
Abstract
The aim of this overview is to discuss the role of thigh compression for the management of venous and lymphatic diseases. The most important indications for thigh compression are prevention and treatment of sequelae of superficial vein procedures (surgery or endovenous procedures), prevention and therapy of deep vein thrombosis (DVT), post-thrombotic syndrome and lymphoedema. The intended effects depend mainly on narrowing/occlusion of deep and superficial veins on which the body position and the applied pressure play a crucial role. While in the horizontal position thigh veins can be narrowed by the light pressure of a thromboprophylactic stocking, much higher pressure is needed to compress thigh veins effectively during standing and walking. This is shown by magnetic resonance imaging (MRI) performed in the supine and upright position. Using pads, rolls or specially designed devices, the local pressure under conventional compression garments or bandages over a treated vein can be increased considerably. In patients with deep valve incompetence, beneficial haemodynamic effects of strong thigh compression have been demonstrated, but clinical studies in this field are still lacking. Thigh compression reduces oedema in patients with DVT and lymphoedema.
Introduction
Thigh compression is a rather underused and underestimated treatment modality in modern phlebology. Actually, there are some arguments that may explain this disregard:
Compression bandages do not stay in place due to the conic shape of the thigh; The upper end of any compression device slips down and is unable to compress the saphenofemoral junction; Compression stockings exert too low pressure on the thigh to be effective; Leg ulcers and severe skin changes develop only on the lower leg and never on the thigh. Therefore we do not need to compress the thigh; Increased thigh compression contradicts the theoretical concept of graduated support.
In the following overview we will discuss indications, experimental and clinical effects of thigh compression and provide some practical hints.
Rationale for thigh compression (indications)
Thigh compression focuses mainly on narrowing the thigh veins in order to achieve the following goals:
Prevention and treatment of sequelae after venous surgery or endovenous treatment. The rationale is two-fold:
To reduce side-effects such as pain, inflammation, deep vein thrombosis (DVT), ecchymosis, haematoma. The clinical outcome can be optimized by keeping the treated veins or the interrupted tributaries free from clots. After sclerotherapy it has been postulated that a better outcome may be achieved if the clots in the venous lumen are maintained as small as possible, following the concept of the ‘empty vein technique’ by George Fegan;
1
To prevent the late sequelae of pigmentation and neovascularization. Some recent publications have described an association between revascularization of haematomas after surgery of varicose veins and an increased risk of recurrence.
2
Prevention and therapy of DVT. Increase of blood flow velocity by narrowing the veins is an important principle directed against the stasis component in Virchow's triad. This has practical implications in the field of primary and secondary prevention of DVT. 3,4
Reduction of venous reflux in patients with deep venous incompetence. Axial reflux in the deep veins penetrating down into the popliteal and lower leg veins play a deciding role in the development of leg ulcers. 5 It has been shown that firm leg compression is able to reduce deep venous reflux and will therefore remain the basic management in chronic venous insufficiency. 6 However, thigh compression may have additional value that should be considered in future studies.
Reduction of oedema in chronic oedema and lymphoedema. Thigh oedema is a frequent problem in proximal venous obstruction and in lymphoedema. Swelling of the thigh and not only of the lower leg also occurs in normal individuals after prolonged sitting. 7
Is thigh compression able to achieve these objectives?
Answers to this question may be given based on some experimental data and few clinical reports.
Narrowing of superficial veins
Venous narrowing is a central prerequisite for the haemodynamic efficacy of compression.
External compression is able to reduce venous diameter if the applied pressure exceeds the intravenous pressure. The intravenous pressure depends mainly on the body position. Venous pressure in the lower extremity is around 10–15 mmHg in the supine position with a very small pressure gradient between the leg and thigh veins. In the standing position, the intravenous pressure in the lower extremity depends on the distance between the measuring point and the right heart. In a person of 180 cm body height, the intravenous pressure is around 90 mmHg at foot level, 60 mmHg at knee- and 30 mmHg at groin level. 8
This means that a low external pressure is required to narrow the thigh veins in the lying position. In fact, thigh length thromboprophylactic stockings, exerting an external pressure on the lower leg of 15–20 mmHg, will produce a pressure of 5–10 mmHg on the surface of the thigh, which is high enough to reduce the diameter of superficial and deep veins in the lying position. This can be shown impressively by magnetic resonance imaging (MRI) (Figure 1).
