
Abstract
Objectives
The destruction induced during endovenous laser treatment (ELT) of the saphenous vein and the perivenous tissue in an animal model (goats) was analysed. Differences in vein wall destruction produced by two laser types, the 980 and 1500 nm diode lasers, were evaluated histologically.
Methods
In 14 goats, 28 lateral saphenous veins were treated with ELT. In 14 veins we used the 980 nm diode laser and in the remnant a 1500 nm laser. Postoperatively the veins were removed at different stages and sent for histological examination.
Results
Immediately removed veins after ELT show an uneven destruction of the vein wall. Veins harvested one week postoperatively show inflammatory tissue at their periphery. Two and three weeks postoperatively, organization is very extensive. In some cases, recanalization begins in a semi-lunar manner at the contralateral side of the laser hit. Veins treated with a 980 nm laser show deeper ulceration with more perivenous tissue destruction compared with veins treated with a 1500 nm diode laser.
Conclusions
The ELT of veins produces an unevenly distributed damage. The cell necrosis is far more extensive than expected.
Uneven vein wall destruction can lead to recanalization. Using a 1500 nm laser correlates with less penetrating ulcerations and more circumferential damage.
Purpose
In this morphological study, we analysed the destruction of the saphenous vein and the perivenous tissue induced by endovenous laser treatment (ELT) in an animal model (goats). We also evaluated the morphological changes in time after treatment. Can histological analysis of the treated veins tell us something about the possible imperfections of ELT? In addition, differences in vein destruction produced by two laser types, the 980 and 1500 nm diode lasers (Intermedic°-Barcelona, Spain), were studied.
Introduction
Endovenous laser treatment (ELT) has become a popular minimal-invasive alternative to stripping in the treatment of saphenous vein reflux. By catheterizing the saphenous vein and introducing a bare fibre into the vein lumen, light energy is delivered intraluminally. This energy is absorbed by blood and water or by the vein wall. The aim of this technique is to obliterate irreversibly the refluxing vein. There are two laser types, one in which there is a higher absorption coefficient for oxyhaemoglobin (810–940–980 nm diode lasers) and a second one in which the energy is preferentially absorbed by water (1320–1500 nm diode laser) (Figure 1). The most commonly used lasers are the 940–980 nm lasers.
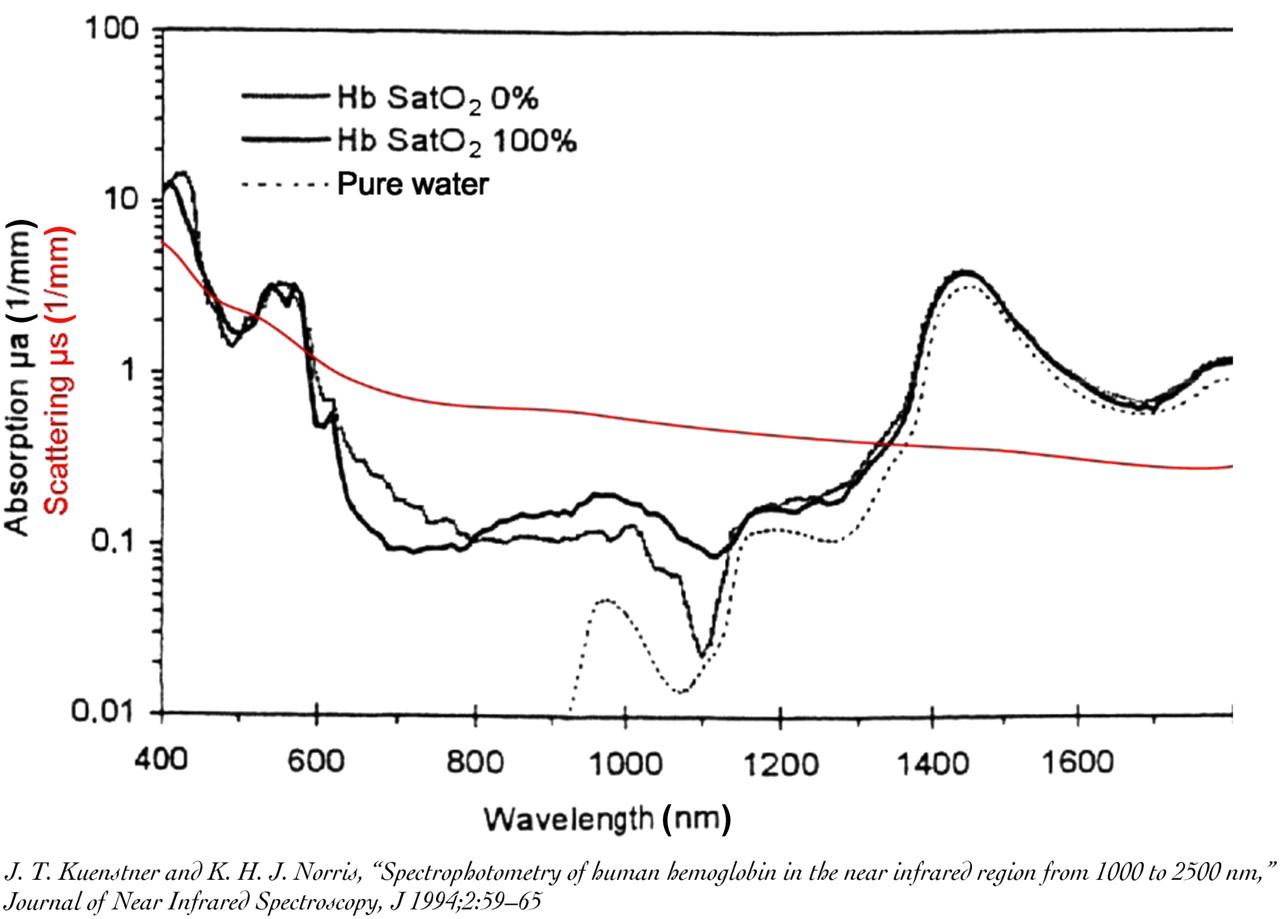
Absorption and scattering coefficients of blood related to wavelength
