
Abstract
Objectives
The degree of benefits and risks, and the role of subfascial endoscopic perforator vein surgery (SEPS) in the management for chronic venous insufficiency (CVI) remains uncertain.
Methods
A multiple health database search was performed including Medline, Embase, Ovid, Cochrane Database of Systematic Reviews, and Cochrane Database of Abstracts of Reviews of Effectiveness, on all studies published between 1985 and 2008 that reported on health outcomes in patients with CVI treated with SEPS and comparing this therapy with the conventional Linton procedure. Three studies, which compared SEPS with conventional surgery, were included in the present meta-analysis.
Results
Between SEPS and Linton groups, there was a significant lower rate of wound infections for SEPS (odds ratio [OR] 0.06 [95% confidence interval (CI) 0.02 to 0.25]) and a significantly reduced hospital stay for SEPS (OR –8.96 [95% CI –11.62 to –6.30]). In addition, SEPS was associated with a significant reduced rate of recurrent ulcers (mean follow-up 21 months) (OR 0.15 [95% CI 0.04–0.62]).
There was no significant difference between the groups in the following dimensions: rate of hospital re-admission (OR 0.21 [95% CI 0.03 –1.31]), death at six months (OR 3.00 [95% CI 0.11–78.27]), ulcer healing rate at four months (OR 0.44 [95% CI 0.09–2.12]), and the rate of deep vein thrombosis (DVT) (OR 0.35 [95% CI 0.01–8.85]).
Conclusion
From the level of evidence available by now it seems that SEPS, used as a part of a treatment regimen for severe CVI, benefits most patients in the short term regarding ulcer healing and the prevention of ulcer recurrence. It can be safely performed with less early postoperative complications compared with the Linton procedure. However, further prospective randomized trials are required to define the long-term benefits of SEPS.
Introduction
As a treatment of venous ulcers, interruption of incompetent perforating veins (IPVs) was first suggested by Linton in 1938, 1 in order to decrease abnormal transmission of pressure from the deep to the superficial vein, and thereby favourably effect venous haemodynamics and clinical outcome in advanced chronic venous insufficiency (CVI). Although some studies have reported good results with Linton's original operation, morbidity related to wound complications has led many to abandon this procedure, which required a long skin incision. 2 Subsequently proposed operations using shorter skin incisions were either incomplete or similar to Linton's operation, but also resulted in frequent wound complications. Subfascial endoscopic perforator vein surgery (SEPS) was first performed in Germany by Hauer in 1985 3 to replace the open technique. Because of the minimally invasive nature of the procedure, combined with a lesser rate of wound complications SEPS is performed in many centres as a component of a comprehensive treatment programme for venous insufficiency, 4 with encouraging early and mid-term results. 5–9 The safety, feasibility and efficacy of SEPS has been established in the North American SEPS (NASEPS) Registry, 9 and in several non-randomized single- and multicentre case series often without comparison treatment groups, so that the usefulness of SEPS in patients with venous disease remains uncertain. So far, only a few studies have compared SEPS with the Linton procedure. When there is controversy regarding the efficacy of an intervention, a meta-analysis of the literature to summarize the available data may be helpful. The aim of the present meta-analysis is to summarize the best available evidence on the ulcer healing, recurrence rates and morbidity of SEPS for treatment of venous disease compared with open perforator vein ligation.
Patients and methods
Study selection
A multiple health database search was performed, including Medline, Embase, Ovid, Cochrane Database of Systematic Reviews and Cochrane Database of Abstracts of Reviews of Effectiveness, on all studies published between 1985 and 2007 describing SEPS and comparing this therapy with conventional Linton procedure. These databases were searched with an unrestricted search strategy, using exploded medical subject heading (MeSH) terms (‘SEPS’, ‘subfascial endoscopic perforator surgery’, ‘varicose vein’, ‘venous surgery’, ‘varicose ulcer’, ‘leg ulcer surgery’, ‘minimally invasive surgery’, ‘endoscopic surgery’, ‘CVS’, ‘perforator vein’, ‘Linton operation’) and specific textword terms for transilluminated powered phlebectomy (‘SEPS $’, ‘Linton $’). The dollar sign was used to retrieve all possible suffix variations of the root word or phrase. In addition, to improve the specificity of these searches, the above terms were restricted using a search filter to identify randomized controlled trials (RCTs).
Inclusion criteria
To be included, a study must have reported the number of patients with active ulceration at the time of SEPS and with ulcer healing during follow-up. In addition to that, studies had to report on at least one of the other outcome measures mentioned below and contain a previously unreported patient group. When two studies with overlapping time periods were reported by the same institution, either the one of better quality or the more recent publication was included in the analysis. Included papers provided data on patients over the age of 18 years with clinically documented primary symptomatic varicose veins attributable to saphenofemoral junction (SFJ) incompetence and long saphenous vein reflux, confirmed using duplex ultrasonography. All limbs treated with SEPS had at least one IPV identified using the duplex scan and had skin changes, or a healed or an active (open) ulcer on the medial part of the lower leg (clinical, aetiological, anatomical and pathological elements [CEAP] classification 4, 5 or 6 disease). Because there were only two RCTs, we included another retrospective study comparing SEPS with conventional surgery in our meta-analysis.