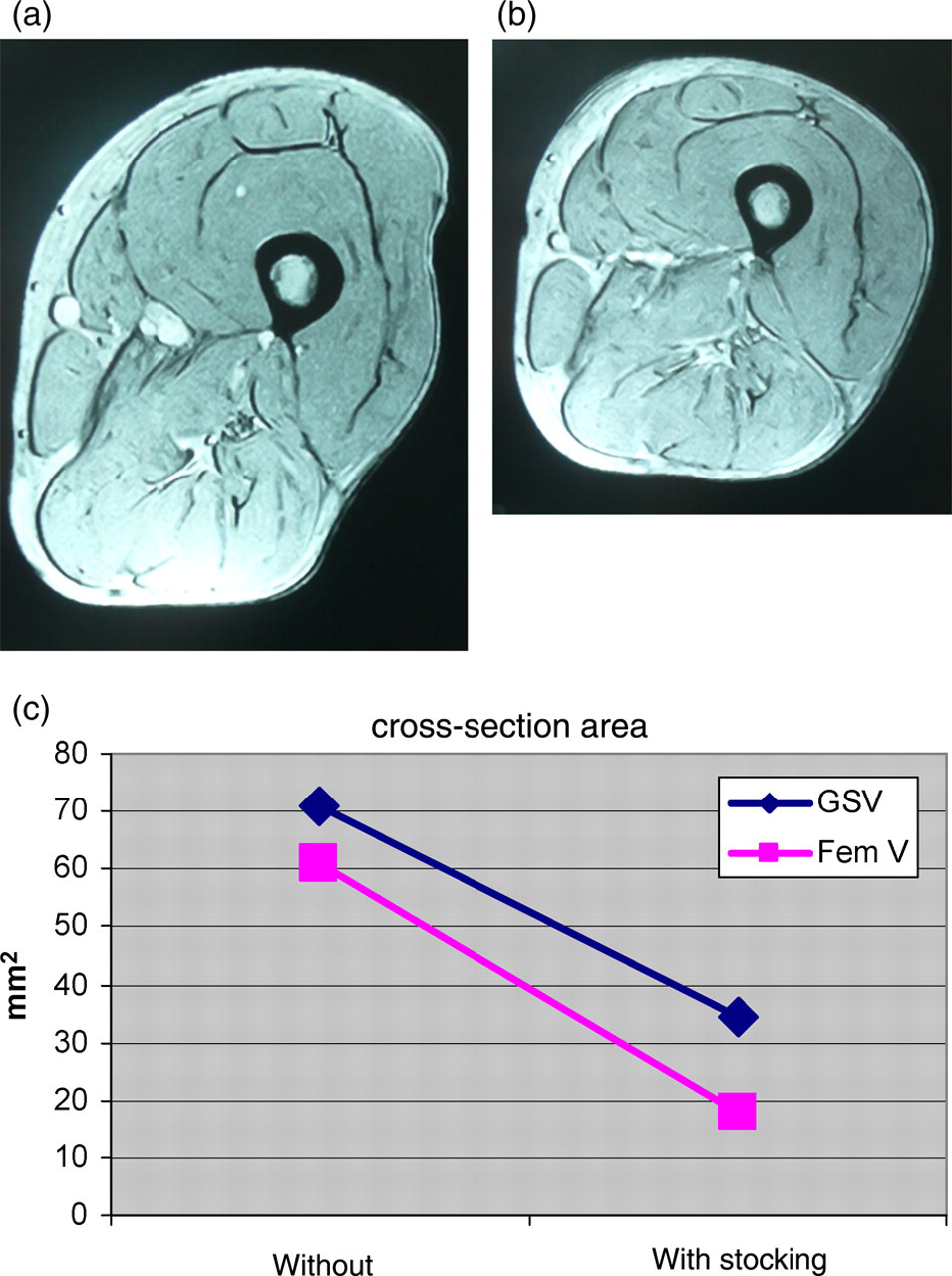
(a) Magnetic resonance image cross-section at mid-thigh level in a patient with massive varicose veins and a dilated great saphenous vein (GSV) in supine position. (b) A thromboprophylactic stocking exerting a pressure of 6 mmHg on the thigh leads to a reduction of the cross-section of the GSV and of the femoral vein. This low pressure is enough to make the contour of the thigh look more circular. (c) Planimetry shows a reduction of the cross-section area of both GSV and femoral vein with the stocking
Much higher pressures are needed to narrow the veins of the lower extremity in the standing position. 9 Venous diameters can be measured by Duplex ultrasound using special blood pressure cuffs containing a transparent acetate window (Echocuff®, VNUS, San Jose, CA, USA). A local pressure of more than 40 mmHg is necessary 10 to achieve a significant narrowing of superficial and deep thigh veins in the upright position. This pressure range can only be reached by strong thigh bandages and not by medical compression stockings.
As a practical consequence it has to be stressed that medical compression stockings after venous surgery or endovenous procedures are not able to achieve ‘an empty vein’ in the upright position. The beneficial effects of thigh length compression stockings after sclerotherapy of spiders 11 may, therefore, be explained by effects on the microcirculation of the skin rather than by venous narrowing.
Eccentric compression
In order to effectively collapse a superficial vein on the thigh after endovenous occlusion or a ruptured side branch after surgery, the local pressure can be increased using pads and rolls reduce the local curvature of the limb. The resulting ‘eccentric compression’ follows the law of Laplace which states that the pressure on a curved structure is indirectly proportional to the radius. Figure 2a shows an example of a newly developed wedge-shaped device consisting of a hard core surrounded by relatively soft plastic material 12 (Medi postop®, Medi Bayreuth, Germany). As can be demonstrated by special tilting MRI equipment, allowing investigations not only in the lying but also in the upright position (G-Scan® Esaote, Genoa, Italy), the great saphenous vein can be collapsed under the wedge, which is fixed by cross-wise applied tapes and a compression stocking on top (Struwa 35®, Medi Bayreuth, Germany) (Figure 2b). The pressure measured under the device at mid-thigh level was 66 mmHg.