The 1500 nm diode laser is a new wavelength diode laser with a high energy absorption in water and consequently in the vessel wall. Heat is generated within the zone of optical penetration by direct absorption of laser energy. Absorption is the primary event that allows a laser or another light source to cause a potentially therapeutic (or damaging) effect on a tissue. Without absorption, there is no energy transfer to the tissue and the tissue is left unaffected by light. Scattering of light occurs in all biological tissues: blood, vessel wall and perivenous tissue. Due to fluctuations in the refractive index of these media, the propagation of light into the tissue is modified and the scattering affects ‘where’ the absorption will occur, usually reducing the penetration of light into the tissue. Heating decreases with tissue depth as absorption and scattering attenuate the incident beam. Based on the absorption and effective scattering coefficients of biological tissue, optical extinction (µ eff) can be determined 1,2 (Table 1). This table clearly shows that the optical extinction is much higher at 1500 nm (5–9 times higher) when compared with 810, 940, 980 and 1320 nm. Interestingly, the optical extinction is similar for blood and vessel wall for all these wavelengths. As the biological target is the vessel wall, the vein must be drained of its blood before ELT in order to avoid important attenuation of light by the blood ‘layer’, resulting in insufficient energy to heat up the vessel wall. Furthermore, the absence of blood will avoid the potential creation of an additional layer of carbon around the tip. Finally, the perivenous tissue extinction coefficient is five times lower than that of the vessel wall extinction coefficient. This means that laser light is less prone to be converted into heat by the perivenous tissue, reducing the risk of local complications.
Extinction coefficients (red) related to wavelength and different biological tissues
µ a (mm−1), absorption coefficient in tissue; µ′s (mm−1), reduced scattering coefficient; µ eff, optical extinction
Taking into account these absorption and scattering coefficients of this new wavelength laser (Figure 1), the 1500 nm laser is at least five times more powerful than the 980 nm laser. With less energy, higher selective destruction of the vein wall can therefore be obtained.
Although ELT has fewer side-effects than classical crossectomy and stripping 3 (fewer haematomas, less postoperative pain, paraesthesia and incapacity to work), the technique is not yet perfect. Documented complications are postoperative ecchymosis, pain and periphlebitis. These complications are due to vein wall perforations and energy penetration in the perivenous tissue.
This morphological study therefore aims to examine the possible differences between the two laser groups (980 nm diode versus 1500 nm diode laser). Does the theoretical higher energy absorption in the vein wall using a 1500 nm laser correlate with a more intense and more even destruction? Can this histological study, in which the treated veins are removed at different dates postoperatively, tell us something about the tissue reaction to this treatment and consequently about possible imperfections of the treatment? There have been a number of previously published reports describing vein wall damage following ELT, 4–7 but up to now none of them have studied morphological change over time.
