
Abstract
Background:
Hypertensive crisis is an important cause of maternal and perinatal morbidity and mortality.
Aim:
To compare the efficacy of oral nifedipine and intravenous labetalol.
Materials and methods:
One hundred women with hypertensive crisis were randomized to receive either oral nifedipine 10 mg or intravenous labetalol 20 mg. Oral nifedipine was given 10 mg stat followed by 10 mg every 30 minutes up to a maximum of 50 mg. Intravenous labetalol was given 20 mg stat followed by 40 mg 30 minutes later then two more doses of 80 mg every 30 minutes up to a maximum of 220 mg. The primary outcome was the number of doses required to achieve target blood pressure (BP) and time required to reduce the mean arterial pressure by 25%. Secondary outcomes analysed included additional drugs required, resurgence of hypertensive crisis. Data were analysed using repeated measures analysis of variance (ANOVA), mixed ANOVA, unpaired t-test and chi square test and P value ≤0.05 was considered significant.
Results:
Systolic (SBP), diastolic (DBP) and mean arterial blood pressure (MAP) were lower than baseline at all time points of follow-up in both nifedipine and labetalol groups (P < 0.01). P < 0.05 by repeated measures ANOVA for overall trend of changes in SBP, DBP and MAP for within-group effects in both nifedipine and labetalol groups and P < 0.05 by mixed ANOVA for between-group effects during entire observation period. The magnitude of fall in SBP, DBP and MAP was greater in the labetalol group compared with the nifedipine group (P < 0.05). Target BP was achieved in 90% in the nifedipine group and 92% in the labetalol group. Maternal and fetal adverse effects were infrequent.
Conclusion:
Both oral nifedipine and intravenous labetalol are effective in the treatment of hypertensive crisis. Intravenous labetalol may have benefits because it is more effective in reducing the SBP, DBP and MAP to target levels with a lower number of doses.
Keywords
Introduction
Hypertensive disorders are the most common medical disorders encountered during pregnancy and are responsible for 31% of the maternal deaths in India. 1 The main causes of mortality are severe pre-eclampsia, hypertensive crisis, cerebrovascular accidents and HELLP (Haemolysis, Elevated Liver enzymes, Low Platelet count) syndrome. A retrospective analysis of maternal deaths due to hypertensive disorders at our own institute revealed hypertensive crisis as the main cause of mortality. 2 There is still controversy regarding the initiation of antihypertensive therapy in mild and moderate hypertension as well as about the choice of antihypertensive therapy in hypertensive emergencies and urgencies. According to the American College of Obstetricians and Gynecologists (ACOG) committee opinion (2011), acute onset, severe systolic (≥160 mmHg) or diastolic hypertension (≥110 mmHg) or both in pregnant or postpartum patients constitutes hypertensive emergency. 3 National Institute for Health and Clinical Excellence guidelines from 2010 recommend the use of intravenous hydralazine, oral nifedipine and intravenous labetalol for the treatment of severe hypertension in pregnancy which is defined as a systolic blood pressure (SBP) ≥160 mmHg and/or a diastolic blood pressure (DBP) ≥110 mmHg. 4
Intravenous hydralazine has been the drug of choice since the 1970s but a recent meta-analysis cautions against its use as the drug of first choice due to severe hypotension and other maternal and fetal complications. 5 Similarly, the use of sublingual nifedipine and oral nifedipine has been criticized because of an unpredictable decrease in blood pressure (BP) and major cardiac events leading to maternal death and fetal distress. A recent review advised against their use for hypertensive crisis, although a randomized double blind trial of oral nifedipine and intravenous labetalol did not report any adverse outcome with oral nifedipine. 6 In this context more randomized trials are required.
This study was undertaken to compare oral nifedipine with intravenous labetalol in hypertensive emergencies and urgencies of pregnancy.
Materials and methodS
This randomized trial was undertaken in the Department of Obstetrics, JIPMER, a tertiary care hospital in South India, between September 2008 and April 2010. The study was approved by Institute ethics committee (SEC/40/2008) and informed consent was obtained from the patients or their relatives in unconscious patients. Pregnant women of more than 28 weeks gestation or less than 48 hours postpartum with BP of 160/110 mmHg or SBP ≥160 mmHg irrespective of DBP or DBP ≥110 mmHg irrespective of SBP were included in the study. Patients without end organ damage were categorized as hypertensive urgency and those with end organ damage like eclampsia, HELLP syndrome, hypertensive encephalopathy, retinopathy and disseminated intravascular coagulation were labelled as hypertensive emergency. Patients with bronchial asthma, congestive heart failure and known atrioventricular block were excluded.