(a) Wedge-shaped foam pad (medi Postop®) with firm core (black cylinder). (b) Magnetic resonance image cross-sectional view at mid-thigh in standing position where the wedge-shaped device (a) causes a deep impression on the medial aspect. The wedge is attached to the skin with tapes and a stocking (Struwa 35®) is put on top. The pressure measured under the device is 66 mmHg. It can be seen that the great saphenous vein is nearly totally compressed
Besides the dimension (radius) of the device, its consistency plays a crucial role for the pressure that is achieved under the pad. 13
Narrowing of deep veins
A reduction of deep vein diameter is a desirable effect of external compression especially for the prevention and therapy of DVT as well as for an improvement of venous haemodynamics in deep venous incompetence.
In the supine position, this can be achieved by very low pressure exerted by a thromboprophylactic stocking as demonstrated in Figure 1. The decrease of the cross-sectional area of deep veins will lead to an increase of venous blood flow velocity, which is the basic mechanism of action of such stockings. This could be shown by measuring the mean transit time of the venous flow in the lower extremity by injecting a radioactive tracer into a dorsal foot vein. Thigh length thromboprophylactic stockings were able to accelerate blood flow velocity significantly to the 1.5-fold in average. 14 The narrowing of deep veins by thromboprophylactic stockings in association with an increase in venous flow velocity favours the use of thigh-length models and does not support proposals postulating that knee length stockings would have the same haemodynamic effect. 15
However, it has to be stressed that such light stockings are effective in the supine position but, not when the patient is mobile and walking around. They are certainly also insufficient as a compression regimen after varicose vein surgery. 16
In the standing position much higher pressures are needed to narrow deep thigh veins. A pressure around 70 mmHg is necessary to nearly occlude the deep femoral vein, as demonstrated by phlebography with and without a tightly applied stiff bandage (Figure 3).

