
Abstract
Objectives
The variable anatomy of the short saphenous vein (SSV) and the potential failure to identify the saphenopopliteal junction (SPJ) contribute to an increased risk of damage to the common peroneal nerve (CPN) during surgical exploration. The aim of the present study was to determine the variation of the SPJ, its relationship to the CPN, and the relationship of both SPJ and CPN to defined anatomical landmarks.
Methods
Measurements of the distance between the SPJ and CPN, and the defined anatomical landmarks (fibula head, lateral joint space, lateral femoral epicondyle), were undertaken on 30 cadaveric limbs following careful dissection of the popliteal fossa.
Results
The level of SPJ termination was classified as low (below), normal (within 100 mm above) and high (more than 100 mm above), the lateral femoral epicondyle. Of the 30 limbs dissected, 70% of SPJs were normal, 23% low and 7% high. Direct measurement from the SPJ to anatomical landmarks showed a higher interquartile range (IQR) in low compared with normal terminations; however, the vertical distance from the SPJ to the fibula head showed an increase in IQR from low to normal terminations (7.1–14.2). The mean distances between the SPJ and CPN in low and normal terminations were 23.3 and 16.7 mm, respectively. Comparison of the IQR showed values very similar to low terminations having a slightly higher IQR compared with normal terminations (7.15–6.0).
Conclusion
Significant anatomic variation was observed in the termination of the SSV, with 67% located within 66 mm above the lateral femoral epicondyle. The risk of damaging the CPN during saphenopopliteal ligation may be higher for SPJs located above the lateral femoral epicondyle because of the proximity of the two structures and variability of SPJ.
Introduction
The incidence of varicose veins in the western world is relatively high, with 20% of women and 7% of men over the age of 40 years being affected. 1,2 In the UK, this equates to an estimated 75,000 operations for varicose veins each year. 3
Saphenopopliteal surgery entails a transverse incision usually placed at or 1 cm below a preoperative duplex mark. The fascia is divided and the short saphenous vein (SSV) traced down to the saphenopopliteal junction (SPJ) and ligated. A section of the SSV is then excised or removed with a pin stripper. The success of superficial venous surgery within the popliteal fossa can be complicated by anatomical variations in the course and termination of the SSV. 4,5 Poor localization and variable siting of the SPJ are contributory factors associated with SSV reflux, as seen in the high rate of recurrent saphenopopliteal (30%) compared with saphenofemoral (7%) incompetence. 6 Failure to correctly identify the SPJ during surgery results in recurrent varicose veins and associated symptoms. 7–10
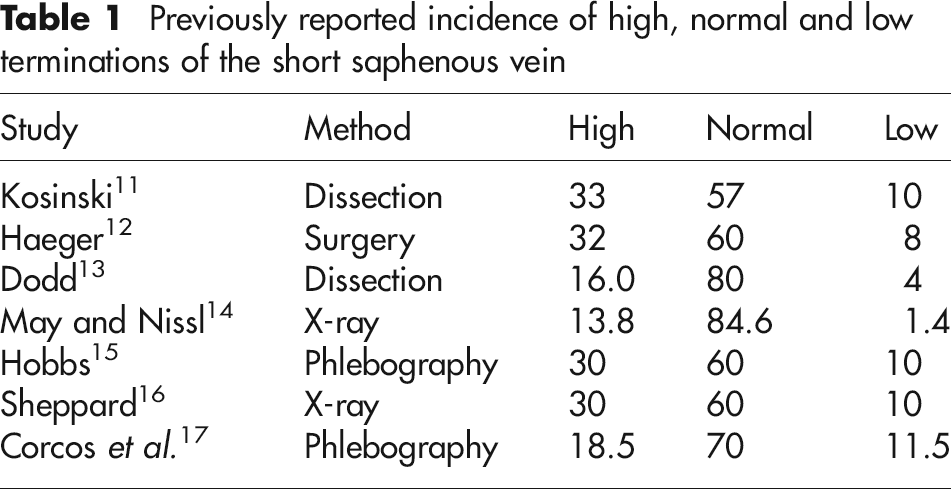
Several studies have investigated variation in the site of the SPJ using different methods and criteria for the classification of SPJ termination (Table 1). 11–17 Vasdekis et al., 18 using Doppler ultrasound, classified a ‘normal SPJ termination’ as being 2–7 cm above the knee joint, with those outside of this range labelled as high and low, respectively. Bergan, 19 using duplex scanning, identified the SPJ in relation to the popliteal skin crease and classified a normal termination as being within 5 cm of the popliteal skin crease. Comparison of these and other studies is made difficult by the lack of a common classification for SPJ termination, with the majority of literature preferring the joint space to knee skin creases as a point of reference for measurements.
