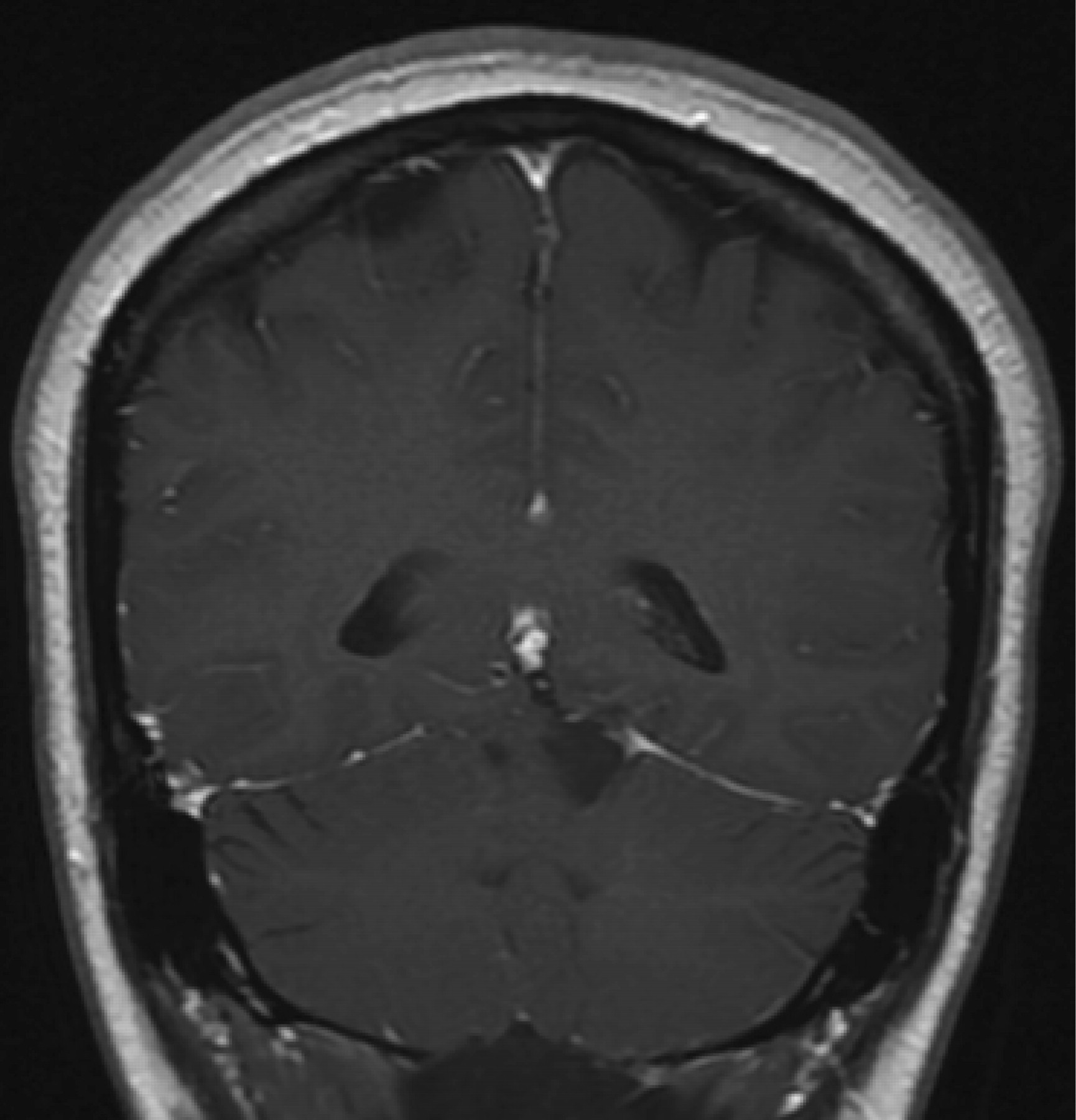
Postoperative T1 weighted enhanced MRI scan showing complete resection of the tumour. MRI = magnetic resonance imaging
DISCUSSION
This case highlights the importance of performing a neurological examination in all cases of persisting headache and/or dizziness during pregnancy. The most remarkable feature in this case was the profound dizziness with instability of gait, readily demonstrated on getting the patient out of bed. Such a manoeuvre is thus an important part of any neurological examination and should not be overlooked. Additionally, the presence of isolated or bilateral lateral rectus palsies in any patient with a headache necessitates urgent imaging to exclude a space-occupying lesion causing direct compression. This abnormality is most commonly characterized as a false localizing sign and is frequently seen in the setting of raised intracranial pressure from intracranial tumours, venous sinus thrombosis or in idiopathic intracranial hypertension. 1
The language barrier may have contributed some difficulty in eliciting a thorough history highlighting the importance of a thorough clinical assessment and the need for 24 hour interpreting services.
