
Abstract
Seventy-three pregnancies in 43 women with SPK have now been described by the US National Transplantation Pregnancy Registry (NTPR) (established in 1991), which contains self-reported data from questionnaires and hospital records. These women have high rates of complications despite normoglycaemia and restoration of renal function. We describe the pregnancies of three SPK recipients in the UK managed in joint renal obstetric clinics and discuss the antenatal and postnatal complications specific to SPK transplants.
CASE 1
A 36-year-old Caucasian woman presented at seven weeks gestation in her first pregnancy. Four years earlier she had a simultaneous pancreas–kidney transplant (SPK) for type 1 diabetes and nephropathy with pancreatico-duodenal anastomosis to the small bowel. Initial immunosuppression included tacrolimus and mycophenolate mofetil (MMF) but sirolimus was started following neutropenia secondary to MMF. The pregnancy was unplanned. Prior to pregnancy laboratory markers were as follows: serum creatinine (Cr) 110 µmol/L (estimated Glomerular Filtration Rate [eGFR] 52 mL/minute/1.73 m2), HbA1C 5.1% and serum amylase 58 µmol/L. Atorvastatin and lansoprazole were discontinued and immunosuppression was left unchanged (tacrolimus 3 mg twice daily and sirolimus 1 mg once daily). She continued taking aspirin 75 mg once daily, which she had been taking since transplantation. She was counselled about the unknown risks of sirolimus in pregnancy and relative safety of tacrolimus. Following discontinuation of lansoprazole she developed heartburn and was prescribed gaviscon and ranitidine.
She was normotensive and protein:creatinine ratios (PCR) (65 mg/mmol Cr) remained stable throughout the pregnancy. Tacrolimus was sequentially increased to 5 mg twice daily between 13 and 23 weeks gestation because levels were repeatedly low (2.7–5.8 ng/mL). She had a normal glucose tolerance test at 27 weeks. Sirolimus levels were adequate (1.5–3.0 ng/mL). Serum Cr initially fell to 80 µmol at 13 weeks but increased to 114 µmol/L at 34 weeks gestation. An ultrasound of the allograft excluded obstruction and Cr peaked at 121 µmol/L at 35 weeks. Fetal ultrasound showed normal fetal growth. An elective caesarean section with Pfannensteil incision was performed at 37 + 1 weeks when Cr was 95 µmol. A 2594 g male infant was delivered (Apgar scores at 1, 5 and 10 minutes: 8, 8 and 10) and fetal arterial and venous cord blood were 7.255 and 7.326, respectively. The baby was transferred to the neonatal unit for temporary non-invasive ventilation. Good perfusion of the maternal kidney and pancreas allografts was demonstrated on ultrasound postpartum. Serum Cr postpartum was 103 µmol/L and amylase 59 µmol/L. She was discharged home with the baby on day 4 and received thromboprophylaxis with enoxaparin (40 mg once daily) for 10 days. Most recent serum Cr is 107 µmol/L (eGFR 58 mL/minute/1.73 m2) at 16 weeks postpartum.
CASE 2
A 29-year-old Caucasian woman with type 1 diabetes developed end-stage renal failure following an episode of meningococcal septicaemia. She received peritoneal dialysis for two years, then underwent a SPK transplant with a pancreatic duodenocystostomy, following which she had three episodes of acute rejection while taking tacrolimus, azathioprine and prednisolone, all of which were successfully treated with methyl prednisolone. She also developed Epstein–Barr associated post-transplant lymphoproliferative disease at one year; azathioprine was discontinued and tacrolimus dose reduced. After three years MMF was introduced, due to a progressive increase in Cr and presumed chronic allograft nephropathy, to allow a reduction in the dose of calcineurin inhibitor. Following prepregnancy counselling and prior to conception, MMF was changed back to azathioprine (100 mg once daily) and she continued to take tacrolimus (2 mg twice daily) and prednisolone (5 mg once daily). Prepregnancy serum Cr levels were 85 µmol/L (eGFR 73 mL/minute/1.73 m2).
She became pregnant 10 years after her SPK transplant and her modified immunosuppression regimen was continued. She was also taking sodium bicarbonate (1.5 g am 3.5 g pm) and had commenced calcium carbonate/cholecalciferol and ferrous sulphate supplements. Tacrolimus was increased at 16 weeks (3 mg twice daily), 30 weeks (4 mg twice daily) and 32 weeks (4 mg/5 mg twice daily alternate days) because levels were repeatedly low (3 ng/mL), in order to maintain adequate immunosuppression (levels 4–6 ng/mL). Glucose tolerance tests were performed at 19 and 28 weeks to exclude gestational diabetes and were normal; HbA1C was 5.0%.