Previously reported incidence of high, normal and low terminations of the short saphenous vein
Recent studies have used duplex or venography to determine the anatomy of the SPJ, with the last dissection-based study being conducted by Dodd in 1965. 13,15,20 Dissection-based studies provide more detailed mapping of the course of the SSV, as well as identify its relationship to surrounding nerves.
The common peroneal nerve (CPN) shows little anatomical variation within the popliteal fossa. However, its superficial position makes it potentially vulnerable to retraction injuries at the time of SPJ surgery. 21 CPN injury during SSV surgery was noted in 2% (2/104) of cases by Lucertini et al. 22 In SSV stripping, the close association between the vein and the CPN is the primary reason for nerve injury: the CPN usually runs lateral to the SSV. Injury to the CPN may result in hypoanaesthesia over the anterolateral aspect of the calf and dorsum of the foot, and weakness of ankle dorsiflexion with concomitant foot drop and difficulty in walking. 23,24 These motor abnormalities can take months or years to recover, with full recovery not achieved in some cases. 25,26 There are currently no dissection-based studies that have investigated the anatomical relationship between the SPJ and CPN.
The aim of the present study was to determine the variation of the SPJ, its relationship to the CPN, and the relationship of both SPJ and CPN to defined anatomical landmarks to provide appropriate information to avoid complications and nerve damage during surgery.
Method
Thirty lower limbs, from 15 embalmed cadavers used for routine dissection and examination, were made available for study: none of the limbs showed evidence of surgery for venous insufficiency. A transverse skin incision was made at the level popliteal skin crease, with longitudinal incisions extending from each end into the thigh and calf. The skin was reflected exposing the superficial structures and deep fascia, which was then incised in a similar manner. The posterior aspect of each lower limb, including the popliteal fossa, was carefully dissected to expose the SSV and CPN. The SSV was followed from its origin posterior to the medial malleolus to its termination, where the SPJ was identified and cleaned. The CPN was identified and followed from its division from the sciatic nerve to the lateral compartment of the leg as it passes below the head of the fibular. With the SSV, SPJ and CPN exposed and visible, the following measurements, recorded to the nearest 0.1 mm, were taken using Mitutoyo calipers (Mitu-toyo, UK).
SPJ termination
The direct, i.e. diagonal, and vertical distances from the SPJ to specific anatomical landmarks (fibula head, lateral joint space, lateral femoral epicondyle) were measured (Figure 1): it was decided that measuring the angle between the SPJ and these landmarks was not appropriate. The diagonal measurements incorporated both vertical and transverse distances producing a radial area in which the SPJ was located (see Figure 2). The level of termination of the SSV was classified as high, normal or low in relation to the lateral femoral epicondyle, an easily palpable anatomical land-mark which was approximately equal to the level of the popliteal skin crease. An SPJ below the lateral femoral epicondyle was classified a low termination, while one more than 100 mm vertically above it was classified a high termination; terminations between these boundaries were classified as normal (Figure 3).