The sample size was calculated using OpenEpi, version 2.3.1 software based on a similar study by Vermillion et al. 6 With the aim of detecting 20% difference in the time interval required to reach the target blood pressure, and with 95% confidence interval and power as 95%, it was calculated that 32 patients would be required in each group. Patients fulfilling the selection criteria were examined by one of the authors and a detailed history regarding antenatal care, past medical, surgical, family and obstetric history was taken. A general, physical and systemic examination was done. BP was re-checked after one hour of admission and a diagnosis of hypertensive urgency or emergency was made. The participants were then randomized by a computer-generated random number table into two groups. The study was not masked. Group A patients received tablet oral nifedipine 10 mg stat followed by 10 mg every 30 minutes till the target BP was achieved and or up to a maximum of 50 mg. It is recommended that while administering antihypertensive therapy, the mean arterial pressure should not be reduced beyond 25% and therefore the target BP to be achieved was calculated as a 25% reduction of mean arterial BP compared with the admission BP.7,8 Once the target BP was achieved, patients received a maintenance dose of nifedipine 10 mg eight hourly. Group B patients received intravenous labetalol 20 mg stat followed by 40 mg 30 minutes later and two more doses of 80 mg every 30 minutes until the target BP was achieved and/or up to a maximum of 220 mg. The dosing regimens were in accordance with those of ACOG recommendations 9 except that labetalol was given every 30 minutes in order to compare the time taken to achieve the target BP with that of nifedipine. Once the BP was controlled, patients received a maintenance dose of oral labetalol 100 mg twelve hourly. 8 BP was measured with non-invasive BP cuff and all patients were on continuous monitoring. If the target BP was not achieved with the maximum dose of antihypertensive, nitroglycerin patch was applied. Resurgence of hypertensive crisis was noted and treated with the same drug. All patients with imminent eclampsia (symptoms of headache, vomiting, epigastric pain and hyper-reflexia) received a prophylactic dose of magnesium sulphate and those with eclampsia received therapeutic doses of magnesium sulphate. Investigations included urine protein, complete haemogram, renal and liver function tests, ultrasonogram for fetal growth and liquor and fundoscopy. Cerebral computed tomography/magnetic resonance imaging was done if the patients were comatose or having recurrent convulsions.
Maternal monitoring included a record of pulse rate, respiratory rate, BP and urine output every 30 minutes until the target BP was reached and thereafter for 24 hours. Success was defined as a decrease in MAP by 25%. Uncontrolled hypertension was defined as failure to achieve target BP after the maximum dose. If there was no resurgence, BP was recorded every eight hours until discharge. Patients were followed up for 48 hours postpartum or until discharge. Fetal monitoring was done by intermittent auscultation every 30 minutes in the first stage of labour and every 5-10 minutes during the second stage of labour. Cardiotocography was used once fetal distress was suspected by intermittent auscultation.
The primary outcome was the number of doses required to achieve target BP and the time required to reduce the MAP by 25%. Secondary outcomes analysed included additional drugs required, resurgence of hypertensive crisis, maternal and fetal side-effects such as hypotension, maternal tachycardia, headache, flushing, nausea and vomiting, dizziness, fetal bradycardia abruption or cardiovascular accidents after starting the antihypertensive medication. The overall trend of differences in systolic, diastolic and mean arterial blood pressures across the entire follow-up period were analysed using a general linear model for within-group effects with repeated-measures analysis of variance (ANOVA), and for between-group effects with a mixed ANOVA. Significant differences were further evaluated with Bonferroni post hoc analyses. A two-tailed P value <0.05 was considered statistically significant. The other data were analysed using unpaired t-test, Fischer's exact test and chi square test and P value ≤0.05 was considered significant.