Materials and methods
In 14 goats, 28 lateral saphenous veins were treated with ELT. The goats were treated under general anaesthesia. Under ultrasound control, access was obtained by puncture at the distal part of the lateral saphenous vein. A sheath was introduced and the bare fibre (600 µm) was localized near the saphenofemoral junction. Physiological fluid was injected abundantly around the saphenous vein inducing spasm of the vein and acting as a protective barrier to the perivenous tissue. We injected on average 120 mL of liquid around the target veins, which is 7.95 mL/cm.
In 14 veins we used the 980 nm diode laser and in the remainder a 1500 nm laser (Intermedic°-Barcelona, Spain).
Postoperatively the veins were removed at different stages (Table 2) and sent for histological examination. Unfortunately, one goat died in the postoperative period, without the veins being harvested. The pathologists measured the diameter of the ulcerations, as the depth of penetration in the vein wall using different optical lenses. Each optical field correlates with a constant defined diameter. Some lenses are scaled, which allows exact measurement of the specimens.
Vein removal data
The mean diameter of the veins was 0.54 cm (standard deviation [SD] 0.09), measured in the supine position.
We use the term linear endovenous energy density 8 for the energy amount in joules divided by the treated vein length in centimeters. On average, 52.8 and 27 J/cm were administrated, respectively, for treatment with the 980 