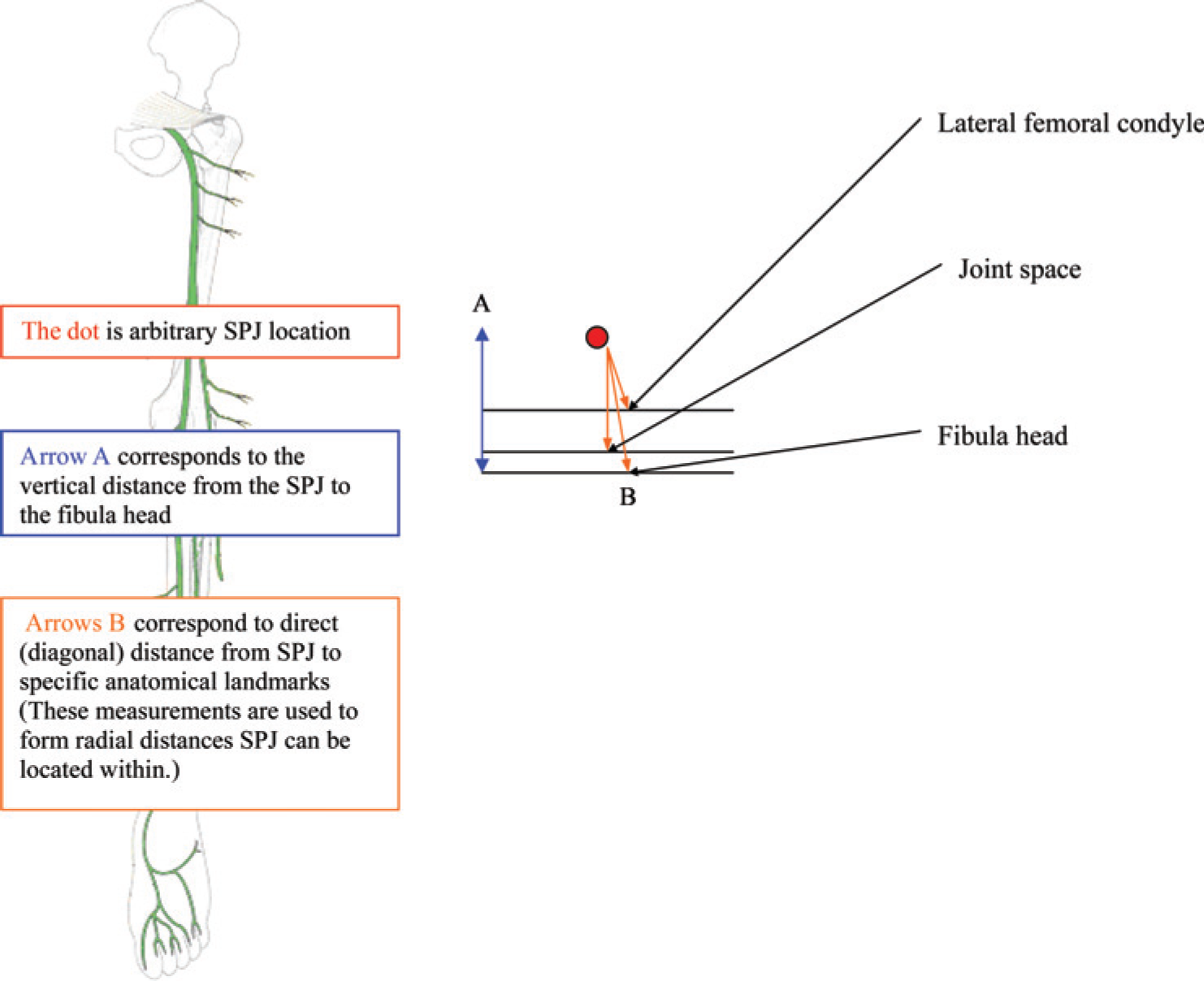
Diagram showing the measurements from the saphenopopliteal junction to specific anatomical landmarks

Radial areas within which the SPJ is located from the lateral femoral epicondyle. The same principle can be applied to the measurements mapping the radial location of the SPJ from the fibula head and lateral joint space

Variations of levels of termination of the SPJ observed in the present study. Low termination: below level of lateral femoral epicondyle (LFE); Low normal: <33 mm above LFE (55–85 mm above fibula head); Middle normal: 33–66 mm above LFE (85–115 mm above fibula head); Upper normal: 66–99 mm above LFE (115–145 mm above fibula head); High termination: >100 mm above LFE
Distance between SPJ and CPN
The horizontal distances from the midpoint of the CPN to the same anatomical landmarks were also measured, as were the direct horizontal distances between the SPJ and the CPN at the level of the landmarks.