Ascending phlebography in the standing position. Left: without compression, right: with a short stretch adhesive bandage exerting a pressure of 60 mmHg at mid-thigh. Concentric thigh compression with high pressure narrows the femoral vein in standing position
Reduction of deep venous reflux
In contrast to the therapeutic target of occluding superficial veins after endovenous procedures or surgery, we do not intend to achieve sustained complete occlusion of deep veins by our compression treatment, which would cause a tourniquet effect enhancing distal congestion.
Two main mechanisms prevent such a tourniquet effect: the instant pressure loss of any short stretch bandage and the driving force of the blood pumped upwards towards the heart during movement.
Actually in everyday life, the phases of standing still are short and regularly interrupted by walking and moving. As shown in Figure 4, the sub-bandage pressure under a stiff bandage fluctuates between 40 mmHg and 60 mmHg during walking. These pressure fluctuations will cause an intermittent vein compression.
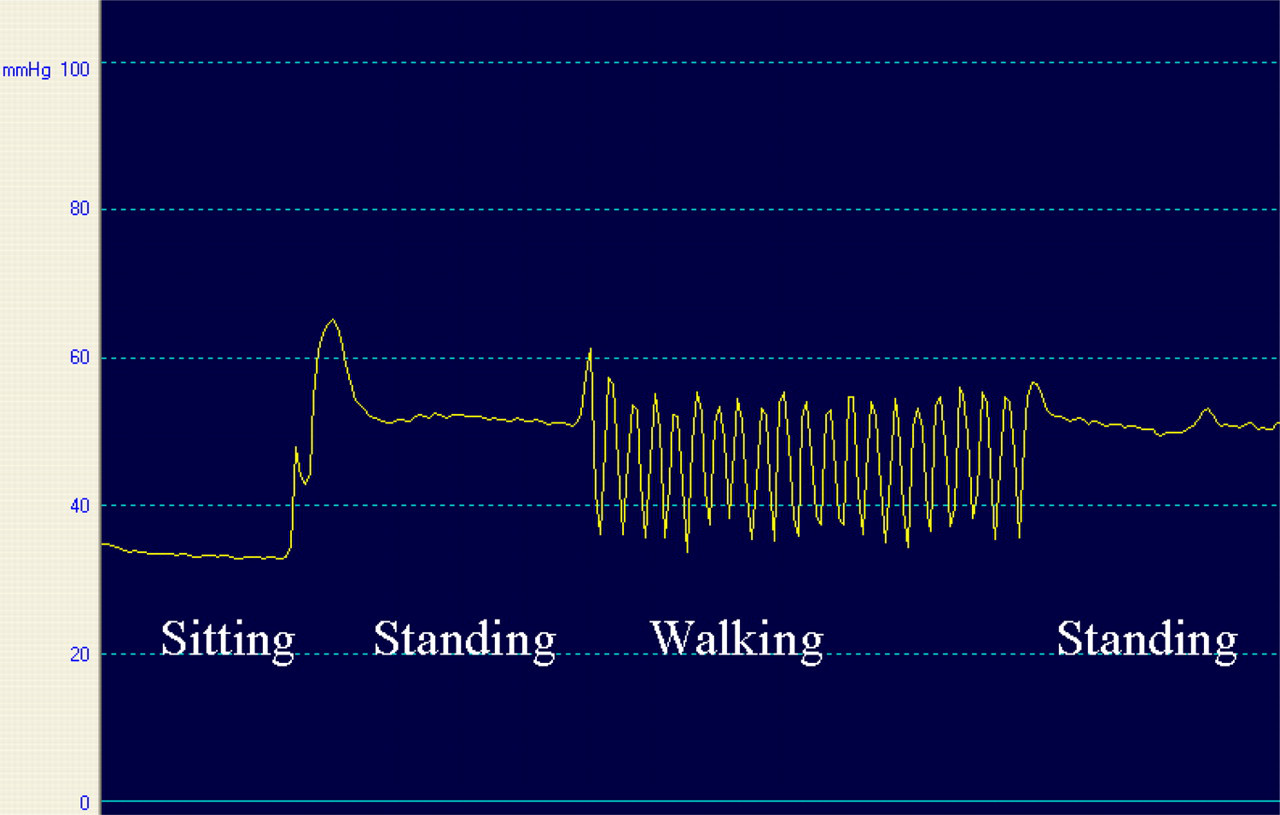
Sub-bandage pressure measured by a Picopress® transducer at the medial mid-thigh level after application of an adhesive bandage. The pressure peaks during walking go up to 55 mmHg
Several experiments have been performed in order to prove the haemodynamic effects of this intermittent compression. Blood pressure cuffs with a pressure of 60 mmHg were taken as a model for strong thigh compression using stiff material. Patients with congenital absence of venous valves, used as a very impressive model for severe deep (and superficial) reflux, were investigated by peripheral venous pressure measurement. This revealed high fluctuations, but no fall of intravenous pressure during walking (ambulatory venous hypertension). 