Outcomes of interest and definitions
The primary outcomes for assessing safety were mortality and morbidity, including procedure-specific adverse events and complications. Complications included in the analysis were infection and deep venous thrombosis (DVT). Effectiveness was assessed by the rate of healing and recurrences, operating time, blood loss and hospital stay. We defined overall healing as the number of patients with class 6 disease that healed by the time of the latest reported follow-up, but we also collected data on healing within four months. Ulcer recurrence was recorded for patients with class 5 and 6 disease that had healed after SEPS.
Quality of trials
The assessment of study quality was based on the methods described by Jadad 10 for randomized studies.
Statistical analysis
Statistical analysis for categorical variables was carried out using the odds ratio (OR) as the summary statistic. An OR of <1 favours the endovenous group and the point estimate of the OR is considered statistically significant at the P <0.050 level if the 95% CI does not include the value 1. The Mantel–Haenszel method was used to combine the OR for the outcomes of interest using a random effects meta-analytical technique. Yates' correction was used for those studies that contained a zero in one cell for the number of events of interest in one of the two groups. 11,12 For continuous variables, statistical analysis was carried out using the weighted mean difference (WMD) as the summary statistic. 13 For studies that presented continuous data as mean (range) values, the standard deviations were calculated using statistical algorithms and checked using ‘bootstrap’ re-sampling techniques.
