
Abstract
Abstract
Background
Digital photoplethysmography (D-PPG) is a newly introduced method of optical screening of deep vein thrombosis (DVT) by recording changes in the size of limb due to tissue fluid.
Objectives
The objective of this study is to assess the effect of high pulmonary artery pressure (PAP) and consequently increased venous system pressure on D-PPG test results.
Methods
Forty-five patients with and 45 patients without PAP pressure were enrolled in the study and divided into two groups. All the patients had a history of chronic obstructive pulmonary disease (COPD). D-PPG test was performed for both legs of all the patients and the results of the two groups were compared. Also, all patients underwent duplex sonography for ruling out DVT.
Results
Using venous refilling time (RT) of <22 s as the optimal cut-off point, it was found that 32 (35%) legs of patients with and 39 (43%) legs of patients without high PAP had positive D-PPG test. Although the rate of positive D-PPG test was higher in patients with high PAP, this was not statistically significant (P = 0.28). Moreover, overall correlation between RT and venous pump detected by D-PPG and PAP was r = −0.11 (P = 0.2) and r = −0.01 (P = 0.6), respectively.
Conclusion
Our results showed that the rate of positive D-PPG test results is slightly higher in patients with pulmonary hypertension, but this difference is not statistically significant. Therefore, increased PAP could be excluded as a confounding factor of D-PPG test.
Introduction
Digital photoplethysmography (D-PPG) has been recently introduced as a reliable, safe, bedside, easy to perform, non-operator-depending and fully portable method, with a high negative predictive value, which can be used to rule-out a lower limb deep vein thrombosis (DVT). 1–7 Photoplethysmography is the term given to the optical technique of recording of changes in the size of limb due to tissue fluid or pooled blood in the veins. D-PPG is a development of light reflection rheography, which can measure initial local blood volume and can be automatically calibrated for different cutaneous optical densities according to different skin colour and thickness. D-PPG measures the refilling time (RT) of calf veins during rest after they have been emptied by exercise by measuring the extent of blood displacement from the calf veins, based on the absorption of emitted infrared light by haemoglobin in red cells, and characteristics of the reflected light from dermal microcirculation. 1,8 Moreover, different studies have shown that RT measured by D-PPG has an acceptable correlation with directly measured intravenous pressure. 9–11 Furthermore, according to the percentage of displacement of initial blood content, D-PPG can verify the efficacy of calf pump. In cases of DVT with obstruction of the calf veins outflow, the rate of blood displacement decreases and consequently venous RT and venous pressure are reduced.
The lower limb venous system can be divided into the deep and superficial veins, interconnected along the leg by a series of perforator veins. The superficial veins drain to the deep ones. The deep venous system drains to the common iliac vein and subsequently into the inferior vena cava (IVC), and right atrium and ventricle of the heart. Eventually, the right side of the heart is connected to the lungs by the pulmonary arteries.
These data raise the question of whether increased pulmonary artery pressure (PAP) could affect backward the pressure and RT of the deep venous system, and consequently the result of D-PPG test. To assess this hypothesis, we prospectively compared the results of D-PPG test in two groups of chronic obstructive pulmonary disease (COPD) patients with and without high PAP, respectively.
Methods
Design
A prospective, single-centre case-control study was employed at the Thrombosis Clinic of Cardiology Department of the National Research Institute of Tuberculosis and Lung Disease (NRITLD), Masih Daneshvari Hospital, Tehran, between November 2005 and April 2006. The study involved patients presenting with COPD to the pulmonary department who were referred for cardiology consultation. Approval of the Research Review Committee was obtained at the NRITLD and informed written consent was obtained from all participating patients.
Study population
Among 90 subjects (180 legs) recruited in this study, there were 45 patients (38 men; age 59.44 ± 8 years; body mass index [BMI] 23.4 ± 2.1 kg/m2) with PAP >40 mmHg who had suffered from COPD concomitantly. This case group was compared with 45 COPD patients (35 men; age 62.44 ± 5 years; BMI 22.6 ± 1.9 kg/m2) with PAP <40 mmHg. The patients were excluded if they had: (1) current or previous DVT or pulmonary embolism documented by objective testing or medical records; (2) current or previous history of venous diseases including varicose and venous insufficiency; (3) history of concomitant systemic diseases which could influence the pressure of the venous system, including congestive heart disease and hepatic disorders; (4) current or previous history of arterial diseases; and (5) pulmonary valve stenosis or right ventricular (RV) outflow tract obstruction detected as an echocardiographic finding.