and 1500 nm laser. The term endovenous fluence (EF) 9 is used for the quotient of delivered energy in joules to the approximated inner vessel surface. The mean energy deposits (EF) were 30.29 J/cm2 (SD 12.15) using a 980 nm laser and 16.75 J/cm2 (SD 8.47) using a 1500 nm laser. The mean length of the treated vein was 15.06 cm (SD 1.02) (Table 3). The reason for using lower energy deposits with the 1500 nm laser is that a 1500 nm wavelength has a stronger energy absorbtion in the vein wall compared with the 980 nm wavelength (Figure 1). The higher optical extinction in the vein wall using a 1500 nm laser permits one to use lower energy deposits (Table 1). We were looking for the optimal fluence related to the wavelength. The used energy levels have been extrapolated from clinical use.
Energy deposits
SD, standard deviation
The lateral saphenous vein in a goat has a mean diameter of 5–6 mm in supine position which is comparable to human veins. The treated animals do not have varicose veins and therefore the thickness of the vein wall is somewhat lesser than that of human varicose veins. Goat saphenous veins are a good model, although not exactly like human varicose saphenous veins.
Our experiments were approved by the ethics committee for animal experiments at the Catholic University of Leuven, Belgium.
Statistical evaluation
Statistical analysis was performed using Statistical Package for the Social Sciences 16.0 (SPSS). Intergroup variances for unpaired continuous and ordinal data were evaluated non-parametrically by the use of the Mann-Whitney U test. An α-level of significance of 0.05 was used.
