
Abstract
Peri-partum Cardiomyopathy (PPCM) is a rare and life threatening complication of pregnancy. There are only two cases registered with the World Health Organization of cases of cardiomyopathy in patients taking Quetiapine. Here we discuss an interesting case of potential Quetiapine induced cardiomyopathy.
Introduction
Peripartum cardiomyopathy (PPCM) is defined as new onset of left ventricular systolic dysfunction secondary to vascular changes during pregnancy. 1 It is a rare and life-threatening complication of pregnancy with an incidence of approximately one in 3000 to one in 4000 live births. Information on the risk of PPCM and outcomes in future pregnancies is limited and their remains to be a consensus on the management of such women and their future pregnancies.1,2
We present an unusual case of PPCM presenting as abdominal pain in a patient on long-term antipsychotics.
CASE REPORT
A 43-year-old Bangladeshi para 8 (all normal vaginal deliveries) presented to the labour ward triage at 24+6 week's gestation complaining of right-sided abdominal pain and vomiting. She originally booked at 10 weeks gestation, with a body mass index of 39. She had a past medical history of long-term schizo-affective disorder and had been doing well on treatment with quetiapine after failure of other psychotropic medication. On admission the patient was initially treated with analgesia, antiemetics and intravenous fluids. She was apyrexial, blood pressure (BP) 128/88 and heart rate (HR) 110 sinus rhythm on an electrocardiogram (ECG). On examination the patient was noted to have an ejection systolic cardiac murmur, mild bi-basal crepitations and a soft abdomen with tenderness in the right upper quadrant. The fetal HR was 140-145 beats per minute (bpm).
Investigations revealed a normal full blood count, renal function, liver function and clotting profile. Her urine dipstick was normal. A chest radiograph revealed cardiomegaly, moderate bilateral pleural effusions and signs of heart failure. The patient was commenced on frusemide and was reviewed by the cardiology team. An urgent echocardiogram was performed showing a dilated left ventricle with an ejection fraction of 15-20%. Functional mitral regurgitation and moderate tricuspid regurgitation were reported.
Frusemide was continued and beta-blocker (metoprolol) and hydralazine were added. Given the complexity of her diagnosis and mental health issues the patient was reviewed at a tertiary centre, who advised for the patient to be admitted to the coronary care unit (CCU) for close monitoring under joint care with the cardiologists and obstetricians. She would be transferred back to the tertiary centre at 34 weeks gestation.
The patient remained stable on CCU and at 28 weeks gestation episodes of non-sustained ventricular tachycardia were documented on telemetry. This was managed by titrating the dose of beta-blockers (Figure 1).
Non-sustained ventricular tachycardia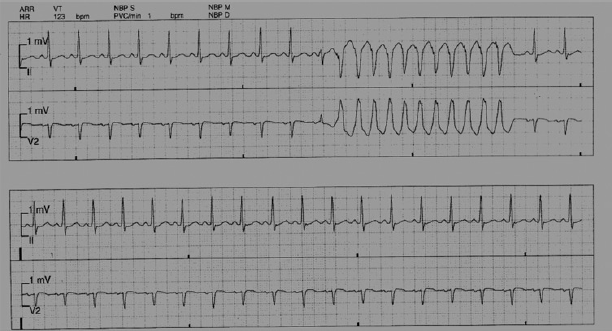
At 32 weeks gestation the patient unexpectedly had a pulse less electrical activity cardiac arrest on CCU. Cardiopulmonary resuscitation (CPR) was commenced and after four minutes an emergency caesarean section was performed. CPR was successful and the patient was transferred to the intensive care unit (ITU) in sinus rhythm. She was intubated and required ionotropic support for 24 hours. She remained on ITU for five days where she was treated for sepsis secondary to a pelvic collection and her cardiac medication was optimized. She was transferred to CCU five days postpartum. Neonatal resuscitation was required and the baby was intubated and transferred to the Neonatal Intensive Care Unit. The baby was diagnosed with tetralogy of fallot and was doing well on medical treatment.
Her cardiac function in the postpartum period remained unchanged. A repeat echocardiogram showed severe mitral regurgitation with no other changes. A cardiac magnetic resonance imaging (MRI) with gadolinium was performed which showed dilated left atrium and right atrium, with moderate mitral regurgitation. The left ventricle was dilated with severely impaired systolic function (Figure 2). The scan was compatible with a diagnosis of dilated cardiomyopathy. The patient continued to have episodes of non-sustained ventricular tachycardia for which an implantable cardioverter defibrillator device was inserted. This was successful and prevented any further arrhythmias. Unfortunately the patient had a relapse of her schizo-affective illness and was transferred to the local mental health unit. She will be followed up in the cardiology outpatient clinic.
Cardiac magnetic resonance imaging: dilated cardiomyopathy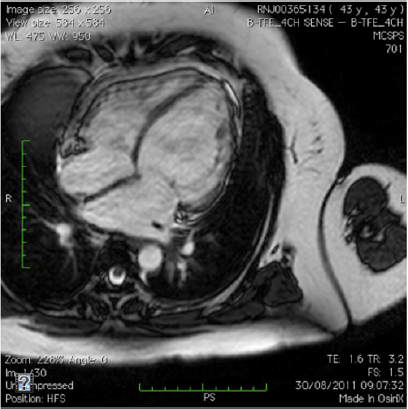
A long discussion was carried out with the patient and partner strongly advising against any future pregnancies, and as a result the patient has had a Mirena Intrauterine Device inserted as a form of contraception.