Uterine artery Doppler waveform at 22 weeks gestation showed a notch in the left uterine artery and increased resistance index and therefore aspirin (75 mg once daily) was commenced. She remained normotensive throughout the pregnancy but PCR increased from 76 to 114 mg/µmol at 24 weeks. Leukocytes were present in the urine throughout the pregnancy. At 30 weeks Cr increased to 101 µmol/L and by 33 + 3 weeks had reached 145 µmol/L. She was admitted, received betamethasone for fetal lung maturation and labour was induced (2 mg prostin E2 gel, artificial rupture of membranes at 24 hours and Syntocin at 28 hours with epidural analgesia). She had a low cavity forceps delivery of a healthy male baby weighing 2160 g (Apgar scores at 1 and 5 minutes: 8 and 9 and venous cord blood pH 7.20).
An episiotomy extended into a third degree perineal tear that was sutured. Postpartum haemoglobin fell to 6.1 g and 3 units of packed red cells were transfused. Serum Cr peaked at 213 µmol/L prior to delivery but subsequently fell to 153 µmol/L postpartum, but on day 3 rapidly increased again to 455 µmol/L with pelvi-caliceal dilation of the allograft and 1.2 L of urine retained in the bladder on ultrasound examination. A catheter was inserted with gentamicin prophylaxis and renal function recovered to 183 µmol/L. She was discharged home with an indwelling catheter and the baby on day 6. Postpartum tacrolimus levels were 7–9 ng/mL and tacrolimus dose was reduced to 4 mg twice daily.
The urinary catheter was finally removed after three weeks following an initial failed attempt. Urinary retention was thought to be due to neuropathy secondary to diabetes because she had suffered problems with micturition prior to the pregnancy. Six weeks postpartum she was readmitted with a potassium level of 6.8 mmol/L, Cr 223 µmol/L and a tacrolimus level of 8 ng/mL. Ultrasound of the graft showed no evidence of hydronephrosis, hyperkalaemia was corrected with insulin and dextrose, her tacrolimus dose was reduced to 4 mg twice daily, azathioprine was stopped and MMF was restarted (500 mg am and 250 mg pm) after discussion about discontinuation of breast-feeding.
Despite these measures, after a few days Cr remained elevated at 220 µmol/L and a biopsy was performed, which showed evidence of acute tubular necrosis with focal calcification and possible evidence of calcineurin toxicity. Tacrolimus dose was reduced further to 3 mg twice daily and MMF was increased to 500 mg twice daily. She was diagnosed with a Pseudomonas aeruginosa urinary tract infection, which was successfully treated with ciprofloxacin 500 mg twice daily for one week. Subsequently, her Cr gradually fell and is 128 µmol/L (eGFR 43 mL/minute/1.73 m2) at 18 weeks postpartum.
CASE 3
A 33-year-old Caucasian woman had a SPK with pancreatico-duodenocystostomy one year prior to a planned first pregnancy. Prepregnancy Cr was 109 µmol/L and during early pregnancy remained at the same level. Immunosuppression was unchanged: tacrolimus (3 mg twice daily), azathioprine (100 mg once daily) and prednisolone (5 mg). She was also taking isoniazid (100 mg) and pyridoxine (12.5 mg), for tuberculosis prophylaxis (diagnosed and treated aged 20), ranitidine (150 mg twice daily), folic acid (400 μg once daily), sodium bicarbonate (4.2 g four times a day) and ferrous sulphate (200 mg once daily).
From 16 weeks gestation she developed recurrent Escherichia coli and pseudomonas pyelonephritis, which was treated with combinations of ceftazidime, gentamicin, co-amoxiclav or cefadroxil and later nitrofurantoin and single agent prophylaxis between infections. Several ultrasound examinations of the renal allograft showed dilation of the pelvicalyceal system. Two infective episodes at 20 and 27 weeks were associated with hyperemesis, metabolic acidosis and subsequent allograft dysfunction. She received intravenous hydrocortisone and sodium bicarbonate and azathioprine was temporarily reduced (50 mg once daily). During the latter episode haemoglobin fell to 7.8 g/dL and two units of packed red cells were transfused. Pancreatic function remained stable throughout pregnancy (HbA1C 4.5%).
