
Abstract
Objectives
Compression sclerotherapy has been satisfactorily used for half a century for the treatment of varicose veins of the lower extremities. The effect of sclerosing solutions is that of making endofibrosis and vascular damage via producing endothelial injury. Different sclerosing agents were used by applying many different sclerotherapy methods. In recent years, sclerosing foam has been introduced in sclerotherapy with the goal of increasing the efficacy in the treatment of varicose veins. It is still uncertain whether foam or liquid form is superior. The aim of this study is to determine the efficacy and safety of the sclerosant polidocanol – which is a well-known detergent-type sclerosing agent – in foam form compared with liquid form.
Methods
A total of 100 women patients with telengiectases and small varicose veins of less than 4 mm were included in this study. The patients were divided into two groups according to presenting dates. Fifty patients who presented first were classified as the first group. They were treated with Tessari's foam sclerotherapy method. The second fifty patients who presented later were placed in the second group. They were treated with the liquid form of polidocanol. Extremity veins that did not have insufficiency at the saphenofemoral junction were divided into three groups as <1 mm, 1–2 mm and >2 but <4 mm, and the veins were treated with 0.25%, 0.5% or 1% of polidocanol, respectively. Clinical improvement, patients' complaints and side-effects were determined after treatment.
Results
Complete disappearance was determined in 84% of patients in the foam form group and in 72% in the liquid form group. Although polidocanol in foam form's success rate was higher than the liquid form of polidocanol to clear the vessels, this result did not reach statistical significance (P = 0.148). There was no significant difference also in the side effects between each group.
Conclusion
Compression sclerotherapy is an effective and useful method for treating small varicose veins and telengiectases. Both polidocanol foam and polidocanol liquid forms are effective and safe sclerosing agents. The rates of side-effects were similar for both sclerotherapy methods. Although efficacy to clear the small varicose veins and telengiectases with foam polidocanol seems to be more successful than with liquid polidocanol, it is early to declare the superiority of the foam sclerotherapy method.
Introduction
Varicose veins disturb patients by their bad appearance, in addition to causing leg complaints such as leg fatigue, heaviness, pain or restlessness, and significant complications such as thrombosis, pulmonary emboli or venous ulcerations. Even patients who do not have any large varicose veins, but only spider or reticular veins may experience severe varices-related symptoms. The goal of treatment of varicose veins is to achieve perfect outcome both physiologically and cosmetically, with sclerotherapy being one of the most popular current treatment methods. Sclerotherapy is an effective and minimally invasive procedure in the treatment of varicose veins of the lower extremities, which can be performed on an outpatient basis. The first use of sclerosing agents in the treatment of varicose veins dates back to earlier than 150 years. Due to the high incidence of complications such as sepsis and emboli in that period, widespread use of sclerotherapy became available only after the 1940s. While sclerotherapy has been used as an alternative for surgical treatment of saphenous vein insufficiency and large varicose veins, it is widely applied in small veins as well. Sclerosing agents produce endofibrosis and vascular obliteration via producing thrombus development and endothelial damage. 1,2 The sclerosing solution to be employed should be safe and effective, without producing any discomfort and with few side-effects. Several different sclerosing agents and various sclerotherapy techniques have been utilized until today. Sigg 3 combined sclerotherapy and compression therapy and started to perform this method in distal veins. Later on, Fegan 4 applied compression sclerotherapy in perforating veins. It has been observed that the application of postsclerosis compression following sclerotherapy increases the effectiveness of the technique.
For years, detergent-type liquid solutions have been widely used in sclerotherapy. In 1944 Orbach 5 reported that foam, which he had manufactured by the air-block technique using polidocanol and sodium tetradecyl sulphate, could be more effective compared with conventional liquid forms that had been adopted in the past. However, foam sclerotherapy only became popular after 1997, following the introduction of Monfreux's method, consisting of air and using a glass syringe, and Cabrera's method, which substituted CO2 instead of air. 6,7 Advances in foam sclerotherapy have since continued, and in 1999, Lorenzo Tessari began practising a novel technique using two disposable syringes and a three-way stopcock. This technique has certain advantages such as simple preparation and instant application. 8,9
Polidocanol (hydroxypolyethoxydodecane), one of the detergent solutions, has been developed as an anaesthetic substance in the 1950s and was used as a sclerosing agent in the treatment of spider veins 10 years later. 10 This sclerosing agent, which induces less pain and toxic reaction compared with other agents, can be used in the liquid form or as foam. It is still uncertain whether foam or the liquid form is superior. The aim of this study is to compare the efficacy and safety of the liquid and foam polidocanol forms as a sclerosing agent in the treatment of reticular and spider veins.