All measurements were standardized to account for differences in limb size: vertical measurements were expressed as a percentage of the distance from the lateral malleolus to the lateral aspect of the fibula head; horizontal measurements were expressed as a percentage of knee width at the level of the knee joint space.
Results
Saphenopopliteal junction
The site of SPJ was found to be variable: of the 30 limbs investigated, two (6.7%) were classified high terminations, 21 (70%) normal and seven (23.3%) as low terminations. The group of normal terminations was further subdivided into low, middle and upper to provide a more accurate mapping of SPJ (Figure 2): 20/21 (95%) of normal terminations were within 66 mm above the lateral femoral epicondyle. With respect to the lateral aspect of the fibula head, 66% (20/30) of the all limbs had SPJs between 55 and 115 mm proximal to the lateral aspect of the fibula head (Table 2).
Direct (diagonal) distance (mm) from the SPJ to specific anatomical landmarks
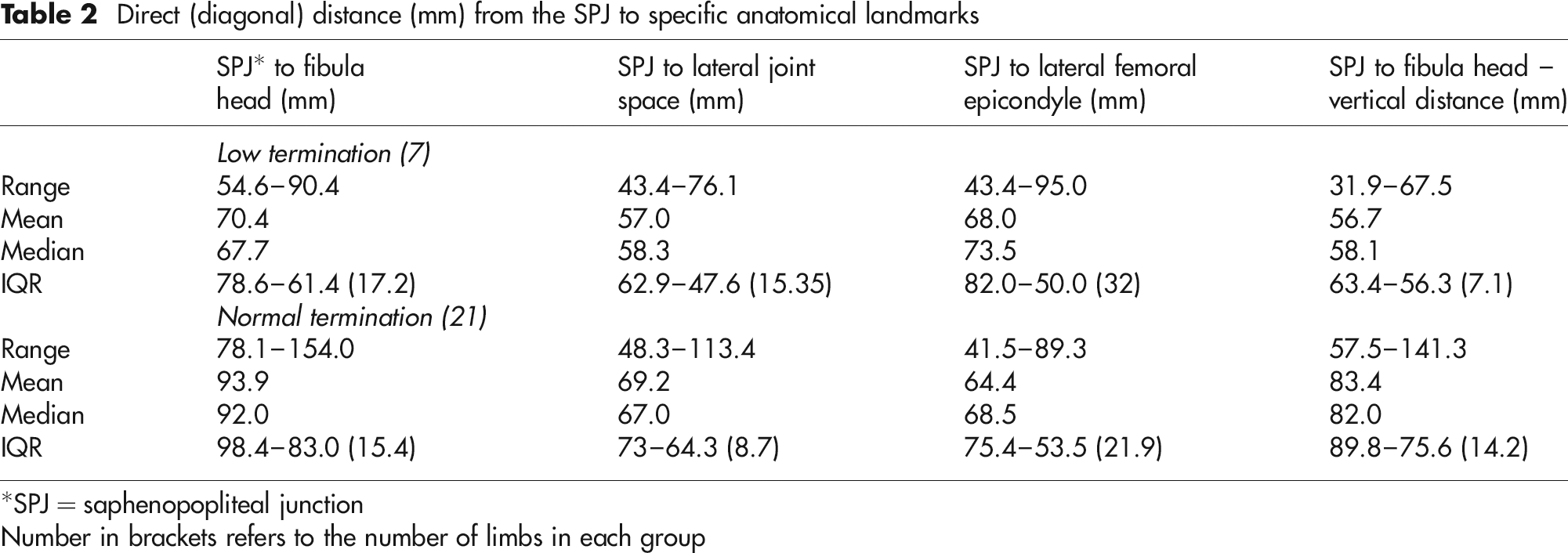
*SPJ = saphenopopliteal junction
Number in brackets refers to the number of limbs in each group
The mean, range, median and associated inter-quartile range (IQR) of the distances from the SPJ to each anatomical landmark are presented in Table 2; in the two cases of high termination, the SSV was not followed into the thigh and measurements were not made. The median value of the distances from the SPJ to each anatomical landmark was significantly greater in normal than in low terminations except for the distance from SPJ to lateral femoral epicondyle. Each of the direct (diagonal) measurements from SPJ to the anatomical landmarks showed a higher IQR in low termination compared with normal terminations. In contrast, the vertical distance from SPJ to the fibula head showed an increase in IQR from low to normal terminations (7.1–14.2).
Short saphenous vein
An incidental finding of the study was that the SSV had a second termination in 53% (16/30) of the limbs studied. One SSV formed a double branch termination into the popliteal vein, while the remaining 16 were identified as the vein of Giacomini ascending into the thigh. The majority of these double terminations occurred bilaterally with six cadavers (12 of 16 limbs) having a vein of Giacomini in both limbs.