Uterine artery Doppler waveform showed bilateral notching at 20 weeks and aspirin was recommenced; it had previously been stopped prior to pregnancy due to gastritis. At 29 weeks she developed proteinuria (1.5 g/24 hours) and hypertension and was started on methyl-dopa (250 mg twice daily) which was progressively increased (500 mg tds) and she was managed expectantly for preeclampsia. Serum Cr had risen from 160 to 180 µmol/L by 31 weeks, with a concurrent pseudomonas urinary tract infection; she was treated with oral ciprofloxacin. At 33 weeks her serum Cr increased further to 248 µmol/L and remained elevated.
At 33 + 6 weeks she had an induction of labour and a forceps delivery of a female infant (1790 g) (Apgar scores at 1 and 5 minutes: 6 and 9 and venous cord blood pH 7.17), who initially was transferred to neonatal intensive care. An evacuation of retained placenta was performed post delivery and she was noted to have a haemoglobin of 7.7 g/dL, which was managed conservatively. Day 8 postpartum dilation of the collecting system (1.4 cm pelvis) of the graft was still present on ultrasound imaging but her serum Cr had fallen to 153 µmol/L. Serum Cr remained elevated for 2 months post delivery, but then reduced back to prepregnancy values and is 102 µmol/L (eGFR 56 mL/minute/1.73 m2) at 41 months after the pregnancy.
DISCUSSION
The first pregnancy in a woman with a simultaneous pancreas–kidney (SPK) transplant was reported in 1986.
1
Increasing numbers of women of child-bearing age are receiving SPK worldwide with concurrent improvements in patient and graft survival (
Immunosuppression
Several studies have now confirmed that tacrolimus, 7 cyclosporine 8,9 and azathioprine 10–12 are non-teratogenic, although mean Cr levels tend to be higher in women with single kidney transplants receiving tacrolimus than those receiving cyclosporine throughout pregnancy and postpartum. 13 There is increasing evidence suggesting that MMF is associated with a syndrome including hypoplastic nails, shortened fifth fingers, microtia (ear deformity) and cleft palate. 14 The safety profile of sirolimus is unknown; no adverse events have been reported in 39 pregnancies, 14 but it is still not recommended in pregnancy by European Best Practice Guidelines. 15
Immunosuppression should be discussed prepregnancy and appropriate adjustments made in order to avoid teratogenicity. In the event of an unplanned pregnancy, medication should be adjusted on an individual basis depending on gestation and previous history of rejection. Drug levels should be closely monitored as pregnancy can be associated with an increase in calcineurin inhibitor requirements, 16 which occurred in two of the cases described. Compromised absorption may occur with hyperemesis and women should be encouraged to seek early medical help if they are unable to take their immunosuppression orally. Post delivery drug levels may increase dramatically and therefore continued monitoring is essential.
Graft loss
Pancreatic function was unaffected in all three women. The majority of women with SPK maintain normoglycaemia throughout pregnancy, although the development of gestational diabetes, requiring insulin and resolving after delivery, has also been described 4 and should be screened for in women taking tacrolimus and prednisolone. Single kidney long-term graft survival may be only minimally affected 17 or unaffected by pregnancy 16 ; however, deterioration in allograft function and allograft loss appears to be more common in women with SPK after pregnancy despite these organs usually being from younger donors. Out of 43 women with SPK, with pregnancies reported by NPTR, eight (19%) experienced graft losses within two years postpartum, three women lost renal allograft function, three lost pancreas allograft function; and two women lost both kidney and pancreas. After a mean follow-up period of 6.4 ± 3.8 years, 29 (67%) women reported good function of both grafts, three had died and 11 (26%) had varying degrees of graft dysfunction. 4
Women with SPK (6 recipients with 8 pregnancies) who experienced graft loss following pregnancy have also been found to have higher serum Cr and episodes of rejection during pregnancy or postpartum than women without graft loss (21 recipients with 28 pregnancies). Prepregnancy Cr does not predict graft loss; 18 therefore, close observation and prompt investigation of suspected rejection in pregnancy are imperative. Women with graft loss also tend to have smaller babies and more neonatal complications than those without graft loss. 18 Larger numbers are required for more accurate estimation of risk of graft loss, but women should be informed of possible effects of the pregnancy on graft function, and immunosuppression should be maintained at levels consistent with those prepregnancy.