Patients and methods
A total of 100 patients treated with sclerotherapy for telengiectasia, venulectasia and/or reticular veins of smaller than 4 mm of the lower extremities were included in this study. Patients who had varicose veins larger than 4 mm were excluded. Patients were divided into two groups according to their dates of admission. The first 50 consecutive patients who were admitted constituted the first group, and the remaining 50 consecutive patients constituted the second group. Patients of the first group were treated with foam sclerotherapy and patients of the second group were treated with liquid sclerotherapy. Patients who had undergone foam and liquid sclerotherapy procedures together were excluded. Patients who had venous insufficiency in the saphenous veins, saphenofemoral or saphenopopliteal junction, as detected by Doppler-duplex examination, and those who had post-thrombotic varicose veins were also excluded. None of the patients had a history of using anticoagulant therapy, severe allergy or asthma. Sclerotherapy was not performed in pregnant or breast-feeding women. All patients in both groups were treated by the same physician. Telangiectasias of less than 1 mm were treated by using 0.25% polidocanol, venulectasias of sizes between 1 and 2 mm were treated by 0.5% polidocanol, and reticular veins larger than 2 mm but smaller than 4 mm were treated by 0.5% and 1% polidocanol. Needle sizes of 26 and 30 gauge were used. Sclerotherapy was performed from the large veins to the small ones; first the reticular veins, then the venulectasias and finally the spider veins. The first group of patients was treated with foam sclerotherapy using the Tessari method. For all concentrations of liquid polidocanol, 0.5 mL of the solution was mixed with air at a 1:4 ratio using a three-way stopcock. Thus, 2.5 mL of foam contained 0.5 mL of polidocanol. Liquid sclerotherapy was applied to the second group by the air-bolus technique. Cotton pads were placed and stabilized by hypoallergic tape following the injections in both groups and elastic compression bandages were applied. Patients were recommended to walk immediately after the completion of sclerotherapy and application of the bandages. Bandages and pads were removed after two days. Then, all patients were required to wear class I (20–30 mmHg) compression stockings for eight days.