Two strategies were used to assess heterogeneity quantitatively. First, data were re-analysed using both random and fixed-effects models. Second, graphical exploration with funnel plots was used to evaluate publication bias. 14,15
Analysis was conducted using the statistical software Statistical Package for Social Sciences (SPSS 12.0, Chicago, IL, USA) for Windows and Review Manager Version 4.2 (The Cochrane Collaboration, Update Software, Oxford, UK).
Results
Studies selected
After the application of inclusion criteria, 126 papers were retrieved for full text appraisal. Three studies, 2,16,17 comparing SEPS with the open (Linton) perforating vein surgery, were included in the present meta-analysis. Of these, two were prospective randomized trials and one trial reported about retrospectively collected data. The characteristics of the included studies are summarized in Table 1.
Study characteristics and outcomes
Meta-analysis
The three studies selected contained a combined total of 118 subjects, 60 (51%) of whom underwent SEPS and 58 (49%) the Linton procedure. The outcomes of interest reported by each of the three studies are summarized in Table 1.
Figures 1–7 are forest plots showing the results of meta-analysis of outcomes for SEPS versus Linton procedure.
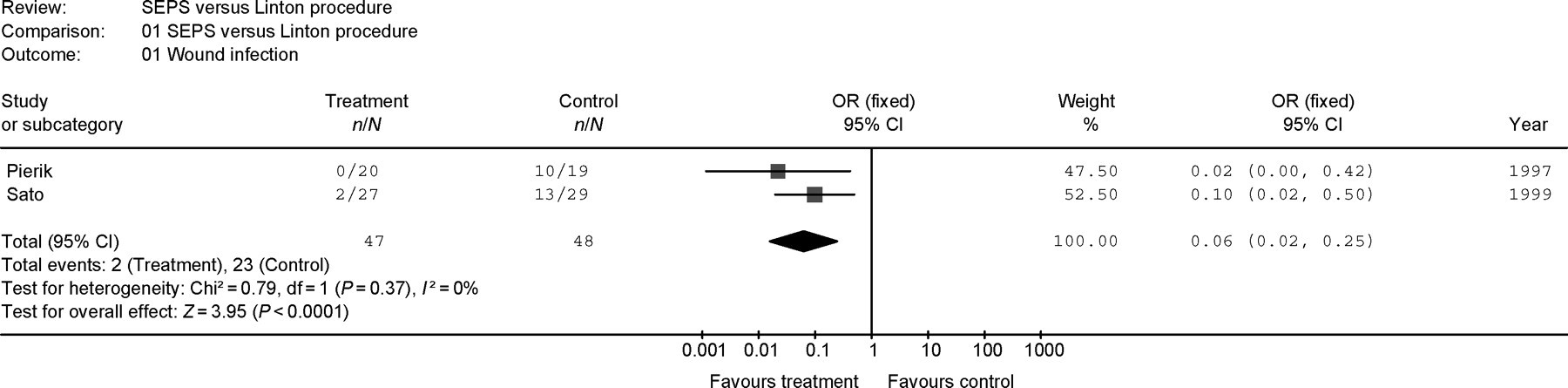
The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Wound infection’. Results are expressed as odds ratio with a fixed-effects model
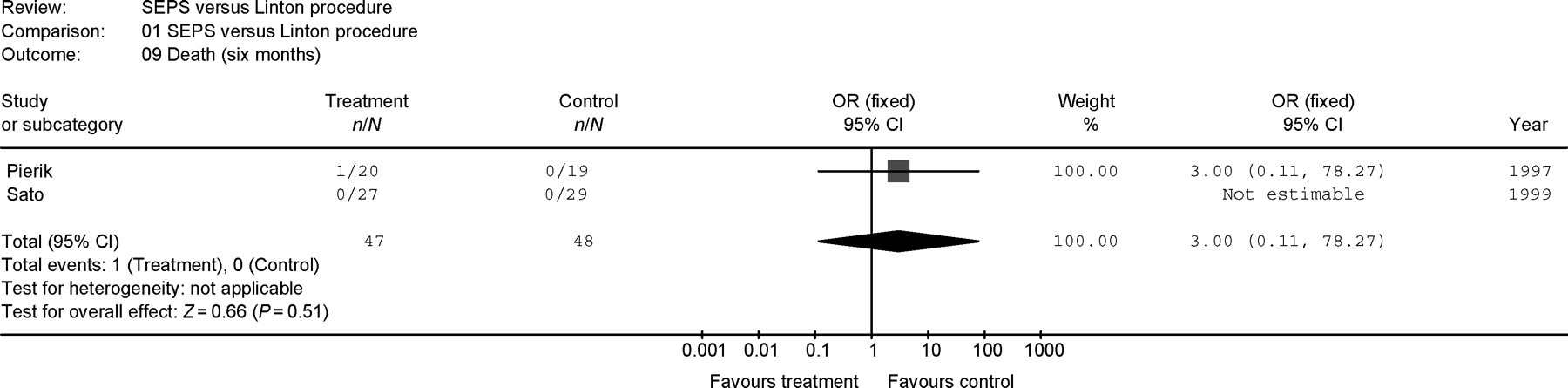
The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Death (6 months)’. Results are expressed as odds ratio with a fixed-effects model
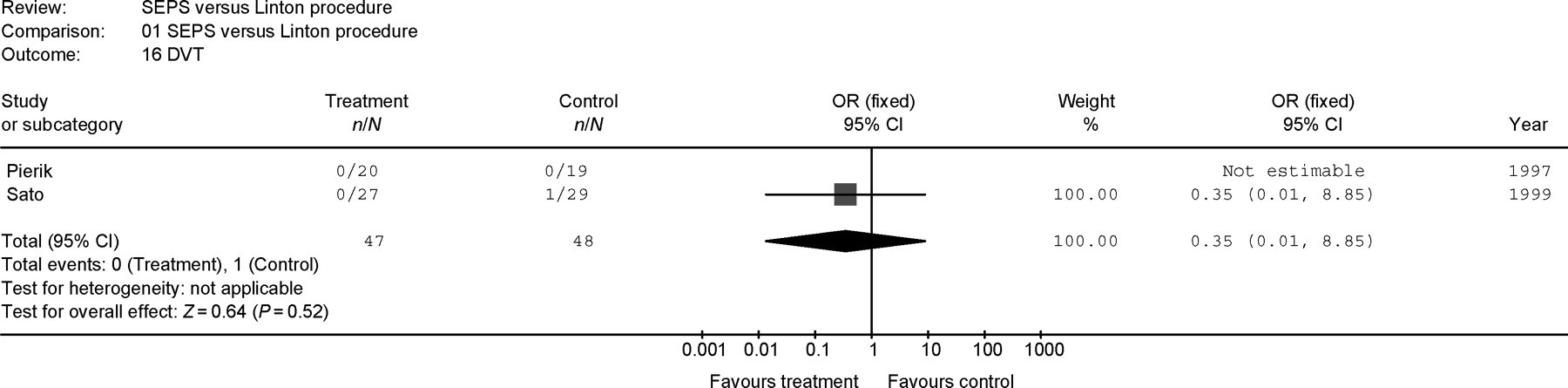