Infection
Infection is the most common complication in SPK pregnancies, 4 frequently occurring in the urinary tract. Pregnant women with SPK have even higher rates of infections than pregnant women with diabetes and kidney transplants despite normoglycaemia. 5 Pancreatico-duodenocystomy may result in a chemical cystitis which can predispose to infection. Normal pregnancy is associated with renal tract dilation and a predisposition to bacteruria and pyelonephritis. Women with renal allografts have further risks due to pre-existing urological abnormalities, e.g. bladder problems, calculi, reflux to native or transplanted kidneys, ureteric re-implantation and immunosuppression. European Best Practice Guidelines for women with single renal transplant in pregnancy recommend monthly screening for bacteruria and additional sampling in the presence of symptoms and two weeks of antibiotic treatment for asymptomatic bacteruria and prophylactic antibiotics for the rest of the pregnancy 15 ; a temporary reduction in immunosuppression in severe cases should also be considered. Serial ultrasound imaging of the allograft is essential if there is any suspicion of obstruction because external drainage may be also necessary.
Obstruction
Two of the three cases developed renal impairment secondary to obstruction. In case 3 this occurred in the setting of pyelonephritis, which was managed conservatively; case 2 developed urinary retention following perineal damage with a subsequent rapid deterioration in renal function. Other authors have also reported renal impairment following renal outflow obstruction, 5,19 which may be related to the intraperitoneal position of the kidney allograft (see Figures 1 and 2). Prepregnancy ultrasound imaging of the transplanted kidney is informative as the presence of hydronephrosis is associated with increased infections and lithiasis. 20 Further dilation of the renal tract is expected in pregnancy but may exacerbate pre-existing hydronephrosis. Imaging must be performed after micturition as dilation may occur due to increased bladder pressure. Scanning of the allograft is important with any rise in serum Cr, although it must be remembered that obstruction can occur without pain in the denervated kidney and in the absence of pelvicalyceal dilation due to the restriction of expansion by surrounding fibrosis. Conservative management includes lying the patient on her side away from the renal allograft or reduction of amniotic fluid. If serum Cr continues to rise, a nephrostomy, antegrade pyelogram and subsequent J stent insertion may be required.

Kidney pancreas graft with duodeno-ileostomy
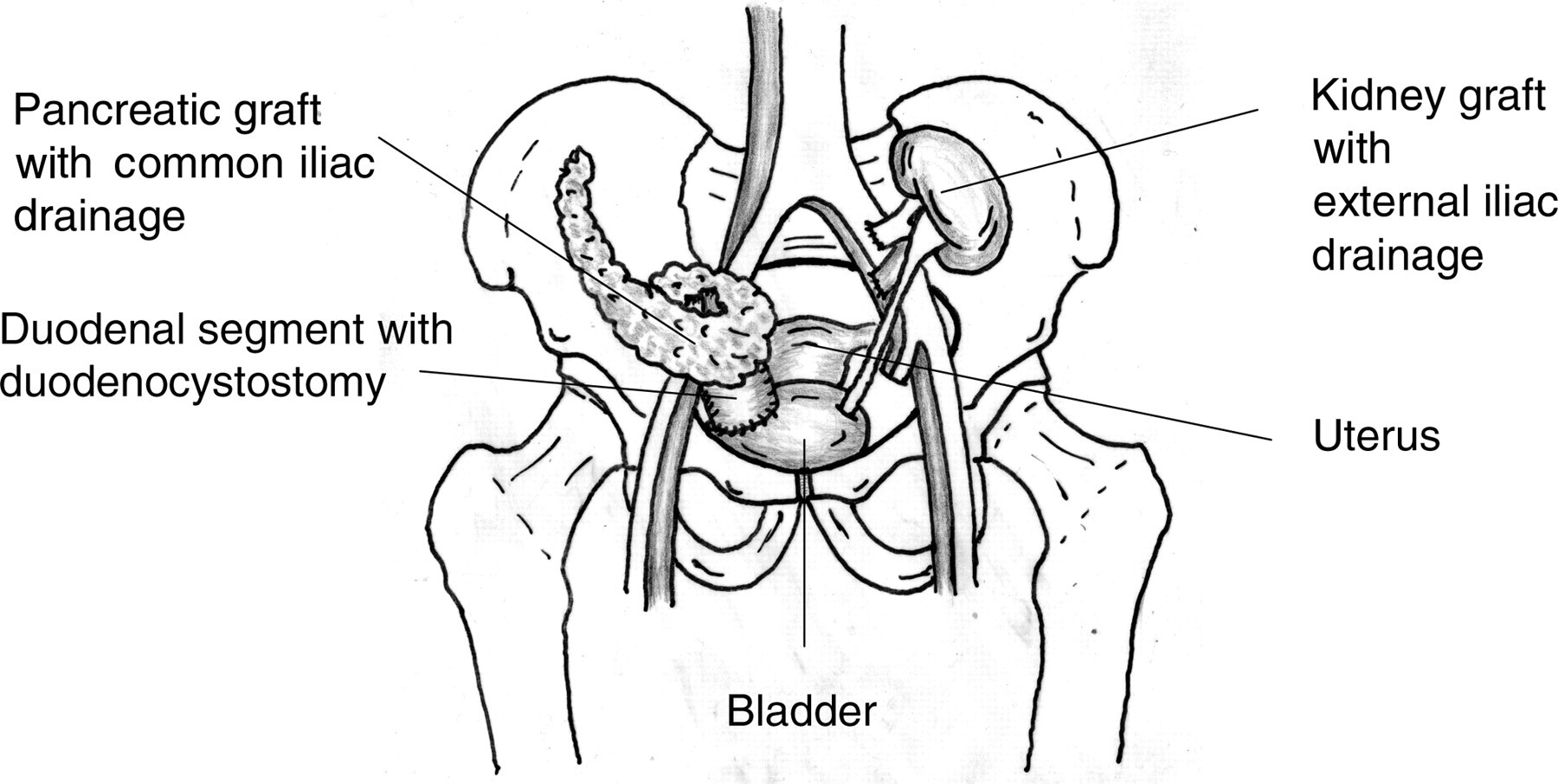
Kidney pancreas graft with duodenocystostomy
Acidosis
Women with pancreatico-duodenocystostomies require high doses of sodium bicarbonate to replace alkaline secretions from the exocrine pancreatic allograft lost in the urine. In the presence of sepsis, or the inability to take sodium bicarbonate supplementation (e.g. hyperemesis), women with SPK are at risk of developing metabolic acidosis. This should be treated with intravenous sodium bicarbonate until the woman is able to recommence sufficient oral replacement.
Preeclampsia