The literature concerning pregnancy and intracranial neoplasms consists largely of case reports, or case series epidemiological analyses. 2 An epidemiological analysis performed in Germany of all tumours notified through the German Democratic Reporting System 1961–1975 suggested a frequency of 3.6 per 106 births which is slightly lower than the background frequency. Of the 29 tumours reported, astrocytoma (9 cases) and glioblastomas (6 cases) were the more frequently observed tumours. 2
Haemangioblastomas comprise 1–2% of all intracranial tumours 3 and 7–12% of posterior fossa neoplasms. 3 They often occur sporadically; however, 20–40% of cases occur in association with von Hippell–Lindau disease (VHL). 3,4 VHL is inherited in an autosomal dominant fashion and arises secondary to a mutation in the VHL tumour suppressor gene involved in cell cycle regulation and angiogenesis. 5 The incidence is one in 35,000–65,000. 6 Haemangioblastomas may occur at various sites within the central nervous system although the cerebellum is the commonest location. The condition may also be associated with renal cell carcinoma, phaeochromocytoma, pancreas and endolymph tumours. Retinal haemangioblastomas also called retinal capillary haemangiomas are the earliest and most common manifestation and are found in 57% of those with VHL at a mean age of 25 years. 3 Cerebellar haemangioblastomas are seen in 30–50% of VHL with a mean age of 29 years 3 and originate from maldevelopment of the vascular portion of the mesenchyme destined to form the choroid plexus of the fourth ventricle and incorporated into the cerebellar tissue during early life. 3 Given the high prevalence of VHL in women with haemangioblastomas, all such women should be screened for tumours at other sites. Following surgery our case underwent screening for retinal disease. However in the absence of symptoms suggestive of tumours elsewhere, it seems likely that the haemangioblastoma in this case was sporadic. The current clinical diagnosis of VHL disease demands at least one VHL manifestation in a patient with familial VHL disease. In the absence of a positive VHL family history, a diagnosis of VHL can be concluded with at least two retinal, spinal or cerebellar haemangioblastomas or with a single haemangioblastoma in combination with a typical visceral lesion. 7 The VHL gene on the short arm of chromosome 3 has been cloned and pre-symptomatic diagnosis of VHL patients is now possible with mutation analysis. 7 Germline mutations of all types are scattered over the VHL gene and include gene deletions. They may be inherited or sporadic. 8 Hes et al. 8 studied the occurrence of VHL mutations in patients and families who either did or did not meet the above-mentioned clinical criteria for VHL disease. Of the 146 patients studied, there were 43 cases not meeting VHL diagnostic criteria but with a solitary cerebellar and spinal hemangioblastoma. Only 1/43 (2.3%) had an identified mutation in the VHL gene. 8 Evidence for the benefit of genetic screening in those not meeting the current clinical criteria for diagnosis of VHL is thus lacking. A pragmatic approach may be to screen those with a haemangioblastoma for lesions at other sites and those who thus meet the criteria for VHL should undergo genetic testing for VHL along with their family members.
There are several case reports of haemangioblastomas worsening or being diagnosed in pregnancy. Most of these reports relate to tumours in association with VHL and therefore report the inherent complexities of managing women with recurrent or multiple haemangioblastomas often at several sites. It is not clear whether the complications seen in these women can be extrapolated to women with isolated haemangioblastomas without VHL. However, several report these tumours may worsen or present for the first time in pregnancy. 3,4 Expansion of the tumour vascular bed, increases in blood volume or altered hormonal milieu 3,9 are all suggested mechanisms. Progesterone receptors have been identified in cerebellar haemangioblastomas 10 and if confirmed may provide an explanation for the predominance in female patients and their rapid growth in pregnancy. Case reports discussing haemangioblastomas in pregnancy are shown in Table 1. Headache with associated dizziness is a consistent feature in the majority of cases. Naidoo et al. report a woman with two cerebellar lesions presenting with symptoms in early pregnancy. One obstructing tumour was resected to relieve hydrocephalus, and the remaining smaller tumour was left in situ. As pregnancy progressed the remaining tumour became symptomatic as it increased in size and was managed medically with steroids. Following delivery symptoms resolved and computed tomography confirmed a reduction in size of the cerebellar tumour. 4 The authors conclude that the observed resolution was facilitated by a return to the non-pregnant state and provides an interesting insight into the possible effects of pregnancy on these tumours. 4 Surgery however remains the first-line treatment for symptomatic cerebellar haemangioblastoma with total excision anticipated to provide a cure. 9 There is a reported 3–10% recurrence rate after resection and long-term follow-up for these patients is therefore advised. 5 The progress of asymptomatic haemangioblastomas in pregnancy is more difficult to determine from the literature. Grimbert et al. looked retrospectively at 56 pregnancies in 30 women with VHL of whom four had central nervous system haemangioblastomas. Three out of 56 women developed symptoms associated with disease progression of which one was in relation to a cerebellar haemangioblastoma causing raised intracranial pressure and resulting in caesarean section at 32 weeks gestation followed by surgical correction. 11 While conservative management may be appropriate for asymptomatic cases, the appropriateness of such an approach as outlined in the case report of Naidoo et al. 4 is likely to depend on the size, site, symptoms and any mass or raised intracranial pressure effect and after careful discussion between managing clinicians and the patient.
Case reports discussing haemangioblastoma in pregnancy
HB = haemangioblastoma; CS = caesarean section; VP = ventricular-peritoneal
CONCLUSION
Cerebellar haemangioblastomas are a rare but important diagnosis in pregnancy and may present with headache and dizziness. Language barriers should not deter the careful and thorough examination required in all cases presenting with such symptoms.