The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Deep vein thrombosis’. Results are expressed as odds ratio with a fixed-effects model

The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Hospital stay (days)’. Results are expressed as odds ratio with a fixed-effects model
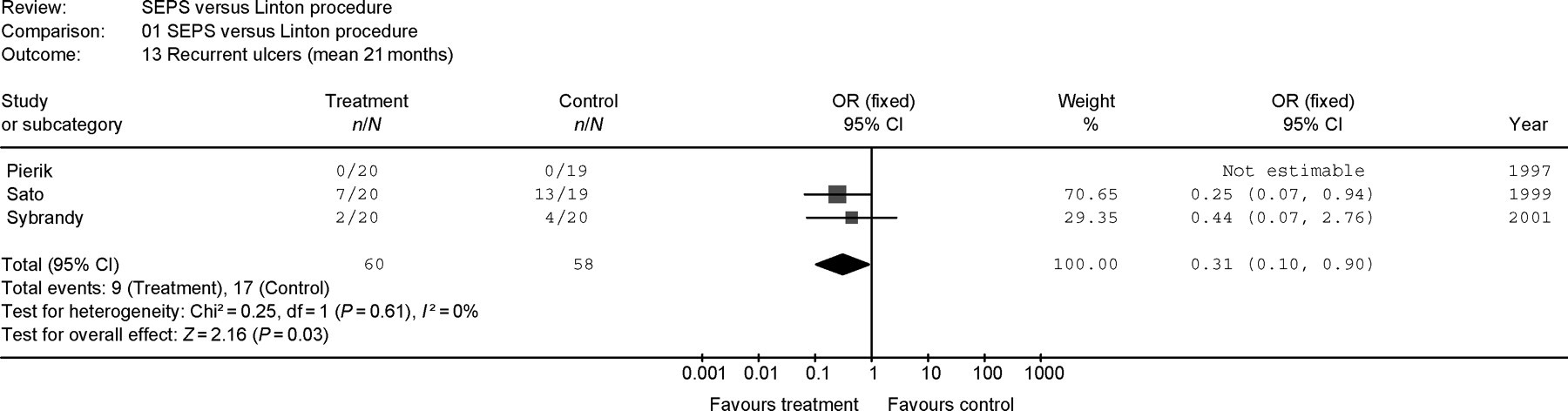
The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Recurrent ulcers (mean 21 months)’. Results are expressed as odds ratio with a fixed-effects model

The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Readmission’. Results are expressed as odds ratio with a fixed-effects model
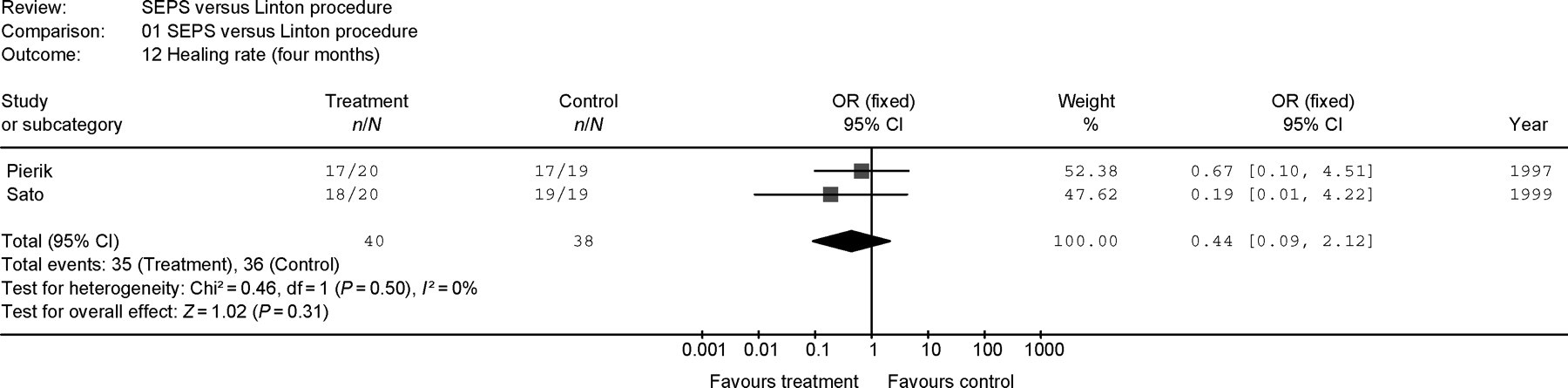
The effect of subfascial endoscopic perforator vein surgery versus Linton procedure on the combined outcome ‘Healing rate (4 months)’. Results are expressed as odds ratio with a fixed-effects model
Meta-analysis of postoperative complications
Regarding the effect sizes analysed in at least two studies, there was a significantly reduced rate of wound infections for SEPS compared with the Linton procedure (OR 0.06 [95% CI 0.02–0.25]) (Figure 1). As expected, there was no significant difference between the groups in the following postoperative complications: death at six months (OR 3.00 [95% CI 0.11–78.27]) (Figure 2), and the rate of deep vein thrombosis (DVT) (OR 0.35 [95% CI 0.01–8.85]) (Figure 3).
Meta-analysis of effectiveness of treatment
Concerning the outcomes quantified in more than one study, between SEPS and Linton groups, there was a significantly reduced duration of hospital stay for SEPS (OR –8.96 [95% CI –11.62 to –6.30]) (Figure 4). In addition, SEPS was associated with a significantly lower rate of recurrent ulcers (mean follow-up 21 months) (OR 0.31 [95% CI 0.1–0.90]) (Figure 5).
