
Abstract
Spontaneous and asymptomatic supraclavicular thoracic duct cysts occurring in the neck are the rarest. We report a case of a huge thoracic duct cyst occurring in the supraclavicular fossa with a review of the literature and management options. A 28-year-old female had a left supraclavicular mass with a 10-year history. A cervical thoracic duct cyst was diagnosed after chemical analysis of the milky fluid obtained by preoperative fine-needle aspiration. Treatment was achieved by surgical excision of the cyst and thoracic duct ligation. Pathological analysis of the cyst after excision confirmed the diagnosis. In the case of left supraclavicular masses, the rare differential diagnosis of thoracic duct cysts must be considered as a possibility. Magnetic resonance imaging as the imaging method of choice and chemical analysis of the milky fluid obtained by preoperative fine-needle aspiration are sufficient for primary diagnosis. The treatment of this disease consists of simple excision.
Introduction
Spontaneous supraclavicular thoracic duct cysts (lymphocele) are very rare. 1–3 The case of a 28-year-old female with a spontaneous thoracic duct cyst is presented along with a review of the literature, including diagnostic features and treatment options.
Case report
A 28-year-old female was referred to our hospital with a 10-year history of a left supraclavicular mass. The mass had steadily increased in size. The patient had no history of trauma or surgery in the region and there was no pain or pressure symptoms. Physical examination showed a non-tender, non-pulsatile, slightly compressible cystic lump in the left supraclavicular area. The chest X-ray was normal. A magnetic resonance imaging (MRI) showed a large cyst in the left supraclavicular fossa and it was multilocular measuring about 10 cm in diameter (Figure 1). Lymph vessel radionuclide imaging demonstrated the thoracic duct was adjacent to the lesion (Figure 2). The fine-needle aspiration yielded about 20 mL of milky coloured fluid. Chemical examination of the fluid revealed total protein of 60.3 g/L, glucose 10.1 mmol/L, triglycerides 28.53 mmol/L and cholesterol 0.04 mmol/L. Considering these clinical and laboratory findings, the initial clinical diagnosis was thoracic duct cyst.

T2-weighted magnetic resonance imaging of the multilocular thoracic duct cyst (arrow showed) (A) coronal plane and (B) axial plane

Radionuclide imaging showing the thoracic duct adjacent to the lesion (thin arrow, thoracic duct; thick arrow, the cyst)
Under general anaesthesia, a low semi-collar type incision was performed. At surgery, a well-encapsulated cyst was found beneath the sternocleidomastoid muscle and the omohyoid muscle, and there was a little adherence to the anatomical structures. The cyst was dissected on all sides and separated from the common carotid artery, internal jugular vein and vagus. The proximal portion of the thoracic duct with a narrowed lumen was in direct contact with the lateral surface of the cyst. The inferior portion of the thoracic duct descended from the bottom of the cyst into the mediastinum. Special care was taken to ligate the connected lymphatic vessels and the thoracic duct, and the cyst was removed from the surgical field. The histopathology of the cyst wall showed a single layer of endothelial cells and there was no evidence of malignancy (Figure 3).
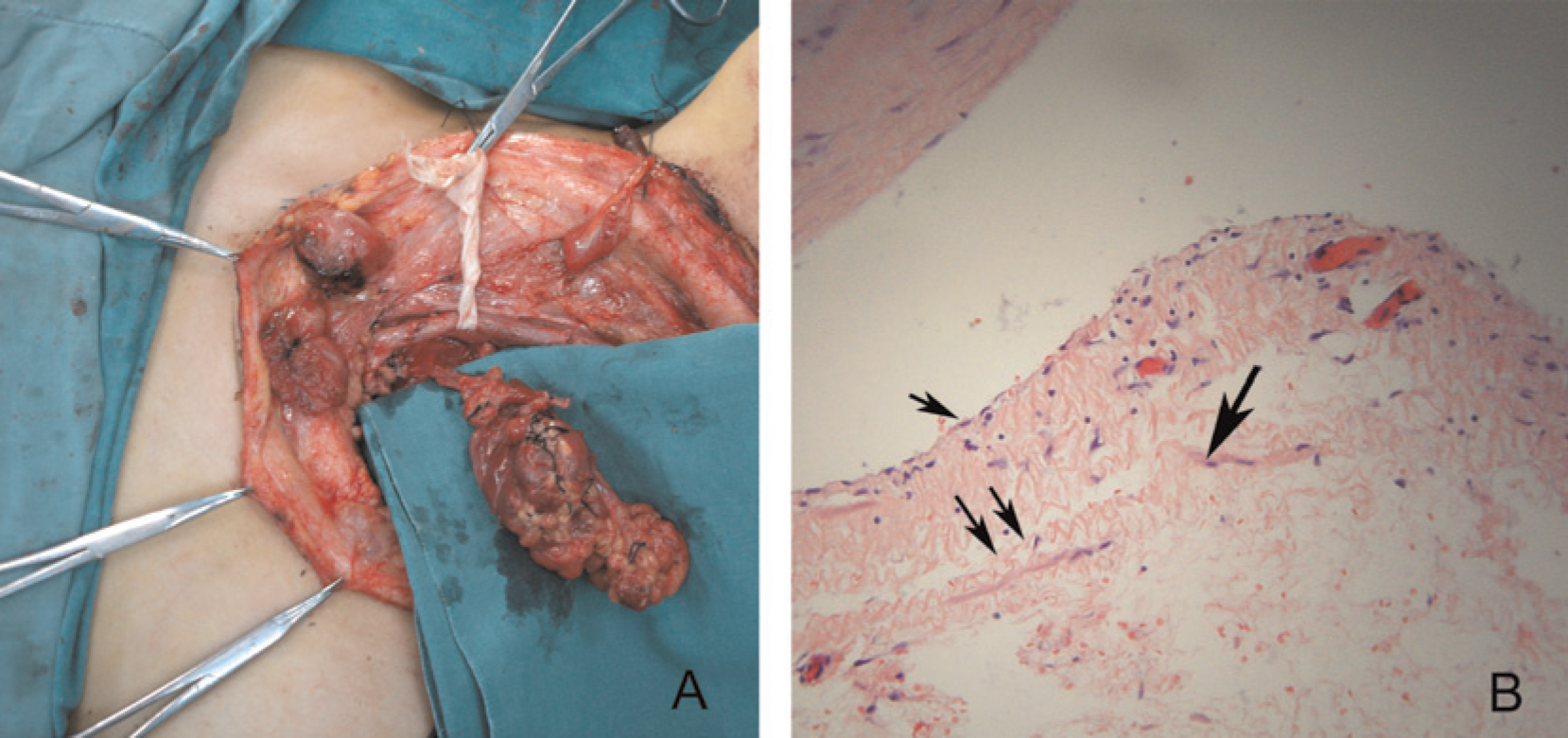
(A) The cyst and the thoracic duct in operation. (B) Photomicrograph of the thoracic duct cyst wall demonstrating a flattened epithelial cell layer (small arrow). There is a loose underlying stroma with lymphoid inclusions and an adventival fat layer (double arrows) with muscular layers (larger arrow)