Common peroneal nerve
The mean, median, range and IQR values for the CPN with respect to the horizontal distances from the anatomical landmarks followed a trend similar to that with the SSV, with the smallest values being from the fibula head (most inferior landmark) and the largest values from the lateral femoral epicondyle (most superior landmark) (Table 3).
Horizontal distance (mm) of the common peroneal nerve from specific anatomical landmarks

*CPN, common peroneal nerve
The horizontal distance between the SPJ and CPN was determined in 28 of the 30 limbs studied. Both the mean and median distance between the SPJ and CPN was reduced in normal compared with low terminations: median 22.9 mm in low compared with 15.4 mm in normal terminations. Comparison of the IQR of low (7.15) and normal (6.0) terminations showed similar values.
The normalized data showed that the measure-ments were not significantly affected by variations in limb length; furthermore, intra-observer measurements were in statistical concordance with the original results (assessed using Bland and Altman method of assessment of clinical measurement). 27
Discussion
The saphenopopliteal junction
Inaccurate mapping of the SPJ prior to surgery is a recognized cause for the high recurrence rate associated with SSV surgery. 18 Preoperative mapping of the SPJ on the skin surface at the time of surgery can improve these complication rates. 28 Techniques for locating the SPJ include venography and duplex scanning, both of which can identify anatomical variations in SSV termination: venography, however, appears to be the more accurate. 29 In locating the SPJ within the popliteal fossa, Vasdekis et al. 18 reported 100% accuracy using venography compared with 96% with duplex scanning. This compares favourably with the findings of De Maeseneer et al. 20 who reported an accuracy of 100% in locating the SPJ using duplex scanning: they further argued that it was a non-invasive alternative to venography. The accuracy of both these techniques in locating the SPJ was determined by comparing the results with operative findings. However, venography is rarely used in modern clinical settings and neither technique is as accurate in identifying high or low SPJs.