There was no significant difference between the groups in the following dimensions: rate of hospital readmission (OR 0.21 [95% CI 0.03–1.31]) (Figure 6) and ulcer healing rate at four months (OR 0.44 [95% CI 0.09–2.12]) (Figure 7).
A single study 17 explored the operating time of the two procedures and found no significant difference between them (WMD 2.00 [95% CI –7.58 to 11.58]). Furthermore, this study showed no significant variation in blood loss between SEPS and the Linton procedure (WMD –127.00 [95% CI –161.01 to –92.99]), and there was no dissimilarity in the number of missed veins during the operation (OR 7.8 [95% CI 0.38–161.87]). In addition, Pierik et al. 17 assessed the the signs of superficial or perforating vein incompetence with postoperative duplex ultrasound scans after six weeks and showed no difference between the two procedures (OR 10.64 [95% CI 0.53–212.44]). These results are stressed by Sybrandy et al. 16 who could not demonsrate any difference in the number of patients with IPVs, evaluated 48 months postoperatively by means of duplex ultrasonography (OR 0.86 [95% CI 0.16–4.47]). Finally, Sato et al. 2 showed that no significant difference exists between the two surgical techniques regarding the time until ulcer healing and until ulcer recurrence (WMD –2.6 [95% CI –6.22 to 1.02]) and (WMD –11.5 [95% CI –24.75 to 1.75]), respectively.
Publication bias
