
Abstract
Objectives
Foam sclerotherapy of varicose veins has recently proven to be an effective, economic and safe treatment modality. The present study attempts to evaluate the haemodynamic changes after sclerotherapy in addition to the clinical results.
Methods
In a prospective observation trial, 67 sites (2/3 of which were recurrent varicose [RV] veins after previous treatment) in 53 patients were treated with polidocanol foam, and the results were assessed clinically, by duplex, photoplethysmography and strain gauge plethysmography.
Results
With the exception of two sites (3.0%), all treatments resulted at least in an improvement, and about 80% of the treated veins were completely occluded as demonstrated by duplex ultrasound examination. The haemodynamical results accordingly reflected a significant improvement of the venous function. Patients with post-thrombotic syndrome showed poorer results.
Conclusion
Foam sclerotherapy is a highly effective and safe method for the treatment of primary and RV veins.
Introduction
Varicose veins are not life threatening but must not be underestimated in terms of disease burden. The number of patients seeking treatment is substantial. Subject to treatment is the entire range of conditions in clinical, aetiological, anatomical and pathological elements (CEAP) clinical stage 2 or higher. The primary goals are as follows:
To permanently interrupt the reflux of blood from the deep into the dilated superficial venous system; To reduce the venous blood volume in the affected limb; To avoid the formation of hydrostatic venous oedema and skin changes; To improve venous haemodynamics; To improve symptoms associated to chronic venous insufficiency (CVI).
There is no definite cure for the disease itself as it is probably a consequence of a structural disorganization of the venous wall whose underlying cause is elusive so far. Current strategies of the symptomatic therapy include conservative measures, sclerotherapy, endovenous procedures and surgical interventions. There is no inevitable link between certain treatment modalities and disease stages, respectively. The traditional mainstay of sclerotherapy, however, has been the treatment of tributary varices (TV), where it has been considered the treatment of choice for a while.
1
However, sclerotherapy of perforating veins (PVs) or the ablation of great saphenous vein (GSV) or small saphenous vein (SSV) with liquid agents was not sufficiently effective. Therefore, the introduction of polidocanol foam for sclerotherapy by Cabrera et al.
2
substantially broadened the spectrum of sclerotherapy. After the positive results of large clinical trials, the method was established for the ultrasound-guided sclerotherapy of saphenous veins (SV).
3–7
For the sake of permanent success, the treatment goal of sclerotherapy is not the induction of thrombosis but a permanent replacement of the vessel by a fibrous cord that cannot be recanalized and is equivalent to the result of a surgical removal of the varicose vein. When indications and contraindications are considered and technical as well as training requirements are met, sclerotherapy is an effective, economical and safe treatment modality. 7
The aim of this study was to study clinical, duplex and functional results after foam sclerotherapy.
Patients and methods
The present study is a prospective observation trial including 53 consecutive patients (6 men and 47 women) aged 60.0 ± 13.8 years on average. They underwent initial foam sclerotherapy of leg veins between October 2004 and May 2007. Indications for treatment were mainly TV or SSV varices and recurrent varicose (RV) veins after previous treatment (Figure 1); GSV sclerotherapy was performed only when patients did not agree on surgery or contraindications were present. A total of 67 sites were treated, 62.7% of which had been treated previously by surgery.

Reasons for treatment
The disease was classified according to CEAP and the stages were complemented with ‘A’ for asymptomatic and ‘S’ for symptomatic, respectively. 8
Sclerotherapy was performed under ultrasound control with a polidocanol solution (Aethoxysclerol®, Kreussler, Wiesbaden, Germany) that was foamed in a 1:4 ratio with air according to Tessari et al. 9 In this technique, two syringes are connected to a three-way stopcock, one of which contains one volume part of the sclerosing agent and the other four volume parts of air. The maximum concentration applied in the present study was 3%, and the patients received 1–4 injections at up to 5 mL per session; the average amount applied is shown in Table 1.