Results
Clinical profile of patients in nifedipine and labetalol group
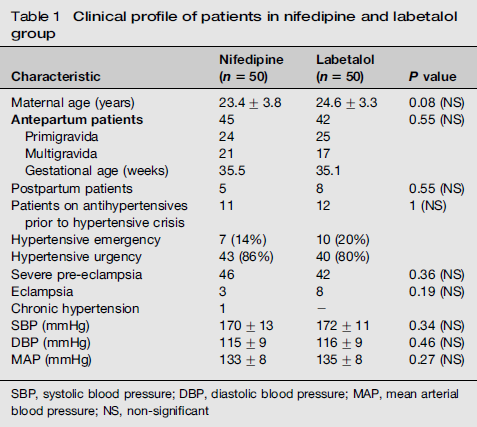
In Group A (nifedipne) seven patients presented with hypertensive emergency. Three had HELLP syndrome, one was oliguric, two had antepartum eclampsia and one had postpartum eclampsia. In Group B (labetalol), 10 patients presented with hypertensive emergency of which two had HELLP syndrome, seven had antepartum eclampsia and one had postpartum eclampsia. No other significant complications were observed in patients with hypertensive emergency. Twenty-five patients in the nifedipine group and 32 patients in the labetalol group received magnesium sulphate (P value 0.22).
The administration of both nifedipine and labetalol led to a significant decrease in SBP, DBP and MAP (P < 0.05 within-group effect; Figure 1). Systolic BP, DBP and MAP were lower than baseline at all time points of follow-up in both nifedipine and labetalol groups (P < 0.01; Figure 1). Thirty minutes following initiation of therapy with either drug, there was significant fall in BP in both the groups indicating that both the drugs are efficacious in lowering BP. The magnitude of fall in SBP, DBP and MAP was greater in the labetalol group compared with the nifedipine group (P > 0.05).
Comparison of blood pressure at half hourly intervals in nifedipine and labetalol groups. *SBP, DBP and MAP were lower than baseline at all time points of follow-up in both nifedipine and labetalol groups (P < 0.01). P < 0.05 by repeated measures ANOVA for overall trend of changes in SBP, DBP and MAP for within-group effects in both nifedipine and labetalol groups. P < 0.05 by mixed ANOVA for between-group effects during entire observation period. SBP (F = 5.479, df 4.6; P = 0.000), DBP (F = 4.843, df 5.1; P = 0.000), MAP (F = 6.202, df 4.9; P = 0.000). SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial blood pressure; ANOVA, analysis of variance; df, degrees of freedom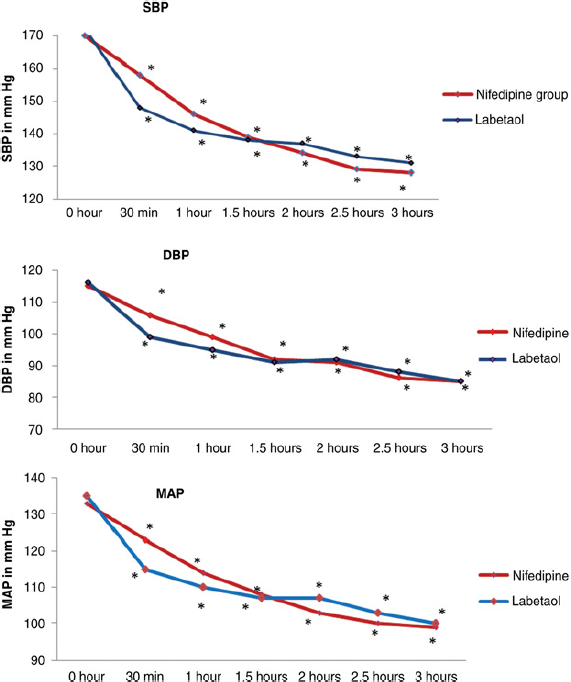
Number of doses required to achieve target blood pressure

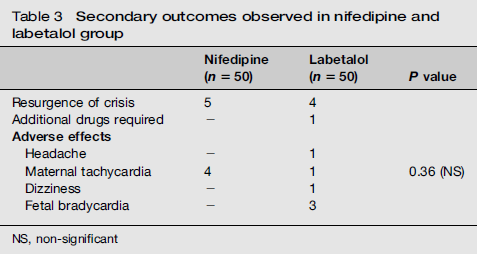
Secondary outcomes observed in nifedipine and labetalol group
Pregnancy and fetal outcome in nifedipine and labetalol group

Discussion
Reduction of BP is an important strategy in the management of severe pre-eclampsia for the prevention of both maternal and fetal adverse events. Recommended drugs for treatment of hypertensive crisis are oral nifedipine, intravenous labetalol and hydralazine. 10 The use of these drugs has been studied in a number of randomized control trials. Nifedipine has been found to have a rapid onset, longer duration of action and the advantage of oral administration.6,11-13 It selectively increases renal perfusion and thereby has a diuretic effect. 14 Intravenous labetalol is a fast-acting antihypertensive with few adverse effects on mother and fetus.6,15-17 It also potentially decreases cerebral perfusion pressure thereby decreasing the incidence of eclampsia. 18
This is the second randomized trial comparing oral nifedipine and intravenous labetalol for management of severe hypertension in pregnancy. In the present study both drugs were found to be effective antihypertensives in the treatment of hypertensive crisis and this is consistent with the reports of the previous studies.6,11,15,16 However, there was significantly greater decrease in the systolic, diastolic and MAP at the end of 30 minutes and one hour in the labetalol group compared with the nifedipine group. The reduction of MAP achieved within 30 minutes with labetalol was double that of nifedipine (labetalol 