The rate of preeclampsia in women with SPK is reported to be 34%. Women with single kidney transplants have higher rates of preeclampsia than background and are at greater risk with higher serum Cr preconception and number of episodes of rejection. 21 The numbers of women with SPK are currently too small to identify clinical risk factors associated with preeclampsia, but the majority of these women are hypertensive, a condition that is independently associated with increased risk of preeclampsia. 22 Preeclampsia rates increase with the number of complications for women with type 1 diabetes. 23 Uterine artery Doppler findings may be difficult to interpret as the uterine artery may be sacrificed as part of transplant surgery. The influence of previous diabetes in normoglycaemic women with SPK on the development of preeclampsia is unknown, but postpartum urinary retention in Case 2 demonstrates that clinicians should remain aware of previous residual complications of diabetes for many reasons.
Case 3 highlights the difficulty in distinguishing between preeclampsia and progressive proteinuria, hypertension and renal impairment. A baseline PCR at booking is useful to allow monitoring of progression of proteinuria. Differentiation between the two conditions is often academic at later gestations because delivery is the appropriate treatment option for both. The risk of preeclampsia in a meta-analysis of high-risk pregnancies has been demonstrated to be reduced by the use of aspirin. 24 It is therefore advisable in all women with SPK and low-dose aspirin should be commenced or continued preconception or as soon as the pregnancy is confirmed. 20 Chronic or de novo hypertension above 140/90 should be treated. 25 Pre-existing proteinuria may increase, particularly in the third trimester, even in the absence of preeclampsia and it is advised that women with nephrotic range proteinuria should commence thromboprophylaxis due to their prothrombotic state. 25
Delivery
The majority of deliveries to SPK recipients are by caesarean section; 21 however, there is no anatomical reason why vaginal deliveries are less likely to succeed, nor will allografts be damaged by fetal descent or vaginal delivery. Therefore, a normal delivery should be the aim in women with SPK, in the absence of obstetric indication for a caesarean section. A transplant surgeon experienced with SPK should be available in the event of a planned or emergency caesarean section and the anatomy of the ureteric and pancreatic surgery reviewed with the surgeon prior to caesarean section. 26
For a more comprehensive guide to management, the reader is referred to the following excellent reviews. 26–29 Learning points are summarized in Table 1.
Learning points for management of pregnant women with simultaneous pancreas–kidney (SPK) transplants
MMF = mycophenolate mofetil
SUMMARY
Women with SPK have complicated pregnancies and are at risk of graft loss during pregnancy and postpartum. With increasing numbers of SPK recipients becoming pregnant, more data regarding prediction of risk of adverse outcome will become available, which will enable more accurate prepregnancy counselling.
Footnotes
ACKNOWLEDGEMENTS
We would like to thank Professor John Lumley for providing the figures.