Details of sclerotherapy (mean ± standard deviation)
GSV, great saphenous vein; SSV, small saphenous vein; PV, perforating vein; TV, tributary varice
Treatment modalities, clinical course and the results of duplex evaluation, photoplethysmography and strain gauge plethysmography were prospectively recorded and stored by the investigator. The last follow-up examination was performed 128 days (mean) after the last treatment, and the result was assessed according to the recommendations of the second Tegernsee consensus conference on foam sclerotherapy as ‘full success’ (complete fibrosis, no flow detectable by duplex sonography, clinical improvement), ‘partial success’ (incomplete occlusion, clinical improvement) or ‘no success’ (no occlusion, no clinical improvement). 6
Duplex was performed before treatment and during follow-up in the standing position. Reflux was defined as retrograde flow >0.5 second. Occlusion was defined as complete incompressibility of the vein. Within one week after the treatment, the deep venous system was checked for deep venous thrombosis.
Photoplethysmography was performed with the patient in the sitting position. Venous refilling time (t 0) was measured after eight dorsiflexions of the foot.
Strain gauge plethysmography was performed with the patient in supine position and 45° elevated legs. Venous capacity (VC) and venous outflow (VO) were measured with a strain gauge at the largest calf circumference after venous occlusion at thigh level for 3 minutes with 80 mmHg.
Data were statistically evaluated with the Wilcoxon test for pair differences, the level of significance being P < 0.05.
Results
The majority of sites (n = 42, 62.7%) had been treated previously by surgery, flush ligation and stripping of the GSV being the most frequent modality (n = 27, 40.3%). The earlier treatment had been performed between 0 and 33 years (mean 11.5 ± 10.0 years) before.
According to the CEAP classification, the majority of cases was in stage C2 (41.8%), followed by C3 and C4 (25.4%, respectively); stage C6 was found only in five cases (7.5%). The aetiology was primary (Ep) in all cases and secondary (post-thrombotic) in five cases (Ep, s). Anatomically all affected vessels were superficial (As) and pathphysiology was caused by reflux (Pr) in all instances. In 36 cases (53.7%), symptoms such as pain (n = 24) or heaviness (n = 22) were present. In half of the cases (n = 33), cosmetic considerations played some role as treatment indication.