Digital photoplethysmography
The examinations were performed with a fully automatic and printout-capable system (Rheo Dopplex II PPG Huntleigh Diagnostics Ltd, Cardiff, UK) according to the manufacturer's protocol, which had been established previously. 1,12 When the test was performed satisfactorily, venous RT and venous pump (VP), which were deemed as the results of the D-PPG test, were calculated with the unit and displayed on liquid crystal display. Moreover, a printout of venous RT, VP as well as blood flow waveform was produced at the same time as a recordable document. The results of the test were compared between the case and the control groups.
Pulmonary artery pressure measurement
PAP in all patients was determined echocardiographically (Diagnostic Ultrasound System, Model Nr. HDI-3500CV, ATL Ultrasound, USA) by an expert cardiologist who was blinded to the D-PPG results, using tricuspid regurgitation velocity (TRV). TRV was obtained with continuous wave Doppler from RV inflow or the apical four-chamber view position. As TRV reflects the pressure difference during systole between the right ventricle (RV) and the right auricle (RA), systolic RV pressure was estimated by adding RA pressure to the transtricuspid gradient derived from TRV using the following equilibrium:
Transtricuspid pressure gradient = 4 * TRV 2
The RA pressure was estimated from the respiratory motion of IVC seen on two-dimensional echocardiograms. Once the diameter of the IVC decreased by 50% or more with inspiration, RA pressure was considered to be 5 mmHg, and those with <50% inspiratory collapse were considered to have an RA pressure of 15 mmHg. 13
All measurements were recorded when the patient had rested for 20 min and was clinically stable. Furthermore, the D-PPG test was performed within 1 h after PAP determination. Therefore, all reasons for a variable PAP were excluded.
Duplex sonography
Duplex assessment of the deep venous system for patency and excluding the presence of DVT was carried out in all patients using Diagnostic Ultrasound System. The main diagnostic criterion used to exclude DVT was complete collapse of the veins under transducer pressure. 14 Colour flow imaging, as well as spectral Doppler, was also used during the assessment.
Statistical analysis
The continuous variables were described as mean ± SD and the categorical variables as percentages. Data were analysed using SPSS for Windows version 11.0 (SPSS Inc, Chicago, IL, USA). The Spearman method was used to assess the correlation between PAP and RT as well as PAP and VP. Mean values of continuous variables were compared with Student's t-test and Mann-Whitney test was used for the comparison of D-PPG results between the groups. A value of P < 0.05 was considered significant.
Results
Two patients were excluded because of history of previous DVT and concomitant severe congestive heart failure; however, no patient was excluded because of inappropriate cooperation. The D-PPG test, as well as echocardiographic measurement of PAP, was performed successfully in all patients, and reproducibility of the D-PPG test was evaluated by repeated studies in all subjects after removal and reconnection of the equipment. There were no significant differences in baseline characteristics between the pulmonary hypertensive and normotensive groups (P = 0.41, P = 0.67 and P = 0.5 for sex, age and BMI, respectively).
Considering RT of <22 s (based on the manufacturer's protocol) as ‘positive’, 32 (35%) legs of patients with and 39 (43%) legs of patients without high PAP had positive D-PPG test. Although the rate of positive D-PPG test was higher in patients with high PAP, this was not statistically significant (P = 0.28). In addition, using the Spearman rank correlation coefficient, overall correlation between RT and VP detected by D-PPG and PAP, which was measured echocardiographically, were r = −0.11 (P = 0.1) and r = −0.01 (P = 0.8), respectively. Therefore, increasing PAP is not associated with changes of RT or VP (Figures 1 and 2).