A large variation was observed in the level of SPJ termination in the present study. Using the lateral femoral epicondyle, which effectively equates to the popliteal skin crease used by Bergan 19 and Farrah et al., 7 7% (2/30) were classed as high, 70% (21/30) as normal and 23% (7/30) as low terminations. The incidence of high termination was lower than the 18.5% reported by Corcos et al. 17 and the 33% by Kosinski. 11 Conversely, the proportion of low terminations was more than double that reported by Corcos et al. 17 The high proportion of low terminations in the present study may be due to the inclusion of terminations previously classified as normal. Previous studies have tended to classify low terminations as those occurring in the calf, joining the gastrocnemial vein via the midcalf perforator, or the long saphenous vein via a communicating vein. 11,17,18 In the present study, the boundary for low terminations set at a more proximal level, i.e. the lateral femoral epicondyle. Similarly, the boundaries for normal terminations were further apart in this study than previously reported, which would explain the lower incidence of high terminations. In the study by Vasdekis et al. 18 normal SPJ terminations were considered as being between 20 and 50 mm of the knee joint: the present study included SPJs terminating within 100 mm proximal to the lateral femoral epicondyle. Nevertheless, the proportion of normal terminations observed (70%) was similar to that reported by Corcos et al. 17
As a result of the high frequency of SPJs classed as normal termination in this study, this group was subdivided into lower, middle and upper normal terminations (Figure 2). The majority (66.7%) of terminations were in the lower two-thirds of normal termination range, i.e. within 66 mm proximal to the lateral femoral condyle, or between 55 and 115 mm proximal to the vertical distance from the fibula head. These values are in accordance with the results from previous dissection-based studies by Kosinski 11 and Haeger, 12 who both identified approximately 60% of SPJs located within 5 cm above the knee joint.
The vertical distance between the SPJ and fibular head was the only measurement not influenced by the horizontal positioning of the SPJ. However, it showed a higher IQR in normal compared with low terminations suggesting that the higher the SPJ, the more variable its location vertically. The direct (diagonal) measurements showed a reduction in IQR from low to high SPJs suggesting that there is more variation in the SPJ horizontally the lower the SSV termination (Table 4).
Horizontal distance (mm) between the SPJ and the CPN in normal and low terminations of the short saphenous vein
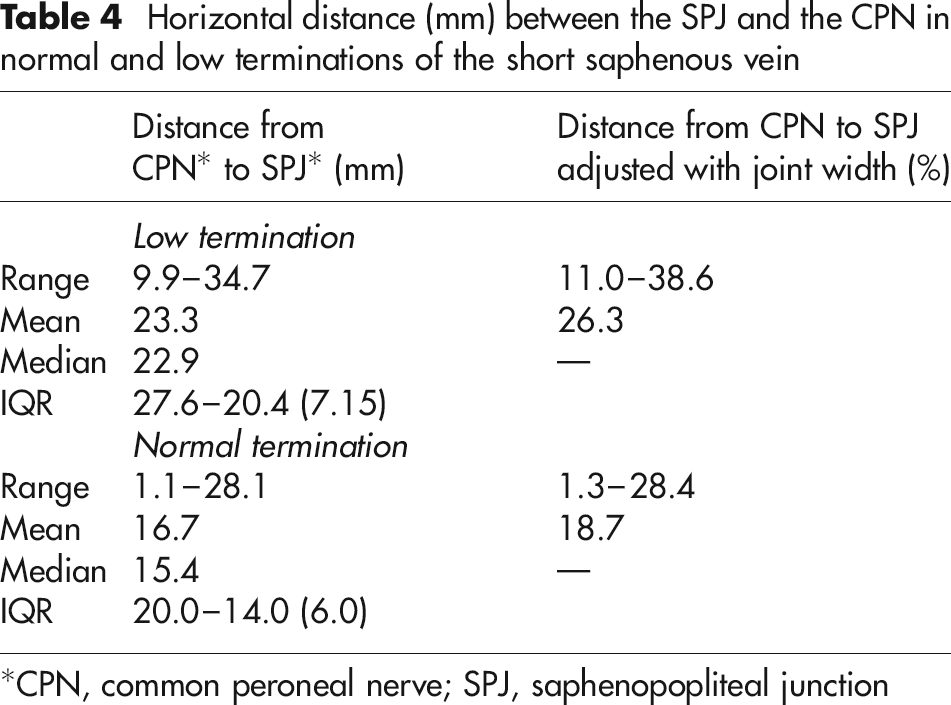
*CPN, common peroneal nerve; SPJ, saphenopopliteal junction
Within the limitations of the present study population of 30, the data in Table 2 can be used to map the location of the SPJ. SPJs located above the lateral femoral epicondyle (i.e. normal terminations) are located superiorly between radial distances of 66 and 100 mm above the lateral femoral epicondyle, while those located below the level of the lateral epicondyle (i.e. low terminations) are located inferiorly between radial distances of 45 and 69 mm (Figure 2). Although application of this data in a clinical setting would be inappropriate, it provides a visual image of the distribution of SPJs. In addition, the IQR can be applied to obtain an estimate of the variation in SPJ termination.