To test whether publication bias was present within the above sample included in the meta-analysis, a funnel plot was undertaken (Figures 8 and 9). None of the studies lay outside the limits of the 95% CI. The funnel plot shows marked asymmetry, but the pattern is not consistent with publication bias, all studies being equally distributed around the vertical axis.
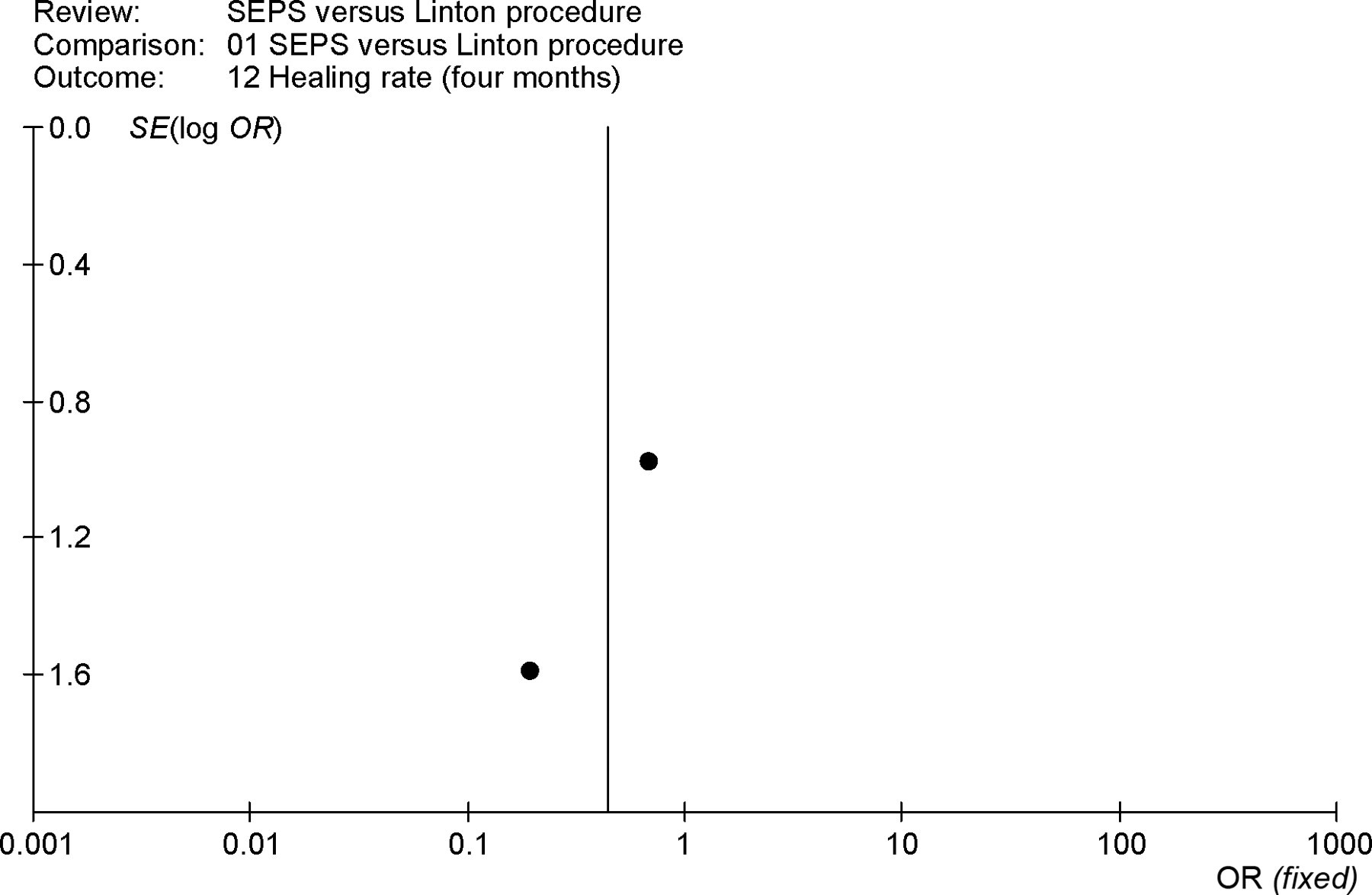
Assessment of publication bias using a funnel plot on the outcome ‘Healing rate (4 months)’: the funnel plot shows marked asymmetry, but the pattern is not consistent with publication bias, all studies being equally distributed around the vertical axis
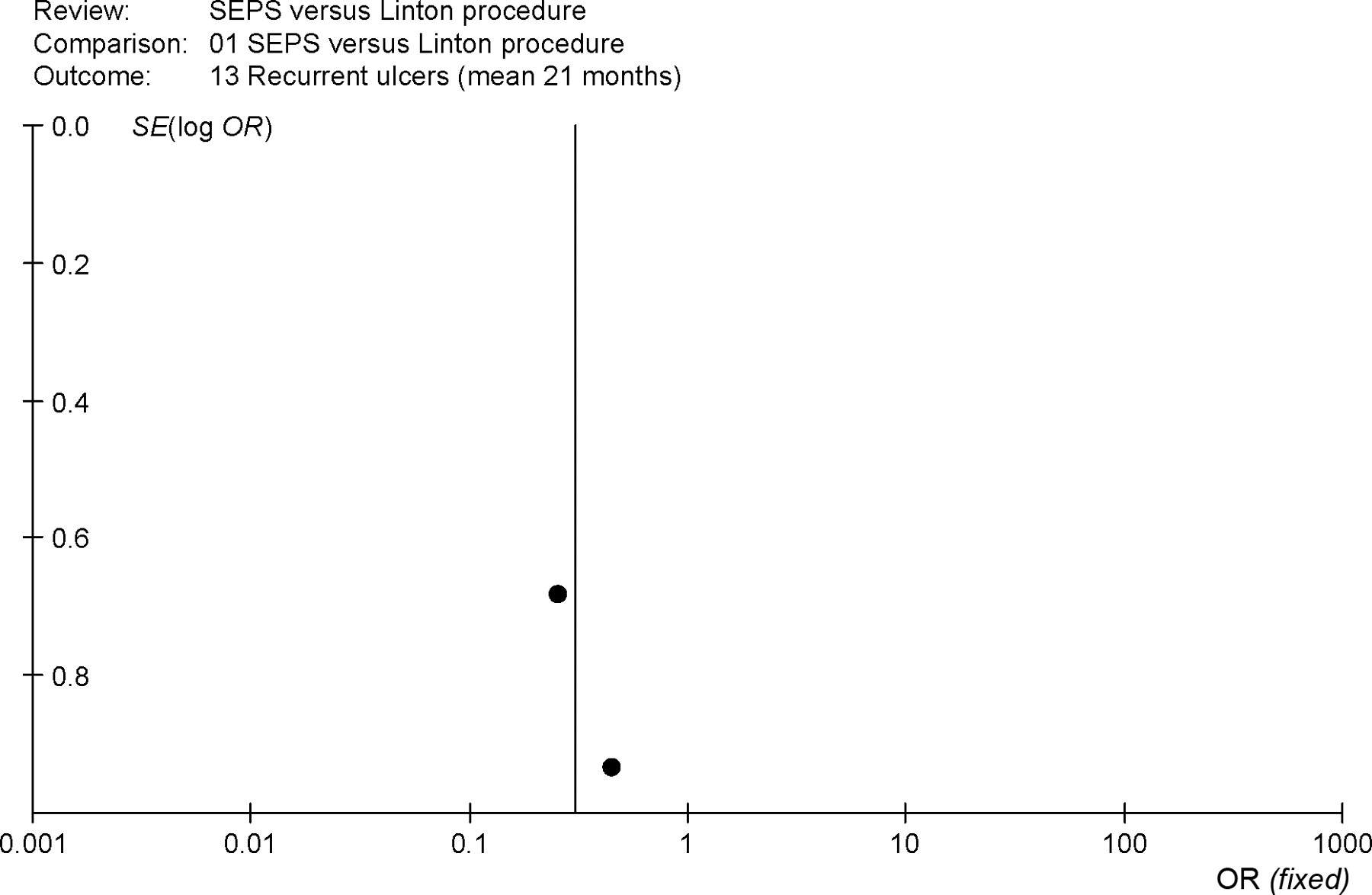
Assessment of publication bias using a funnel plot on the outcome ‘Recurrent ulcers (mean 21 months)’: the funnel plot shows marked asymmetry, but the pattern is not consistent with publication bias, all studies being equally distributed around the vertical axis
Sensitivity analysis
There was a significant heterogeneity in the data only for ‘hospital stay,’ which was available from two trials (test for heterogeneity [χ2 = 13.09, P = 0.0003]). For all the other outcomes measured in more than one study, no significant heterogeneity was found between the trials. However, this absence of heterogeneity between the trials may be caused by the comparatively low number of trials included in the meta-analysis. This in turn would mean that the test for heterogeneity was not powerful enough to determine whether significant heterogeneity was present or not. In addition, the studies yielded such a low volume of good quality data that sensitivity re-analysis was not carried out due to the difficulties of estimating ‘reasonable’ data.