Scatter plot shows non-significant correlation between pulmonary artery pressure and refilling time among participants (correlation coefficient = −0.11, P = 0.1)
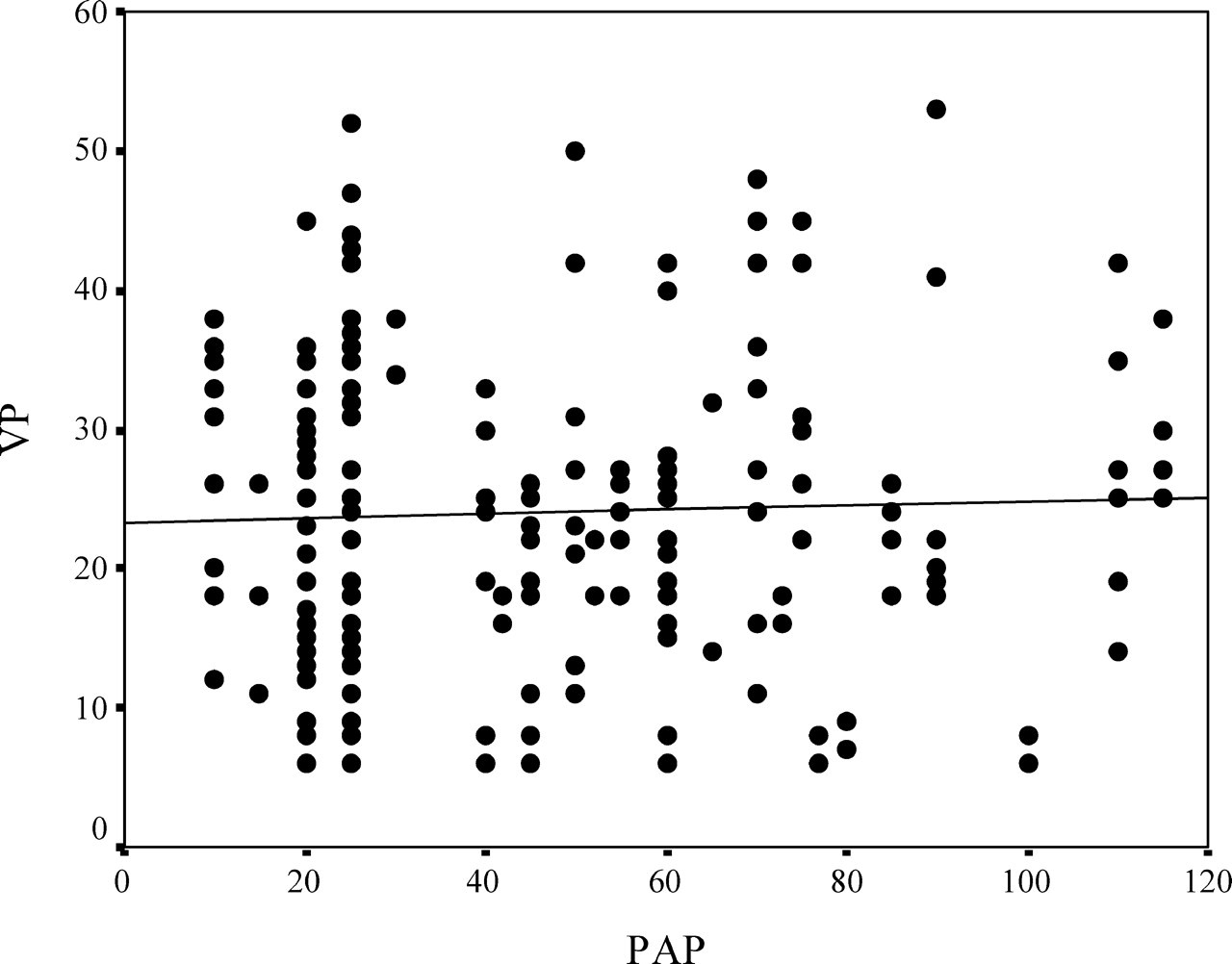
Scatter plot shows non-significant correlation between pulmonary artery pressure and venous pump among participants (correlation coefficient = −0.01, P = 0.8)
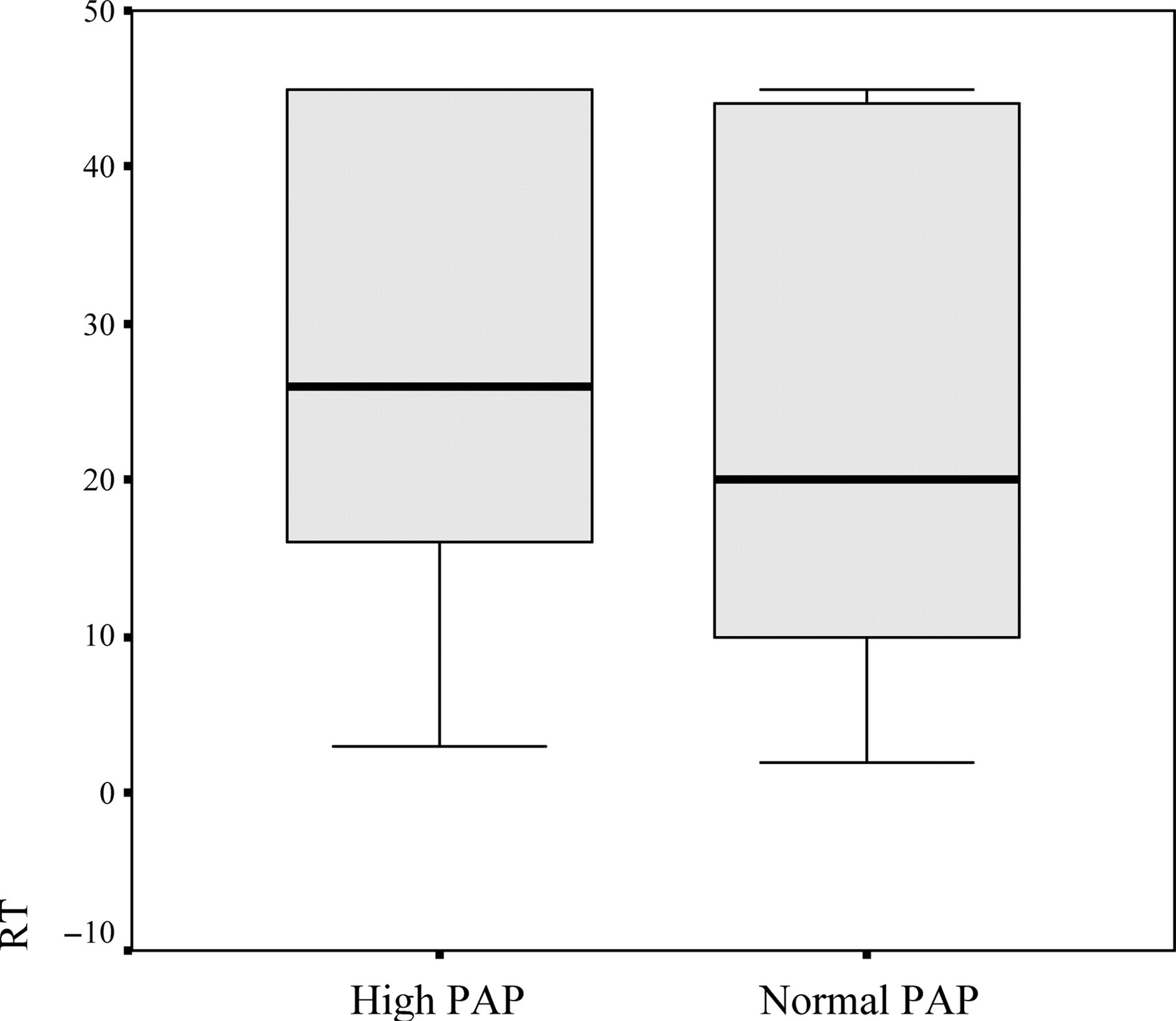
Furthermore, there were no significant differences of RT (P = 0.2) and VP (P = 0.6) measures between the patients with and without high PAP (Figures 3 and 4).
Comparison of refilling time measures between patients with and without high pulmonary artery pressure. Data are shown as 25th, 50th and 75th percentiles; P = 0.2

Comparison of venous pump measures between patients with and without high pulmonary artery pressure. Data are shown as 25th, 50th and 75th percentiles; P = 0.6
Discussion
To our knowledge this is the first study evaluating the possible effect of high PAP as a possible confounding factor on the results of D-PPG. Although the results of several studies support the worth of D-PPG as a reasonably accurate, practical, non-invasive and inexpensive screening test for DVT, 1–7 increased venous system pressure has not been assessed as a confounding factor yet.
The network nature of venous system and given the fact that any changes in subcutaneous microvasculature pressure could directly affect the results of the D-PPG test, led us to hypothesize that raising venous pressure in any sites of venous system including pulmonary venous system may influence backward the results of the D-PPG test.
To evaluate this hypothesis, we compared the results of the D-PPG test in two groups of patients suffering from COPD with and without increased PAP, respectively.