One to seven sessions of sclerotherapy were performed on each patient. The mean number of sclerotherapy sessions was 2.5 in the first group and 2.7 in the second. All patients were evaluated 15 days after the last therapy session in terms of disappearance of the vessels and improvement of visual appearance. The results were categorized in five groups as worse than before treatment, no change, minor disappearance, moderate disappearance and complete disappearance. Treatment-related adverse events were noted in both groups. Success and complication-related results were statistically analysed. The chi-squared test was used to compare the results and adverse events of two treatment modalities. A P value <0.05 was considered significant.
Results
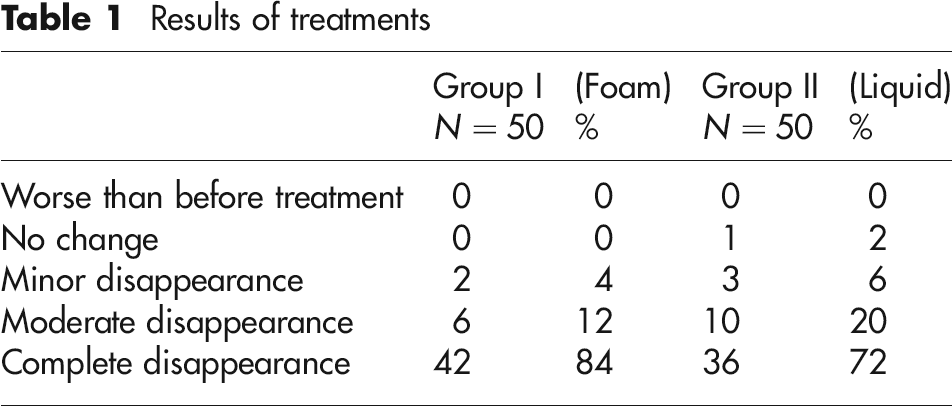
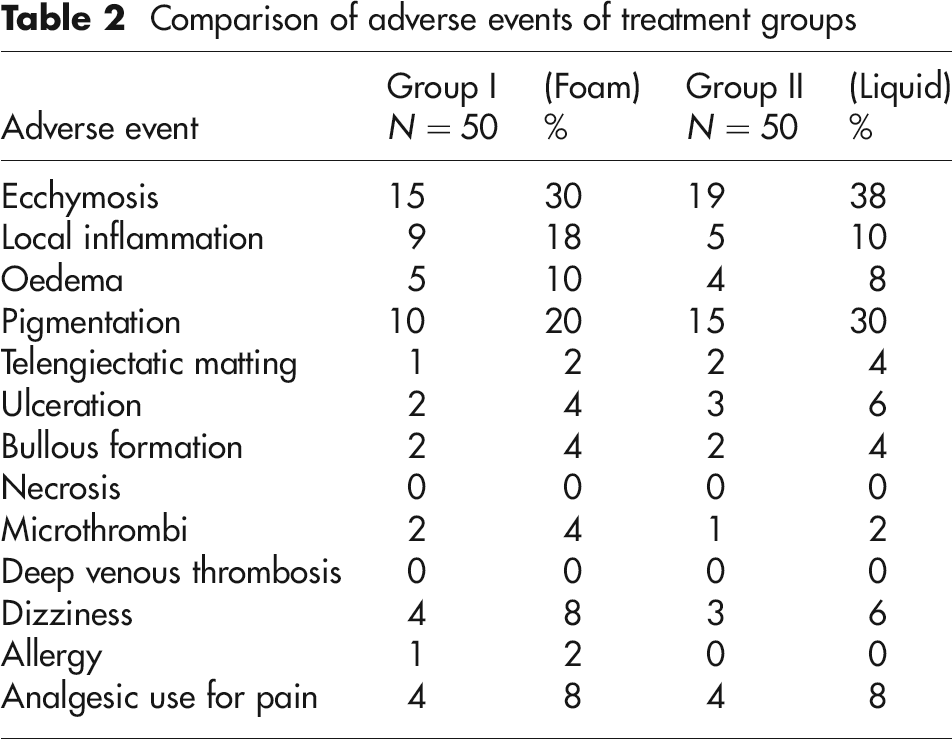
The first group treated by foam sclerotherapy consisted of 48 women (96%) and two men (4%), with a mean age of 36 years. The second group consisted of 49 women (98%) and one man (2%), with a mean age of 38 years. Both groups appeared to be successful in terms of resolution of bad appearance (Table 1). Complete disappearance was determined in 84% of patients in the foam form group and in 72% in the liquid form group. Although complete disappearance seemed to be more prominent in the foam sclerotherapy group, this difference was not statistically significant (P = 0.148 with the chi-squared test). The results of treatments are shown in Figure 1. The sums of complete disappearance and moderate disappearance rates were close, being 96% in the first group and 92% in the second. Adverse events seen in both groups are presented in Table 2. There was no significant difference in all adverse events between each group (P > 0.05). Adverse events, except for ecchymosis, local inflammation and pigmentation, were very rare. Ecchymosis was the most frequent adverse event and was observed in 30% of the first group and 38% of the second. The other transient dermatological adverse events that were observed included local inflammation in 18% and 10% of the first and second groups, respectively, pigmentation in 20% and 30% of the first and second groups, respectively, and ulceration in 4% and 6% of the first and second groups, respectively. Bullous lesion was evident in 4% of both groups. Microthrombus was present in 4% of the first group and 2% of the second. No deep venous thrombosis was observed. While the rate of dizziness during the procedure was 8% in the foam sclerotherapy group and 6% in the liquid sclerotherapy group, visual disturbance was not seen in the two groups. Analgesics were needed after the procedure in 8% of the patients in both groups due to pain. Allergic reaction was seen in only one patient of the first group and there were no anaphylactic reactions in both groups.