Discussion
Venous ulceration due to IPVs can be cured with good results by surgical treatment. In the past, various surgical techniques have been abandoned in this field, mainly because of wound complications and because certain groups of patients failed to heal ulcers or developed recurrences, despite operation. 8,17–20 In addition to that, early reports of perforator ligation are particularly difficult to evaluate as they are invariably contaminated by synchronous saphenous ligation.
Stuart et al. 21 reported that most cases, where reflux was confined only to the superficial venous system ablation of superficial venous reflux alone, would result in haemodynamic improvement of synchronous ‘secondary’ deep venous reflux. However, IPVs were still observed in 72% of patients with residual deep venous reflux or in whom surgery had failed to resolve superficial venous reflux. In these cases, SEPS is believed to be the only reliable way to correct pathological outward flow in the perforating veins.
SEPS is a minimally invasive technique to interrupt calf perforators under direct vision using endoscopic instruments placed through small ports remote from the area of lipodermatosclerosis or active ulceration. Just as perforator ligation was falling into disrepute, enthusiasm was rekindled by the development of this technique and subsequent studies have shown promising results in terms of ulcer healing. 9,22–24 However, it is noteworthy that this procedure was recommended even though the early protagonists of SEPS seemed to have no clear view about the clinical circumstaces in which it was indicated. 25
TenBrook et al. 26 analysed the benefits and risks of SEPS in 1140 limbs with advanced CVI (two-thirds having synchronous superficial surgery) in a systematic review of 20 published studies. After SEPS, with or without superficial venous surgery, ulcers in 88% of limbs healed. The recurrence rate in 661 limbs was 13% at mean time of 21 months. Surgical complications included wound infection (6%), haematoma (9%), neuralgia (7%) and DVT (1%). The review cited four studies in which concomitant superficial surgery appeared to be associated with healing, but while combining the data from three of these studies showed a lower risk of non-healing, this did not reach statistical significance. Recently, Uncu 27 demonstrated the advantage of the combination of SEPS with superficial venous surgery, as well.
Similar findings to the systematic review by TenBrook et al. were noted in the reports by the New England Medical Center and the Mayo Clinic. 4,28 From the data of the NASEPS registry reported by Gloviczki et al., 9 an ulcer recurrence rate of 28% at two years, with a particularly poor outcome for secondary CVI (46% recurrence at two years), was noted. In patients with secondary CVI, there was valve destruction that would not be improved after superficial and perforating vein surgery. Deep vein surgery may be necessary in this situation.
In the setting of IPVs and superficial venous reflux, these initial studies and two more recent studies 29,30 suggest that SEPS combined with saphenous vein surgery is most advantageous. Furthermore, SEPS seems to be beneficial when IPVs are associated with deep venous reflux alone or when there is combined superficial and deep venous reflux.
In a RCT of several medical treatments of CVI combined with compression therapy, ulcers in 14–31% of patients healed by four weeks, 31 less than the 40% healing at 30 days shown for SEPS by TenBrook – even though the patient population in these surgical studies generally had severe venous disease and previous conservative therapies had failed. Risk factors for no healing and recurrent ulcers included new or recurrent IPVs, post-thrombotic syndrome, deep vein obstruction and ulcers larger than 2 cm in diameter. These risk factors increased the odds of the adverse outcomes by about four-four to 14-fold. However, there was a considerable uncertainty in the estimate, for wide CI were calculated.
The present meta-analysis only analysed the possible differences between the two techniques and not the cause of recurrent ulceration or non-healing. Regarding the postoperative complications between SEPS and the traditional Linton procedure, SEPS was associated with a significantly lower rate of wound infections owing to the avoidance of incisions over the already compromised skin.