17 By applying blood pressure cuffs with 60 mmHg on the thigh, no increase of peripheral pressure was observed in the standing position, proving that the exerted pressure did not totally occlude venous outflow. When patients started to walk on a treadmill, a reduction of ambulatory venous hypertension by reducing the systolic pressure peaks could be demonstrated (Figure 5). The same effect could be shown in patients with deep venous incompetence owing to a post-thrombotic syndrome. The most extensive reduction of venous reflux using air plethysmography was achieved by a thigh pressure of 60 mmHg. 10 These observations can be explained by an intermittent interruption of venous reflux by intermittent narrowing of the incompetent veins creating a kind of artificial valve mechanism. 17
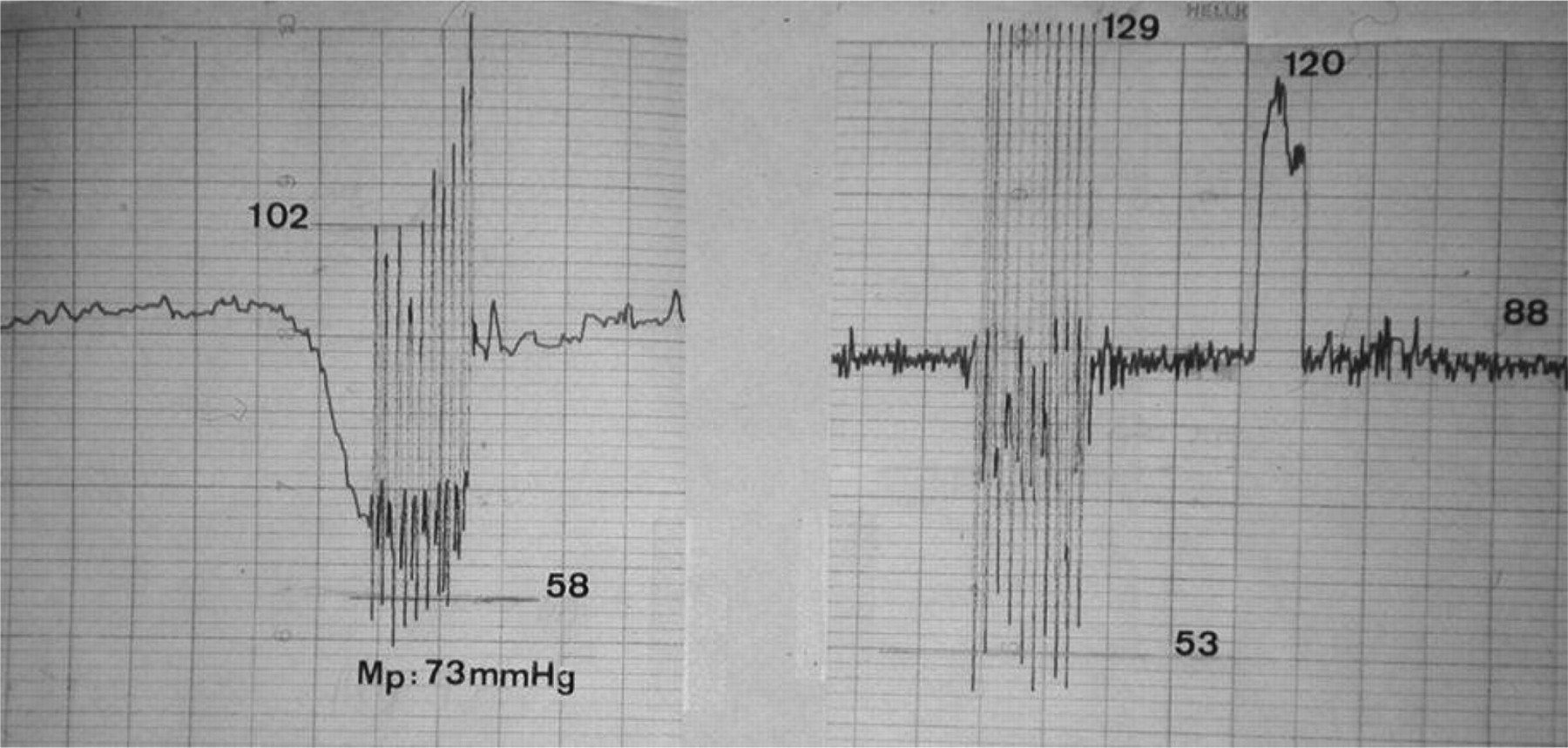
Pressure in a dorsal foot vein in a 16-year-old boy presenting venous leg ulcers owing to congentital absence of vein valves. The curves should be read from the right to the left side. Right: Standing pressure is 88 mmHg and increases instantly to 120 mmHg by a Valsalva manoeuvre. Walking on a treadmill causes the pressure to oscillate between 53 mmHg and 129 mmHg without a fall of pressure (ambulatory venous hypertension). Each systolic pressure peak represents a wave of massive venous reflux. Left: A blood pressure cuff on the thigh with a pressure of 70 mmHg cuts the pressure peaks during walking down to 102 mmHg due to short phases of intermittent interruption of venous reflux
Oedema reduction
Studies reporting a volume reduction after compression treatment have been published, especially for lymphoedema patients. They usually report on absolute and relative volume reduction of the whole extremity in comparison with the normal contralateral side, but do not specifically address volume changes of the thigh alone. 18 Thigh compression may shift oedema fluid into the non-compressed parts of the groin and the genitalia, and should therefore be combined with manual lymph drainage in the initial treatment phase.
Clinical efficacy of thigh compression
The importance of compression after active varicose vein therapy is still not well endorsed by evidence-based medicine data. 19 Studies are sparse, especially concerning thigh compression. In one trial measuring postsurgical bleeding using labelled red blood cells, less haematoma formation was found by application of adhesive thigh bandages after surgery. 20 Most other trials did not show advantages of bandages over stockings. 19 This raises the suspicion that the sub-bandage pressure applied in these studies was considerably lower than the pressure range needed to achieve venous narrowing in the upright position.
One important study clearly showed that high compression pressure on the thigh exerted by a special bandaging technique was able to reduce the pain after endovenous laser ablation with high statistical significance. 21 This finding is in strong agreement with our experience showing that patients after such procedures nearly never need analgesic drugs if they are put under a strong thigh compression bandage.