The main finding of this study is that increase of PAP is not associated with significant alteration in the D-PPG results and, consequently, sustains the usefulness of D-PPG in screening of patients who are at high risk of developing DVT. Several interpretations of our finding are possible. One explanation might be that numerous bicuspid venous valves of lower limbs withstand high degrees of back pressure, typically in excess of 250–300 mmHg. 15 They are present in more numbers in the distal veins and possibly can resist against conducting higher proximal venous pressures to the extremities. 15 An alternative elucidation may be that, even though less than arteries, natural elasticity of venous wall from lungs to inferior limbs makes high pressure of pulmonary veins neutralized gradually; thereby, increased pressure of pulmonary venous system is deactivated while getting to the inferior limbs.
There are two main limitations to our study that should be acknowledged. First, virtually all the study patients were referred from pulmonary wards for cardiological consultation. Thus, the subjects were nearly selected from the inpatients, where the venous pressure of the lower extremities might be influenced by long-term effect of hospitalization. Hence, it is not clear, however, that our conclusion can be generalized to the outpatients, in which walking and standing possibly affect blood volume and consequently the pressure of the lower limbs. Secondly, the study setting applied only to patients presenting with just one type of clinical setting that is accompanied with increased venous system pressure, COPD. Therefore, our conclusion may probably relate to a particular group of patients, exclusively. Further studies with larger numbers and more types of patients are needed to improve the robustness of our conclusion and to determine likely confounding factors of the D-PPG test.
Conclusion
The increase of PAP is not associated with significant change in the rate of D-PPG positive results. Therefore, increased PAP could be excluded as a confounding factor of D-PPG test.