Results
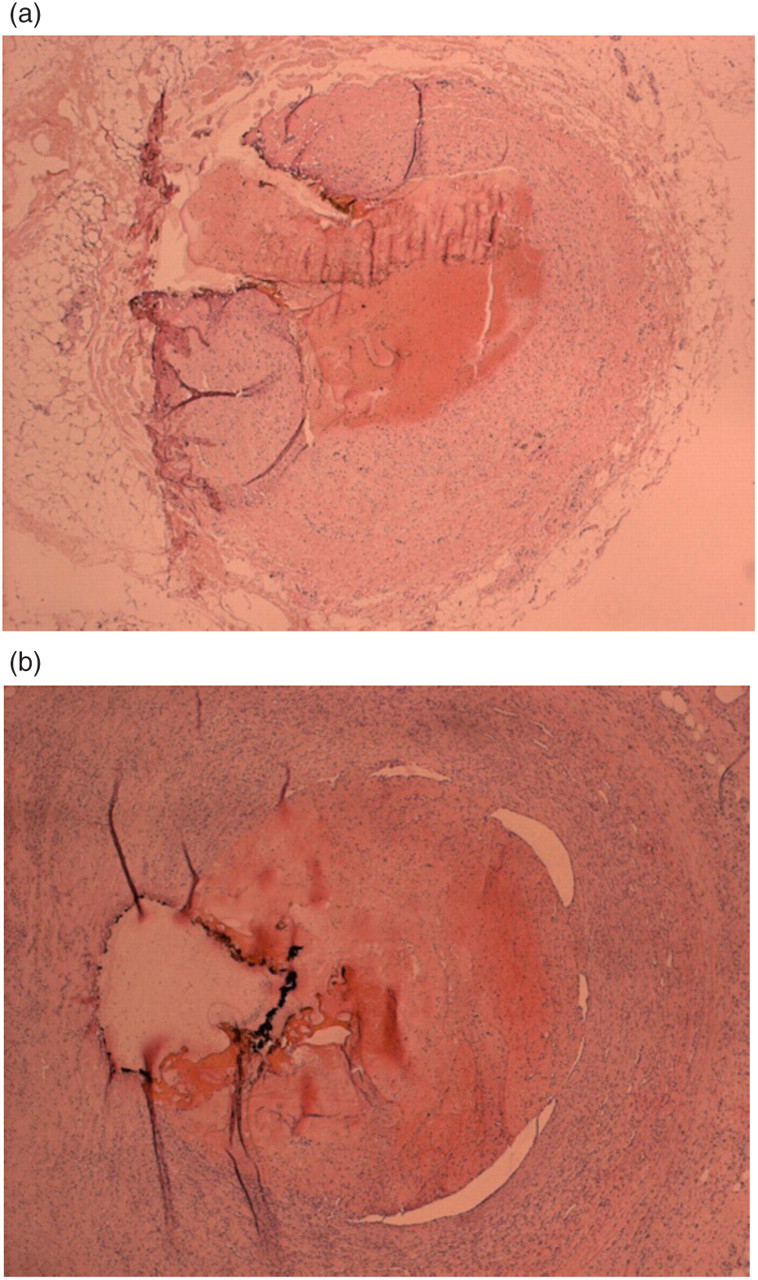
Veins removed immediately after ELT show an uneven destruction of the vein wall with perforations and ulcerations, due to direct contact of the fibre tip and the vein wall (Figure 2). The contralateral sides of the vein are not damaged and remain unaffected. The ulcers in the veins treated with a 1500 nm laser are larger (Tables 4 and 6). The 980 nm laser probably induces more perforations of the vein wall, but the difference is not always very clear. The 980 nm laser induces more carbonization in the vein wall than the 1500 nm laser. This carbonization is found at the point of direct laser impact.