The thromboprophylactic effect of compression stockings is well established. 3 Based on our findings (Figure 1), we are convinced that there is still a place for thigh length stockings in the bed-ridden patient.
Concerning compression as an adjuvant treatment in patients with DVT data have been published who show advantages of bandages compared with stockings, both covering the thigh, concerning a reduction of pain and swelling. 22
The immediate pain-relieving effect of placing an eccentric compression pad topped by a strong compression bandage over a thrombophlebitic vein segment is based on experience, but has not been investigated by any randomized clinical trial.
Also studies dealing with compression therapy in lymphoedema do not give information regarding the specific effect on the thigh.
Practical tips for effective thigh compression
Thromboprophylactic stockings exerting a pressure of 15–18 mmHg in the ankle area are effective in the supine position of the bed-ridden patient, but not in the upright position.
Medical compression hosiery, even higher compression classes, is too weak to achieve adequate venous narrowing and compress-treated superficial vein segments in the thigh region. The local pressure can be considerably increased by applying pads, rolls or specially designed devices over the treated veins. It is advisable to mark the site of the treated vein exactly before the procedure and to attach such devices firmly to the skin by using tapes before a stocking is donned on top.
An alternative for sufficient pressure is to apply a thigh bandage with high pressure, starting proximal to the bandaged leg, including the knee and going up to the groin. This kind of bandage can also be used to treat patients with DVT and severe chronic oedema of the thigh due to proximal venous obstruction or lymphoedema.
In our daily routine, we prefer strongly applied adhesive bandages that will stay on the leg for seven to 10 days (Figure 6). Alternatives that are widely used, especially in lymphoedema patients, are short stretch bandages applied over foam-padding layers. Our bandages achieve a pressure at the mid-thigh level of 40 mmHg or more in the lying position, corresponding to a standing pressure of more than 70 mmHg when inelastic material is used (Figure 7). In the first few hours, this pressure will drop to a level of around 25 mmHg in the supine position, which is very well-tolerated, and about 50 mmHg during standing and walking, which is high enough to narrow the veins and thus cause a haemodynamically significant effect.

Thigh bandage using adhesive material (Panelast) applied with high pressure after venous surgery. The patient is mobilized immediately and the bandage is removed after 10 days, together with the sutures in the groin

Example for a bandage applied after classical varicose vein stripping in the operating theatre. After immediate mobilization, a fast pressure loss takes place after firm application of an adhesive bandage. The resting pressure during night time is less than 25 mmHg, which is well tolerated
The first circular tour starts on the proximal lower leg overlapping the leg bandage. The knee is bent in a 120° position and the tendons in the popliteal fossa are protected with cotton wool. Over the knee we use material that also has some stretch in the transversal direction (e.g. Panelast®, Lohmann & Rauscher, Neuwied, Germany; Tricoplast®, BSN, Hamburg, Germany). In order to cover the thigh up to the groin, a second bandage (2.5 m long) either with the same material or with a one-way stretchable bandage (Porelast®, Lohmann & Rauscher, Neuwied, Germany) will be needed in most cases. The uppermost border of the bandage can be fixed using a well-tolerated adhesive tape (Fixomull®, BSN, Hamburg, Germany).
In addition to the full leg compression, bandages intermittent pneumatic compression cuffs covering the thigh and even including the groin and the lower abdomen may be successfully used in lymphoedema patients as one component of complex lymphatic decongestion therapy.
In order to prevent post-thrombotic syndrome after proximal DVT, the use of thigh-length stockings is recommended as long proximal swelling is a problem. Two-part stockings can be considered from which the thigh sleeve is used in the first weeks after acute DVT only.
Footnotes
Acknowledgements
The authors thank Dr Steven Zimmet for encouraging us to write this overview and for providing assistance in editing the text.