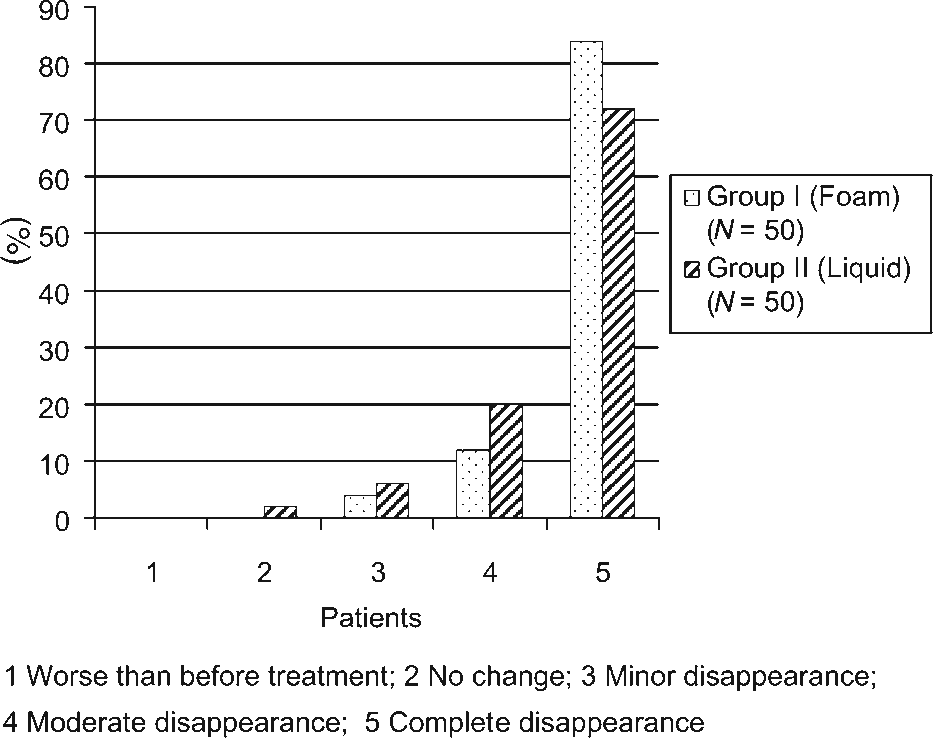
Results of treatments
Results of treatments
Comparison of adverse events of treatment groups
Discussion
Sclerotherapy is a safe and cost-effective method used in the treatment of lower extremity varicose veins. It is performed on an outpatient basis. The goal of sclerotherapy is to achieve maximal therapeutic effect with minimal patient discomfort and minimal side-effects. In addition to being an alternative to surgical treatment in the management of superficial venous insufficiency and large varicose veins, it is also very effective in the treatment of small veins of the lower extremities such as reticular veins or spider veins. It was shown in a prospective multicentre study of 12,173 sclerotherapy sessions that sclerotherapy was a very safe procedure for the treatment of telangiectasias, reticular veins, and saphenous and non-saphenous varicose veins. 11 Although most patients admit cosmetic concerns due to these small veins, varices-related symptoms also exist in almost all of them. 12 Besides achieving vessel clearance by sclerotherapy, improvement in other symptoms may also be obtained. The principle of treatment is to induce vascular endothelial damage and chemical phlebitis, followed by spontaneous thrombus and vein sclerosis. Detergent effective sclerosing agents used for this purpose include polidocanol, sodium tetradecyl sulphate, ethanolamine oleate and morrhuate sodium, hyperosmotic agents include hypertonic saline or dextrose, and chemical irritans include iodine and chromated glycerin. The detergent effect of polidocanol, which is one of the two most widely used sclerosing agents, is lower compared with sodium tetradecyl sulphate. However, it also has fewer side-effects such as toxicity, necrosis, pain and pigmentation. Compared with large veins, excellent results can be obtained in telangiectasias and small veins. In two large studies of compression sclerotherapy using liquid sclerosing agents, good to excellent results have been reported in more than 90% of the extremities. 13,14 In another study of liquid sclerotherapy, 12% had fair improvement while excellent cosmetic improvement was declared in 85%. 15
In liquid sclerotherapy, the sclerosing solution is unavoidably mixed with blood, thus reducing its sclerosing effect due to dilution. Sclerosing foam became popular due to its different behaviour from liquid solution by using the Monfreux method after 1997. Instead of being diluted in the blood as in liquid sclerosing agents, foam sclerosing agents replace the blood that is present in the vessel, get in full contact with endothelium and stick better to the vessel wall. Moreover, they also penetrate collaterals and induce their effects in a larger area of distribution in the extremity, and also reduce the venous diameter by 80% by inducing significant venous spasm. The same effect can be obtained by smaller amounts of foam sclerosing agent compared with liquid solution. 9,16,17 If large bubbles are present in the foam, its effect will be diminished as it will contain less amounts of sclerosing substance. For this reason, foams with little bubbles which are more effective, are preferred. 16 High rates of matting and microthrombus formation as side-effects have later been encountered by the Monfreux method as well. The side-effects of foam sclerotherapy were decreased by using the higher consistency and small bubble size foam solution of Tessari. 8 In the light of this information, studies comparing foam sclerotherapy with liquid sclerotherapy were performed. In one study, two methods were compared in greater saphenous vein sclerotherapy, and significantly more favourable results were obtained by foam sclerotherapy at three weeks (84% versus 40%). This was explained by the increased time of contact with the vessel wall in foam sclerotherapy. 18 In another comparative study, where both foam sclerotherapy and liquid sclerotherapy were performed in small veins of the same patients, a better outcome was reported with foam sclerotherapy as 94% versus 53%, but also with more complications. 