
Abstract
In November 2009 the Royal College of Obstetricians and Gynaecologists published an updated guideline, ‘Reducing the risk of thrombosis and embolism during pregnancy and the puerperium’. This includes a clear and simple score-based risk assessment tool, designed for antenatal and postnatal patients. Thresholds are given at which thromboprophylaxis should be offered. However the proportion of patients who reach the threshold is not estimated in the guideline, and we are not aware of any published data regarding this. In this cross-sectional study, we studied the case-notes of all 109 deliveries conducted over a one-week period, including elective caesarean sections. Of those, 7% met the threshold for antenatal thromboprophylaxis and 41% met the threshold for postnatal thromboprophylaxis.
INTRODUCTION
Despite an increase in use of thromboprophylaxis in pregnancy and the puerperium, pulmonary embolism remains the leading direct cause of maternal death in the UK (1.56/100,000 maternities), with 79% having identifiable risk factors. 1 Advancing maternal age and increasing maternal BMI (body mass index) are significant risk factors which are becoming more prevalent in society. 2
In November 2009 the Royal College of Obstetricians and Gynaecologists (RCOG) published an updated Green-top Guideline, 3 entitled ‘Reducing the risk of thrombosis and embolism during pregnancy and the puerperium’. The updated guideline recommends formal documented risk assessment for all women before or in early pregnancy, and again if admitted to hospital or if intercurrent problems develop. The guideline includes a clear and simple score-based risk assessment, designed for antenatal and postnatal patients. Thresholds are given at which thromboprophylaxis should be offered. The authors acknowledge that the evidence is low grade (due to a paucity of high-quality trials) and that alternative approaches may be reasonable. Extrapolating from studies on medical and surgical patients, they suggest that the risk of venous thromboembolism (VTE) in obstetric patients may be reduced by up to two-thirds.
The proportion of patients who reach the threshold for thromboprophylaxis, and therefore potential cost to units, is not estimated in the guideline. The National Institute for Health and Clinical Excellence (NICE) guideline published last year 4 acknowledges that there is no cost-effectiveness evidence for antenatal patients admitted to hospital. Before introducing the RCOG risk assessment tool in our unit, we wished to establish what proportion of patients would reach the threshold. This would allow us to estimate the implications and cost of introducing the tool, and plan appropriately. The cost of the drug is small, but there are other potential costs which are not immediately apparent (Table 1). In addition to this, patients receiving antenatal thromboprophylaxis may be denied regional analgesia or anaesthesia if this is required within 12 hours of their most recent dose. We wished to have further information on the number of patients this may affect to facilitate liason with the anaesthetic department before introduction of the tool.
Potential costs of thromboprophylaxis (in addition to drug costs)
METHODS
We performed a cross-sectional study using a retrospective case-note review of all deliveries over a one-week period. Our unit is a university teaching hospital with approximately 6000 births per annum. At the time of the study, a formal documentation of risk factors using a scoring tool was not being undertaken.
The antenatal hand-held notes, delivery record and postnatal notes were reviewed to identify any of the risk factors listed in the tool and data entered by hand on an anonymized data collection sheet. These results were collated using an Excel spreadsheet and a risk assessment score was generated.
RESULTS
Data from 104 patients have previously been published in abstract form. 5
A list of deliveries was gained daily from the birth register on the delivery suite, which includes all deliveries including home births. There were 113 deliveries between 08:30 on 4 December 2009 and 08:30 on 11 December 2009 at the Norfolk and Norwich University Hospital. There were no home births. Case-notes for all 113 deliveries were available.
Of those, 32 deliveries were via caesarean section (16 elective, 16 emergencies) leaving 81 vaginal deliveries.
Eight patients (7%) met the criteria for being offered antenatal thromboprophylaxis by scoring three or greater using pre-existing risk factors. Of these, only two met the criteria due to a personal or family history of thrombosis (one of each: the patient with family history also having a BMI > 30). The remaining six of those eight were due to a combination of high BMI (n = 5), smoking (n = 5) or age (n = 2).
If they had been admitted to hospital, a further 18 patients (17%) would have met the criteria for antenatal prophylaxis by scoring two or greater on pre-existing and transient risk factors.
Forty-six patients (41%) met the criteria for postnatal thromboprophylaxis for at least seven days. The number of patients with each risk factor is shown in Figure 1.