The patient had an uneventful postoperative recovery with no dropsy in the left upper limb. Postoperative MRI did not reveal any residual or recurrent cyst formation. There has not been any further recurrence of the supraclavicular swelling over the last three years.
Discussion
Thoracic duct cysts are very unusual and are commonly found in the mediastinum and occurring in the neck are rarest. 1 The main symptoms observed are swelling or those resulting from compression of adjacent structures such as dysphagia and cough, the latter being more frequent in the case of a mediastinal mass. 2 The aetiology of thoracic duct cysts remains undetermined. There are three schools of thought with respect to thoracic duct cysts arising de novo. The first attributes it to a congenital weakness in the wall and the others consider these cysts to be either secondary to the degenerative process consisting of inflammatory or degenerative changes in the cyst wall. Other authors thought that obstruction of lymphatic drainage in the angle formed by the internal jugular vein and the subclavian vein was also one of the reasons. In this patient, the first seems to be the reason of this disease, as the histopathology of the cyst wall showed a thinner layer of endothelial cells.
Diagnosis can be done using chemical analysis of fine-needle aspiration of these lesions. 3,4 The cystic fluid is milky and usually contains an excess of triglycerides and protein. MRI, especially a T2-weighted image is superior in delineating the anatomical boundaries and retrosternal extension. 1 This allows for the planning of therapy. For screening purposes, a thorax X-ray is advisable in order to exclude an expanded mediastinum. 1 Lymphangiography or lymph vessel radionuclide imaging may aid preoperative diagnosis and confirm communication with the thoracic duct. 5
Where treatment becomes necessary by virtue of its size or symptoms, a variety of approaches have been described ranging from fine-needle aspiration with sclerosants to surgical exploration and removal. If an MRI shows that the cyst is multilocular, sclerotherapy should be performed under digital subtraction angiography (DSA) guidance. For surgical removal, care should be taken to ligate the thoracic duct to avoid the serious surgical complication of chylothorax or cervical chylous fistula. As the existence of multiple collateral circulation of lymphatic vessels, the ligation of the thoracic duct in the neck would not result in lymphatic dropsy in the left upper limb. Other surgical complications reported in the literature are wound-healing problems, inflammations, and scars and loss of sensation in the surrounding skin. The injury of the vagus nerve, the brachial plexus and the phrenic nerve during surgery could be avoided as long as there is a thorough knowledge of the normal anatomy of the neck. In our patient, there were no complications except the temporary loss of sensation in the surrounding skin which restored five months later. After three years of follow-up, there has been no sign of recurrence in the patient.
On the whole, in the case of left supraclavicular masses, the rare differential diagnosis of a thoracic duct cyst must be considered a possibility. Fine-needle aspiration as well as MRI is sufficient for the primary diagnosis. The treatment of this pathology consists of simple excision.
Footnotes
Acknowledgement
This work was supported by grants from the Shanghai Science and Technology Committee (Grant No. Y0203).