9 Contrary to these results, no significant difference was found in terms of disappearance of reticular veins and telangiectasias in another study comparing these two techniques. 19 Another comparative study showed that both foamed and liquid polidocanol were safe and effective in the treatment of varicose and telangiectatic leg veins with improvement rates of 75% and 85%, respectively. 20 Complete disappearance rates in our study were in favour of foam sclerotherapy with 84% versus 72% in liquid sclerotherapy. If moderate disappearances were included in the analysis, similar success rates were found in both groups in our study. Owing to the significance of cosmetics, complete disappearance is clearly very important and foam sclerotherapy appears to be more successful in vessel clearance.
The success of any given method depends on both its effectiveness and its safety regarding complications and side-effects. Probably, as high concentrations of sclerosing agent were not administered to large veins, we did not see any incident of deep vein thrombosis. Although it has previously been suggested that foam sclerotherapy has higher rates of dizziness and visual disturbance, because of little amounts of air transfer into circulation, we have not noted such symptoms. 19 Higher rates of local inflammation, microthrombus formation, telangiectatic matting and pigmentation have been proposed as the most negative aspects of foam sclerotherapy compared with liquid sclerotherapy. In foam sclerotherapy, as a result of its greater contact with the vessel wall for a longer duration, the bubble affects perivenous tissue and therefore induces intense local inflammation. Similarly, local inflammation was observed in 18% of the first group versus 10% of the second group in our study. Alos 9 has also reported significantly more local inflammation in the foam sclerotherapy group. Compression application following sclerotherapy has been suggested to reduce local inflammation, microthrombus formation and pigmentation, in addition to enhancing the effect of the sclerosing agent via preventing the resolution of venous spasm. Postsclerotherapy hyperpigmentation occurs due to perivenous deposition of haemoglobin as haemosiderin pigment in the skin. There is more pigmentation with higher concentrations of sclerosing solution. In the early period, pigmentation rates were high in both groups of our study. In fact, rates of pigmentation as high as 10–30% have been reported in the early period in all previous studies; however, it has also been noted that 80–95% of these pigmentations have disappeared in 6–24 months. 2,12,21,22 While angiogenesis is held responsible, the exact cause of telangiectasic matting is unknown. High concentration, quantity and high pressure adopted during therapy, rather than the type of sclerosing solution, may be influential in the formation of matting. In general, telengiectatic matting is observed in over 10%. 15,23 Matting rates were similar in both groups in our study, both being below this value. There were no significant differences between foam sclerotherapy and liquid sclerotherapy in terms of pain induction requiring analgesics and other minor complications.
Conclusion
According to our results, very successful outcomes have been achieved by both foam sclerotherapy and liquid sclerotherapy, with low rates of complications and high rates of the efficacy of disappearance of lower extremity telangiectasia, venulectasia and reticular veins. Foam sclerotherapy seems to be more successful than liquid sclerotherapy in producing complete disappearance. Side-effects were observed in similar frequencies in both groups. It is too early to suggest that foam sclerotherapy, a safe and effective technique with high rates of success and low rates of complications, is the best method or is superior to liquid sclerotherapy in the clearance of small veins of the lower extremity. Further prospective studies, including larger patient groups and long-term results, are needed in order to reach definitive conclusions.
This study was presented as an oral presentation in the European Venous Forum in Barcelona in 2008.