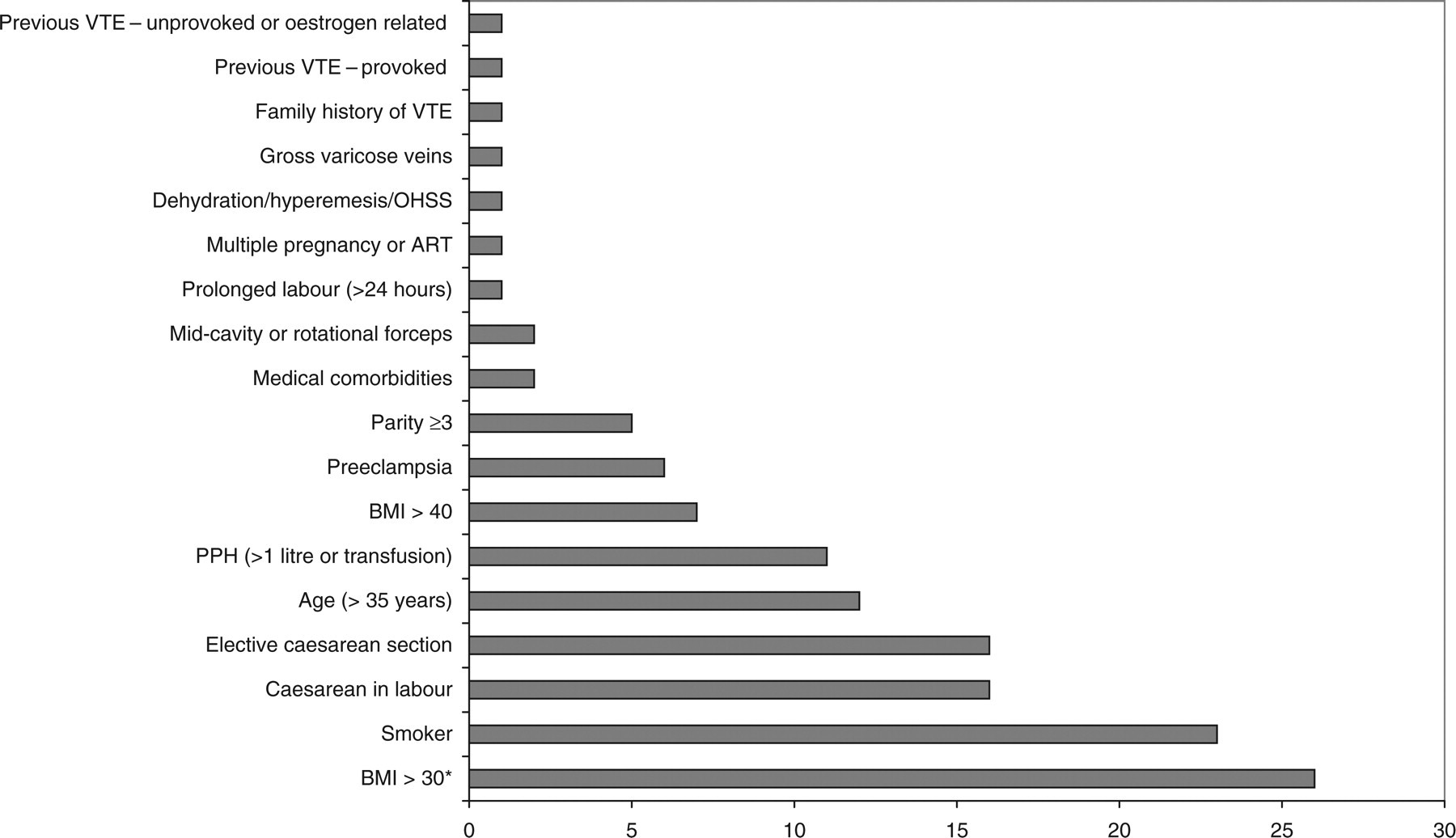
Number of patients with risk factors for venous thromboembolism. *Includes those with BMI > 40. BMI = body mass index; VTE = venous thromboembolism; OHSS = ovarian hyperstimulation syndrome; ART = assisted reproductive therapy; PPH = postpartum haemorrhage
DISCUSSION
In our study population, 7% and 41% would qualify for antenatal and postnatal thromboprophylaxis, respectively. The commonest risk factor identified was obesity, with 26 patients (23%) having a BMI > 30 (Figure 1, BMI > 30 and > 40 shown separately). Maternal obesity varies in different populations, being more common in deprived populations. A study of English maternity units showed that only 20% of those mothers resident in the least deprived areas had a BMI > 30 compared with 33% of those resident in the most deprived areas. 2 The same study showed different obesity rates in ethnic groups, the proportion of women classified as obese doubled between 1989 and 2007, and that this increase was accelerating, rather than increasing in a linear manner. The second commonest single risk factor identified was smoking, with 23 patients (20%) being recorded as smokers. A recent Scottish study showed that the percentage of pregnant women who smoked varied from 14% in the least deprived areas to 39% in those areas most deprived. 6 The same study showed that those in most deprived areas are more likely to under-report their smoking habits.
Units located in more deprived areas may therefore anticipate that more patients reach the threshold for thromboprophylaxis, and that these numbers will continue to increase as obesity rates rise.
At the time of our study, a formal documentation of risk factors using a scoring tool was not being undertaken. Our hand-held notes contain space for medical history, family history, smoking status and BMI. However there is no specific space for personal or family history of VTE, history of thrombophilia or gross varicose veins. Therefore, it is probable that risk factors were under-recorded and that if a formal risk scoring tool was used, the proportion of patients reaching the threshold would be higher than in our study.
The RCOG guideline 3 recommends that patients be offered thromboprophylaxis. The proportion of patients who accept this offer will vary depending on the counselling they receive, and they are likely to be influenced by the health professional delivering the counselling. Our unit is preparing written information to aid counselling, and to introduce a degree of standardization.
We did not study the health or economic benefits of thromboprophylaxis. It may be that the benefits of thromboprophylaxis more than outweigh the costs. A Swedish study using a different risk-scoring system modelled that the cost of prevention was less than the cost of treating the VTEs which may be prevented. 7 However their model did not include costs for those factors listed in Table 1.
It is clear that using the formal risk scoring tool will increase the number of patients offered thromboprophylaxis, and this will have additional costs to units as they implement it. In performing this study, we were not looking for reasons against implementing the RCOG tool, but wished to have the necessary financial and staffing systems in place prior to implementation. This will involve not only obstetricians and hospital midwives but also community midwives and general practitioners.