135-115 mmHg, a reduction of 20 mmHg of MAP; nifedipine 133-123 mmHg, a reduction of 10 mmHg of MAP; P value 0.002) indicating the rapid onset of action of labetalol (Figure 1). A similar trial by Vermillion et al. 6 conducted in 50 peripartum patients with severe pre-eclampsia demonstrated that nifedipine lowered BP more rapidly with fewer doses than intravenous labetalol. This discrepancy is probably because of the higher dose of nifedipine (20 mg) used in their study. The dose regimens of the present study are in accordance with the recommendations of ACOG 2002a with the only variation being a time interval of 30 minutes for the subsequent doses in the labetalol group although the recommended interval was 10 minutes. 9 The time interval was altered so as to compare the fall in BP every 30 minutes between the two groups.
The number of doses required to control the BP indirectly reflects the time required to reach the desired BP, the probability of persistent severe hypertension and the side-effects, all increasing with increasing dose requirements. As 44% of patients in the labetalol group required a single dose compared with 14% in the nifedipine group to reach the target BP, it is evident that intravenous labetalol is more effective than oral nifedipine in reducing the BP to target levels. Seventy percent of patients required only 1-2 doses of labetalol to reach target MAP similar to the success rate obtained in the study by Vigil-de Gracia et al. 15 The average number of doses required in the nifedipine group were three compared with two in the labetalol group. However, nifedipine with longer duration of action reduces the BP in a gradual manner while labetalol reduces BP with rapid onset but further reduction being gradual and reaching a plateau with time (Figure 1). This is reflected in the pattern of resurgence of hypertensive crisis with only one patient in the nifedipine group having resurgence within 24 hours whereas all the four patients in the labetalol group had resurgence within 24 hours.
All the patients responded to antihypertensive agents except for a single patient who did not respond to the maximum dose in the labetalol group. The failure rate with labetalol is similar to that in other studies.15,16 Further, there were no cases of overshoot hypotension, cerebrovascular accidents, eclampsia or abruption after initiation of antihypertensive treatment. There were no cases of maternal mortality. Though efficacy has been demonstrated with sublingual administration of nifedipine, it is not recommended due to the risk of sudden hypotension. 10
Maternal side-effects such as tachycardia, headache and dizziness were insignificant indicating that both the drugs can be used safely. Another concern with labetalol is adrenergic blockade that can cause fetal bradycardia but it has been found that labetalol does not affect umbilical artery waveforms and does not have any adverse effect on neonatal outcome. 19 In a systematic review of 26 studies, it was concluded that commonly-used antihypertensives do not adversely affect fetal heart rate. 20 One patient in the present study had fetal bradycardia which cannot be reliably attributed to the drug but may be due to the underlying placental disease process itself.
From the conclusions of the present study, it can be stated that though both oral nifedipine and intravenous labetalol are effective in the treatment of hypertensive crisis during pregnancy, intravenous labetalol may have benefits because it is more effective in reducing the SBP, DBP and MAP to target levels with a lower number of doses.