In a prospective study by Pierik et al., 17 53% of patients who were treated with open perforator vein ligation had their postoperative course complicated by wound infections. Although some authors report wound complications in only 7–24% of patients 32–35 the findings of Pierik are in concordance with other reports of surgical treatment of patients with venous leg ulceration that mention wound complication rates of 44–58%. 36,37 Wound complications after endoscopic perforator vein ligation have been reported in 0–7.5% in retrospective studies. 38–41
Pieriks's study 17 showed no significant variation in blood loss between SEPS and the Linton procedure. As to this result, one has to consider that this study was published in 1997 and that SEPS was performed at that time with a mediastinoscope with channels for both the camera and working instruments. Improvements in instrumentations for this technique resulted in a reduced blood loss in SEPS. As to this, Uncu 27 also showed that SEPS performed with a balloon dissector is an effective and reliable method, and may result in a reduced blood loss in SEPS without tourniquet.
Although not evaluated in detail in the present meta-analysis, SEPS is associated with better cosmetic results compared with the Linton procedure. As originally described by Linton, the procedure involves a medial lower limb incision placed over the site of clinically significant insufficient perforator veins. Although the Linton procedure could eliminate the perforator reflux, it has been associated with longitudinal operation scarring and even skin breakdown at the incision site, resulting in less satisfactory cosmetic results compared with SEPS.
In the rate of DVT and death at six months, there was no difference between the groups. In the clinical parameters (healing and recurrence) SEPS was associated with a significant reduced rate of recurrent ulcers at a mean follow-up of 21 months. On the other hand, the ulcer healing rate at four months did not differ between the two procedures. In addition, the duration of the hospital stay was significantly shorter for SEPS than for the Linton procedure, whereas the rate of hospital re-admission showed no significant difference between both the groups.
In general, healing rates of >80% in both groups support the concept of meticulously eradicating reflux at all potential sites of deep-to-superficial reflux in the surgical treatment of venous ulceration of the lower leg. 42,43 A potential limitation of the endoscopic technique includes the inability to reach all IPVs. Especially in patients who have severe lipodermatosclerosis, the necessary expansion of the subfascial space can be laborious.
Limitations/heterogeneity of included studies
The different trials included in our meta-analysis partly varied in criteria for patient selection, clinical characteristics of their populations and the patients' risk profile (different proportion of patients with several key risk factors for adverse outcomes), in inclusion criteria, definitions of outcomes and reporting of outcomes, different operative and endoscopic techniques (whether all patients in the SEPS group underwent a systematic dissection of the intermuscular septum), in study design and protocols, follow-up periods, primary endpoints, in the execution of the trials and in a comprehensive definition of perforator incompetence based on their potential to cause venous haemodynamic dysfunction. In detail, the application of simultaneous saphenous vein ligation, which may improve the outcome in venous disease by itself, differed among the studies. In addition, the differences in the extent of perforator vesssel ligation, individual surgeon experience and the use of skin grafting may contribute to the variability in outcomes. Furthermore, individual studies generally did not report outcomes stratified by the use of concomitant procedures or by level of patient adherence concerning postoperative ambulant compression. Also, because some patients underwent bilateral surgery, some outcomes may have been affected by clustering of risk factors for both limbs.
Some of the studies presented preliminary data and outcomes that might have reflected a learning curve for the procedure and the material with which the procedure is performed has been greatly improved, resulting in a much better exposure of the subfascial space. Again, in the present meta-analysis, there was a considerable uncertainty in the estimate, for wide CIs were calculated.
Summary
Implications for practice
In terms of clinical practice, the present meta-analysis shows that there is little robust randomized trial data for a definite statement concerning the role of SEPS in the management of CVI. Its use should not be employed routinely and could only be justified in patients with persistent ulceration thought to be of venous origin, and in whom any superficial reflux has already been ablated and post-thrombotic changes excluded. However, from the level of evidence available by now, it seems that SEPS, used as a part of a treatment regimen for severe CVI, is characterized by uncomplicated wound healing and less wound complications, which presumably lead to the significant shorter hospital stay compared with the Linton procedure. In addition, compared with the conventional Linton technique, SEPS is associated with a significantly lower rate of recurrent ulcers, whilst at the same time equivalent ulcer healing rates. Hence, this minimally invasive procedure, in combination with ligation of the SFJ and continued compression therapy, can be performed safely with less early postoperative complications compared with the Linton procedure and is, therefore, superior to open surgical exploration of the subfascial space in patients with venous ulceration of the lower leg.
Implications for research
However, further large prospective randomized trials are required to define the long-term benefits of SEPS, and to differentiate the relative contributions of compression therapy and the effect of concomitant superficial venous surgery in the management of severe venous disease. These trials should exclude post-thrombotic legs, because these patients may not benefit even if both the saphenous and perforating veins are ligated.
Incompetent perforators are but one of the contributing factors to ambulatory venous hypertension, and in patients with post-thrombotic syndrome and deep vein occlusion they are likely to be important outflow channels that should be preserved to assure the collateral venous circulation. Introduction of less invasive techniques for perforator ablation, such as ultrasound-guided sclerotherapy or radiofrequency ablation, may diminish the role of SEPS in the future.