Sclerotherapy was performed in GSV (n = 17), SSV (n = 14), PV (n = 36) and TV (n = 50, multiple treatment sites in one session). The most frequent treatment reason was RV veins after GSV surgery (Figure 1); post-thrombotic syndrome was present in five cases (7.5%).
In 52 treatment sessions (77.6%) ‘full success’ was accomplished, 11 sessions (16.4%) gained ‘partial success’ and 2 sessions (3.0%) ‘no success’ (Figure 2); for two sessions, no result was recorded, 27 of the 36 symptomatic patients (75.0%). All but one patient with cosmetic problems (97.0%) reported improvement of signs and symptoms.
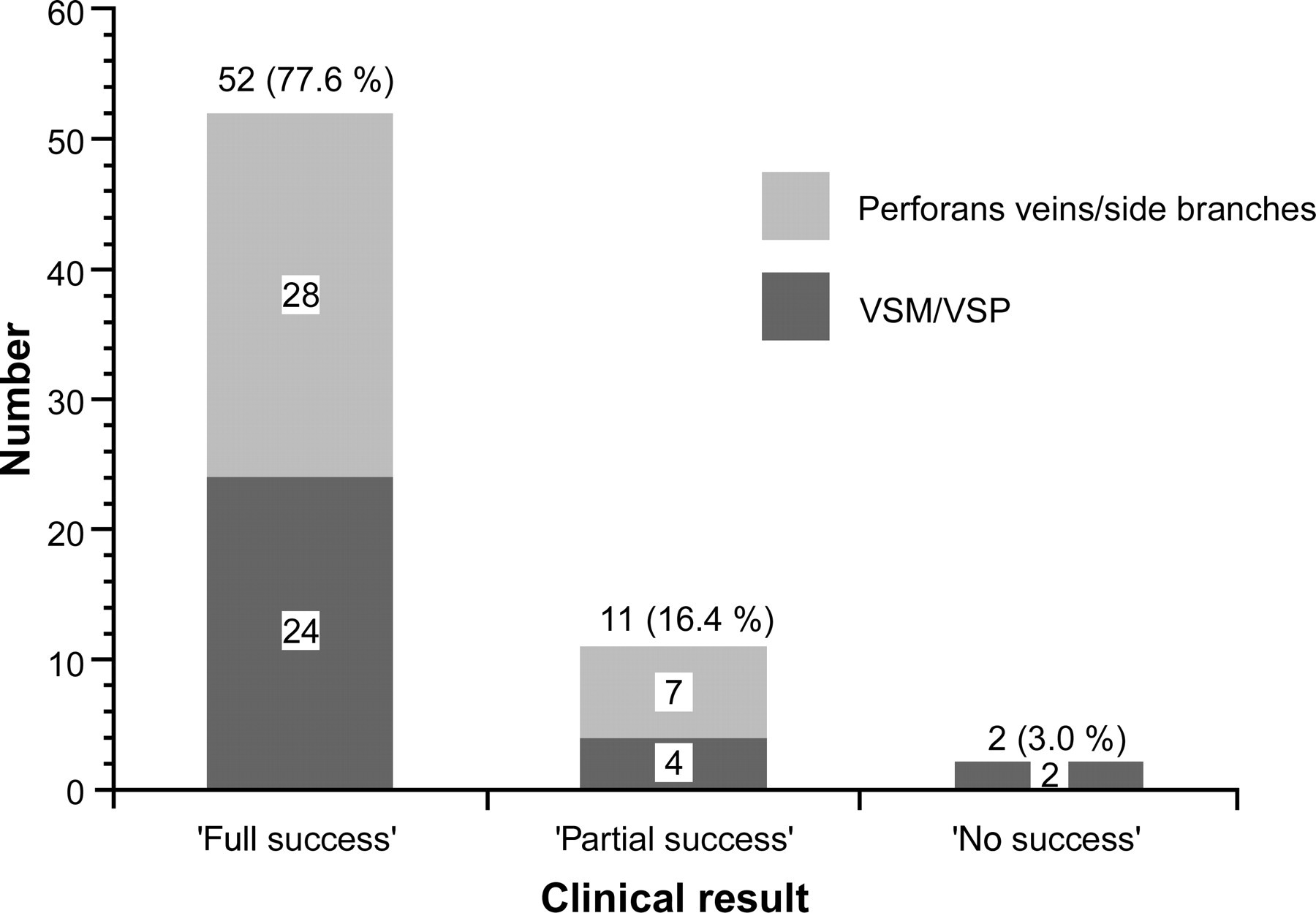
Clinical results of foam sclerotherapy
SVs (GSV or SSV) were treated in 30 cases (44.8%), of which 24 (80.0%) were classified as ‘full success’, four (13.3%) as ‘partial success’ and two (6.7%) as ‘no success’. After sclerotherapy, t 0 increased significantly by 5.9 ± 5.4 seconds, and VC (by 0.8 ± 1.0 mL/100 mL tissue) as well as venous VO (by 11.9 ± 15.6 mL/100 mL tissue/minute) decreased significantly (Table 2). All three results could be replicated for GSV and SSV separately upon independent evaluation.
Results of photoplethysmography (refilling time, t 0) and strain gauge plethysmography (arterial influx, venous capacitiy and venous outflow) before and after 30 sclerotherapy sessions of saphenous veins (Wilcoxon test for pair differences)
SD, standard deviation
Thirty-seven interventions (55.2%) affected non-SVs (PV, TV). Whereas in 31 of those treatments (83.8%) both PV and TV were treated, the remaining six sessions (16.2%) were exclusively aimed at TV. Twenty-eight treatments (75.7%) were rated as ‘full success’ and seven (18.9%) as ‘partial success’. The remaining two had not been classified. After sclerotherapy, t 0 increased (by 2.8 ± 3.0 second) and VC decreased (by 0.2 ± 0.4 mL/100 mL tissue) significantly. Unlike in SVs, VO showed no significant alteration due to therapy (Table 3). The differences could also be replicated for PV and TV separately.