Discussion
Peripartum cardiomyopathy is a rare and life-threatening complication of pregnancy associated with maternal morbidity and mortality. Demakis et al. 3 and Lampert and Lang 4 have described four criteria for the diagnosis of PPCM 5
Development of cardiac failure in the last month of pregnancy or within five months of delivery;
Absence of other causes of heart failure;
Absence of pre-existing cardiac dysfunction;
Left ventricular systolic dysfunction confirmed by echocardiogram.
Our patient did not have any history of pre-existing heart failure or heart disease and although her diagnosis of PPCM was made in the second trimester, there have been other cases of PPCM diagnosed early in pregnancy. Recently, Elkayam et al. 5 provided evidence through a large observational study that patients presenting earlier than the last trimester with cardiomyopathy had similar clinical presentations and outcomes as those diagnosed in the last month of pregnancy, therefore suggesting the same diagnosis of PPCM throughout pregnancy. In all of our patients’ eight previous deliveries there was no evidence of cardiac dysfunction. Her last delivery one year ago was uncomplicated and the patient was asymptomatic throughout the pregnancy. She did have other risk factors including, increased maternal age, multi-parity and obesity.
There is a clear acceptance of the unknown aetiology of this complication of pregnancy. During pregnancy cardiovascular changes such as increase in blood volume and stroke volume can contribute to heart failure.1, 6 This patient may have had pre-existing heart failure, which was exacerbated by the haemodynamic stress of pregnancy. However, there was no evidence to confirm this theory. A number of other potential mechanisms for her heart failure were considered including myocarditis, abnormal response to haemodynamic stresses of pregnancy, stress-activated cytokines, cardio-tropic viral infections, raised serum markers of inflammation leading to cardiac cell death and an abnormal maternal immune response to pregnancy.1,2,7
The patient had an echocardiogram, which confirmed a dilated cardiomyopathy, and postpartum she was investigated with a cardiac MRI. Prior to delivery the echocardiogram showed trivial functional mitral regurgitation and moderate tricuspid regurgitation. It is well known that regurgitant valve diseases are well tolerated in pregnancy. It was only in the postpartum period that worsening mitral regurgitation was noted. This was most likely secondary to her left ventricular dysfunction and global dilated cardiomyopathy. The role of cardiac MRI in the diagnosis of PPCM has been recently better described. Cardiac MRI is the gold standard for diagnosing left ventricular dysfunction and is a non-invasive means of establishing ischaemic heart disease through cardiac gadolinium uptake. It is also useful in determining prognosis. 7 Our patient underwent a cardiac MRI, which showed a dilated cardiomyopathy with no other cardiac abnormalities.
This patient had been taking quetiapine for one year for schizo-affective illness. It is widely accepted that such antipsychotics have many side-effects including diabetes mellitus, hyperlipidaemia, cardiac dysfunction and arrhythmias, extrapyramidal symptoms and weight gain.8, 9 Quetiapine has been associated with myocarditis, which is a well-known cause of dilated cardiomyopathy. However, postpartum investigations excluded myocarditis as the cause. Quetiapine induced cardiomyopathy is extremely rare. There are only two cases registered with the World Health Organization of cases of cardiomyopathy in patients taking quetiapine. 10 Our patient continued quetiapine as it was thought the risk of relapse would be more detrimental to the patient.
PPCM is treated symptomatically. Due to restrictions of many drugs in pregnancy, the mainstay of treatment includes diuretics, vasodilators and ionotrophic support if needed. Beta-blockers are used cautiously in generic left ventricular dysfunction, however their use has not been tested in PPCM. Anticoagulation should also be considered due to the risk of thromboembolism. Following delivery treatment is converted to the standard treatment for left ventricular dysfunction, which includes angiotension converting enzyme inhibitors.2,3,7 Newer treatments such as immunoglobulins, immunosuppressive therapy and bromocriptine have shown early promising results; however, much more evidence is required to include these treatments in standard practice. 11
Patients should also be counselled regarding defibrillator devices. This is not a routine consideration in the treatment of PPCM; however, the multicentre autonomic defibrillator implantation trial II (MADIT II) confirmed survival benefit with an ICD in patients with arrhythmias. Our patient was referred for inpatient ICD insertion as she met the criteria for secondary prevention of sudden cardiac death. 12 Aggressive treatment such as intraaortic balloon counter pulsation can be used acutely or cardiac transplantation or more often a left ventricular assisted device, remain options for those patients on maximal therapies for severe heart failure.2,7
Mortality rates of 20-50% are well documented as a result of ventricular arrhythmias, thromboembolism and progressive heart failure. 13 Our patient experienced non-sustained ventricular arrhythmias while on CCU, all of which were medically managed.13, 14 Approximately 50% of patients will not see recovery of their left ventricular function and half of all deaths will occur within three months postpartum, as a result of worsening left ventricular function.5,15
Information on the prognosis of future pregnancies remains uncertain. There have been recommendations stating if ventricular function has fully recovered subsequent pregnancy is not contraindicated. If left ventricular function has not recovered the risk of recurrence is high and therefore another pregnancy is not recommended. Despite the limited data there is evidence to show a significant risk of recurrence in future pregnancies.2,4
In conclusion, peripartum cardiomyopathy is a rare complication of pregnancy. Although the aetiology is unknown many theories exist. Most patients once diagnosed are treated with the standard treatment for left ventricular dysfunction. There is insufficient evidence to diagnose quetiapine-induced cardiomyopathy, despite known adverse cardiac affects with antipsychotic drugs such as quetiapine. At present there is no exact evidence on the risk of PPCM on future pregnancies. As a result patients need to be carefully counselled when considering another pregnancy. This multidisciplinary approach should involve obstetricians, anaesthetists, cardiologists and the mental health team.