In 53% (16/30) of limbs studied, a vein of Giacomini was observed passing into the posterior thigh as a branch of the SSV. This incidence is less than the 70.4% reported by Delis et al. 30 in their study of 301 limbs: identification of the vein of Giacomini was by duplex ultrasound. This discrepancy could be a result of the smaller sample size in the present study. Delis et al. concluded that the vein of Giacomini was insignificant in regard to its effect on venous incompetence, nevertheless if not ligated and of sufficient calibre, it could result in significant reflux.
Common peroneal nerve
As expected, the CPN becomes progressively more lateral as it passes through the popliteal fossa and upper calf, coming to lie closer to the inferior anatomical landmarks. The largest variation in its horizontal location was at the level of the lateral femoral epicondyle (range 25.5–81.9 mm) and least at the fibula head (range 7.1–21.8 mm). The variability of the course of the CPN at the level of the lateral femoral epicondyle puts it at risk during saphenopopliteal ligation and multiple stab avulsions in or around the popliteal fossa. Normalizing the distance between the CPN and specific anatomical landmarks may help to avoid inadvertent trauma.
The relationship between the CPN and SPJ can provide a valuable clinical guide to the risk of CPN injury during varicose vein surgery. Low SPJs were 23.3 mm from the CPN (range 9.9–34.7 mm), while normal SPJs were 16.7 mm (range 1.1–28.1 mm) suggesting that the higher the SPJ, the closer it is to the CPN. The SPJ is commonly found close to the midline within the popliteal fossa, consequently the CPN is at an increased risk of injury during surgery associated with high SPJ terminations, confirming the views of Critchley et al. 31 Nevertheless, trauma to the CPN during SPJ surgery is a rare, but severe complication and can occur in up to 2% of cases. 22,32 The CPN can be subject to trauma during retraction of the nerve trunk to expose the SPJ as well as during the process of stripping the vein. 1,22 Unlike locating the SPJ, duplex scanning or venography cannot identify the course of the CPN, consequently surgery is effectively ‘blind’ to the course of the CPN within the popliteal fossa.
The present study confirms the anatomical variability of the SPJ location and the close proximity of the CPN and SPJ in the superior part of the popliteal fossa. Above the level of the lateral femoral epicondyle, they become more closely associated, thus increasing the risk of CPN injury: in one case of a normal termination, the CPN and SPJ were only 1.3 mm apart, a situation that potentially places the nerve at risk during surgery. Furthermore, the CPN showed a high degree of variability at the level of the lateral femoral epicondyle (range 25.5–81.9 mm) making intervention potentially precarious.
The present study suggests that surgical intervention in relation to an incompetent SPJ at any level above the lateral femoral epicondyle incurs increased risk of CPN injury, not only because of the close association between the SPJ and CPN but also because of their variability. An awareness of this relationship and an understanding of anatomical variability prior to SPJ surgery should reduce the incidence of varicose vein recurrence and CPN injury. The present findings add weight to the clinical need for routine SPJ duplex marking prior to surgery.