Results of photoplethysmography (refilling time, t 0) and strain gauge plethysmography (arterial influx, venous capacitiy and venous outflow) before and after 37 sclerotherapy sessions of non-saphenous veins (Wilcoxon test for pair differences)
SD, standard deviation
There were no appreciable differences in either aspect of the treatment outcome depending on the underlying condition.
Among patients with non-SV treatment, those previously untreated had shown a significantly longer refilling time than those with RV veins before treatment (21.4 ± 8.8 versus 14.7 ± 3.3 second, P = 0.031). This difference was equalized after sclerotherapy (22.4 ± 8.7 versus 21.8 ± 1.7 second, P = 0.255).
No difference between the groups was observed with respect to strain gauge plethysmography and clinical outcome, respectively.
Relatively unfavourable results were observed in the five patients with post-thrombotic syndrome. Improvement of symptoms was recorded significantly less frequently (25% improved, 75% unchanged) than in the rest of the sample (83.9% improved, 16.1% unchanged, P = 0.0083, 1 patient missing), and there was a non-significant tendency towards worse clinical results. Patients with post-thrombotic syndrome scored ‘full success’ in only 60.0% (versus 83.9% in patients without it), ‘partial success’ in 20.0% (versus 16.7%) and ‘no success’ in 20.0% ( versus 1.7%).
No deep venous thrombosis was detected after sclerotherapy. In 10 cases (14.9%) symptomatic phlebitis with hyperpigmentation in the treated vein developed after treatment.
Discussion
According to the results of the present study, foam sclerotherapy can achieve an improvement of varicose veins in almost all cases and a complete fibrous conversion of the treated vein in about 80%. The results are largely independent of the calibre of the treated vein and the issue of primary versus recurrent disease. Only patients with post-thrombotic syndrome seem to benefit less.
Treatment results were assessed clinically, sonographically, by photoplethysmography and strain gauge plethysmography, which equates the current state of the art. 10 Further emphasis is gained by the fact that the haemodynamic investigations revealed an increase in venous competence of the limb that favourably corresponded with the clinical outcome.
As far as the clinical stage of disease previous to treatment is concerned, our sample presents a higher rate of CVI compared with other studies with less than 10%. 11 More than half of the patients of the present trial had CVI (C3–C6).
Despite the fact that some studies yielded higher occlusion rates of up to or in excess of 90%, 3,11,12 our results correspond favourably with the literature especially when higher C-stages are being considered. A recently published meta-analysis of foam sclerotherapy trials 13 described serious side-effects in 1% (this study 0%), hyperpigmentations in 17.8% (14.9%) and an occlusion rate of 87% (77.6%). Overall pigmentation rates are estimated to be between 10% and 30% 14 placing the present trial in the lower half.
Our observation of an independence of foam sclerotherapy resulting from the calibre of the treated vein is in accordance with a trial by Barrett et al. 15
There is, however, some controversy on the issue of polidocanol concentration. 16,17 Caution is commanded regarding practical application recommendations concerning concentration of the agent.
Foam sclerotherapy bears particular value as an alternative to surgical procedures in RV veins after treatment. Beyond this, it seems to be suitable not only for its traditional domain – TV or PV – but also for the treatment of SSV and GSV. This conclusion is backed by a number of randomized controlled trials, 18–22 which confirm an efficacy for foam sclerotherapy that is comparable to that of surgery and superior to the traditional liquid sclerotherapy. Typically, success rates of 80–90% are to be expected. 4,5,23 This conclusion is supported by recent reviews of sclerotherapy. 12 A Cochrane review on the issue is in preparation. 24
The higher efficacy of foam compared with liquid sclerotherapy is by far not outweighed by the somewhat higher rate of tolerable side-effects. 20 Thus, the formerly unanimous superiority of surgical treatment as compared with sclerotherapy for the treatment of SVs 25 has to be debated in the light of current results. Long-term results of foam sclerotherapy cannot be reliably assessed presently because long-term studies are still missing. Formally, the remodelling process initiated by the polidocanol foam – the complete fibrosis of the former vessel – is irreversible, but the possibility of de novo vein formation has to be considered. 18