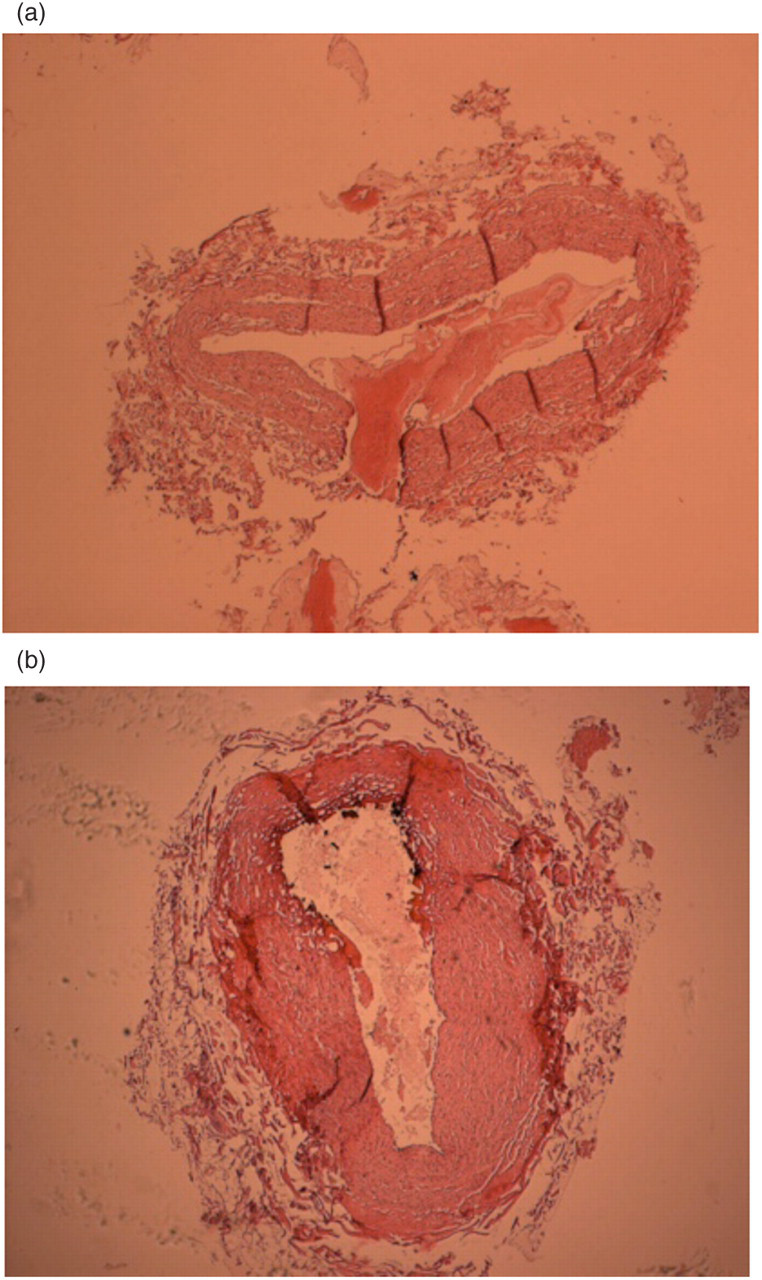
Veins removed immediately showing ulcerations and perforations. (a) 980 mn laser treatment and (b) 1500 nm laser treatment
Diameter and depth of the ulcerations of the treated veins
SD, standard deviation
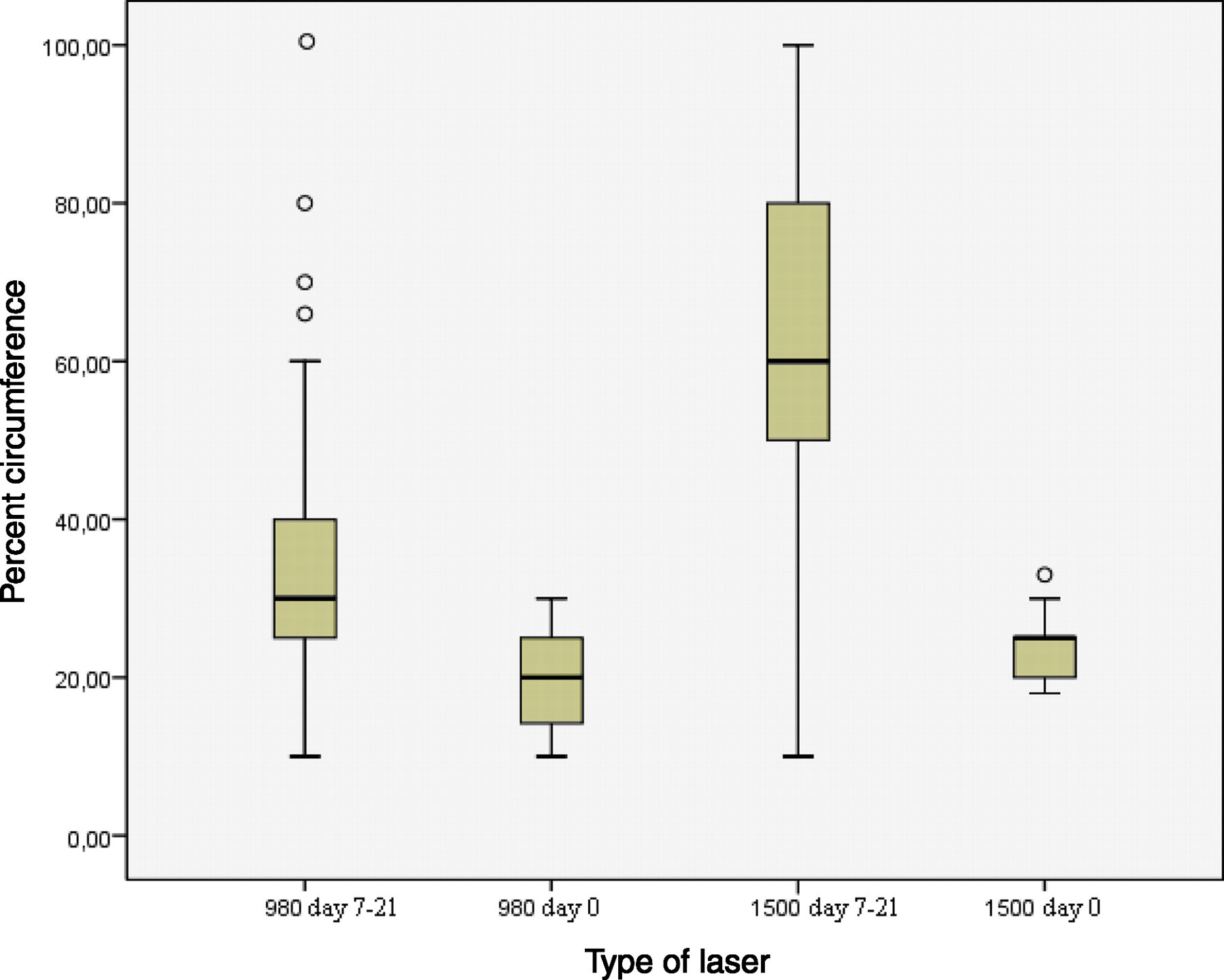
Mean percentage of circumferential vein wall destruction in veins treated with a 980 nm and a 1500 nm laser, immediately removed (day 0) and removed one week or later after treatment (days 7–21)
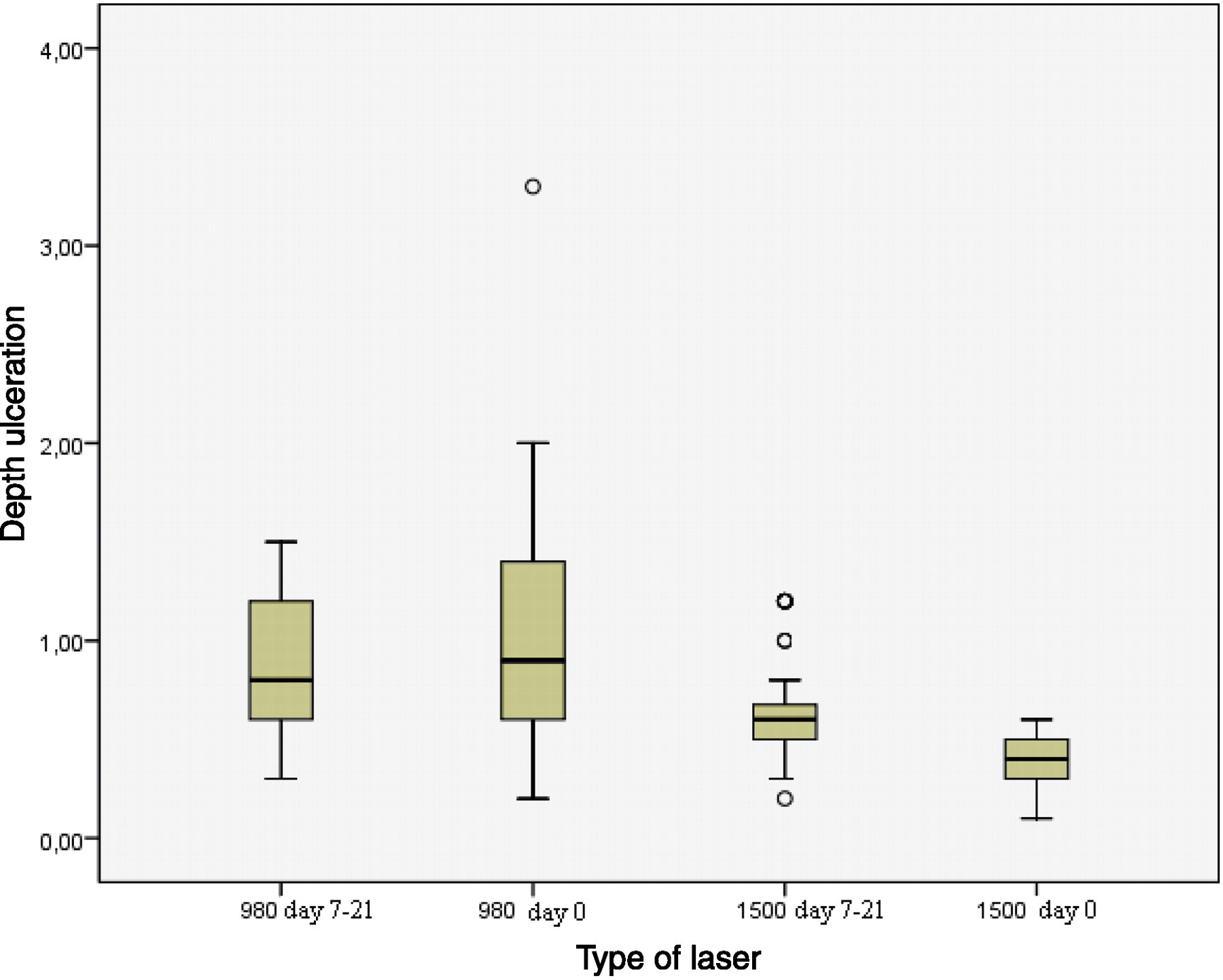
Depth of the ulcerations in veins treated with a 980 nm and a 1500 nm laser, immediately removed (day 0) and removed one week or later after treatment (days 7–21)
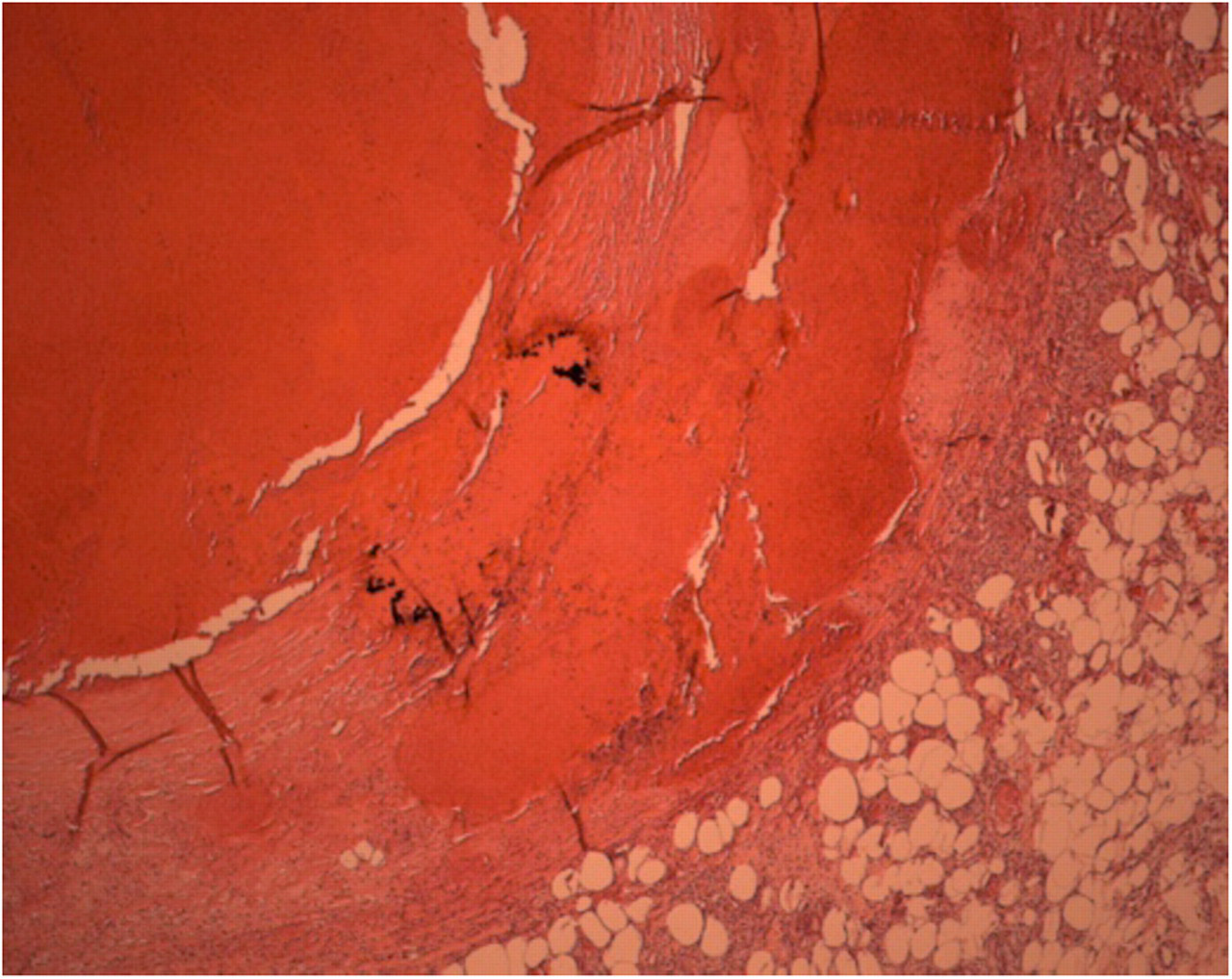
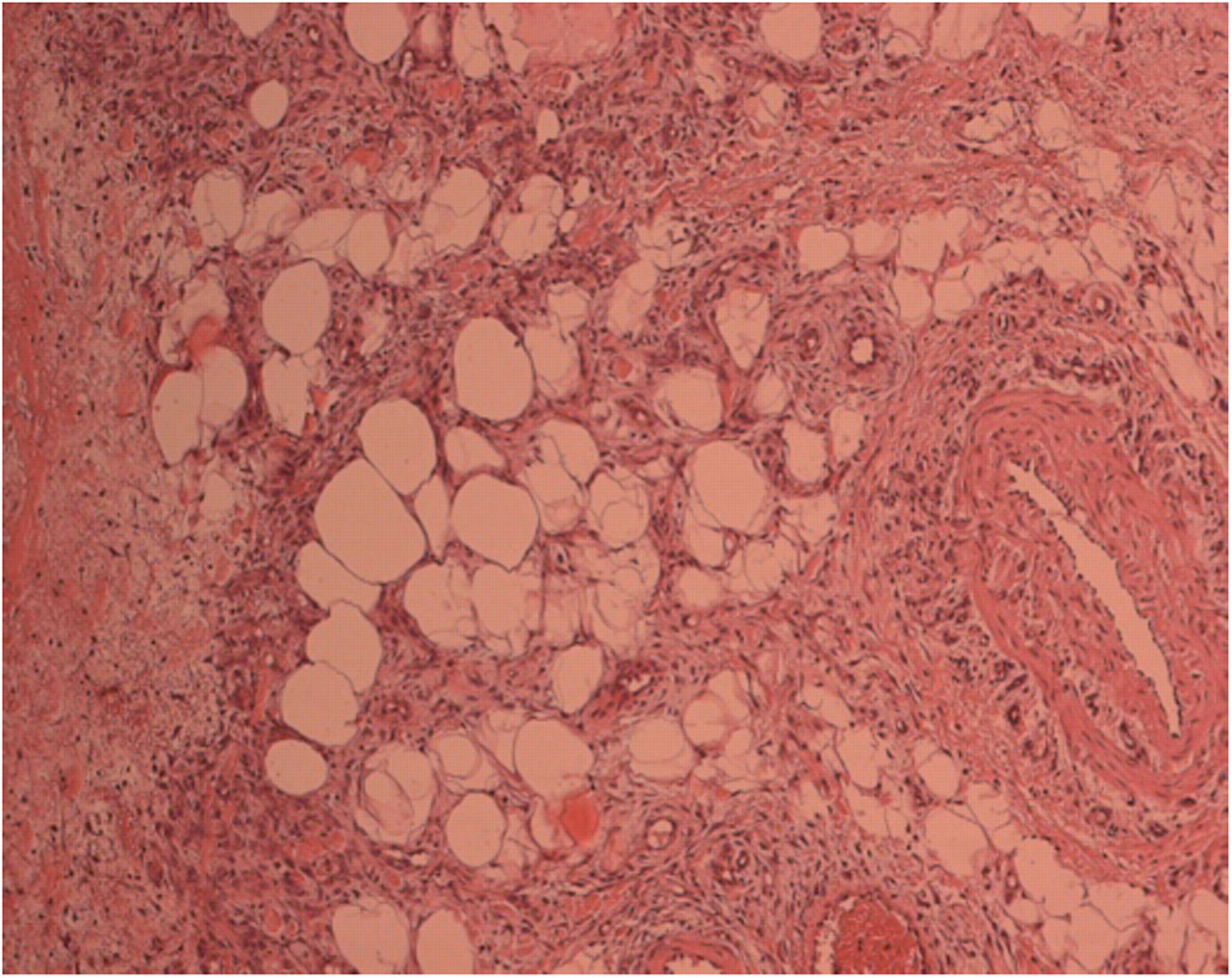
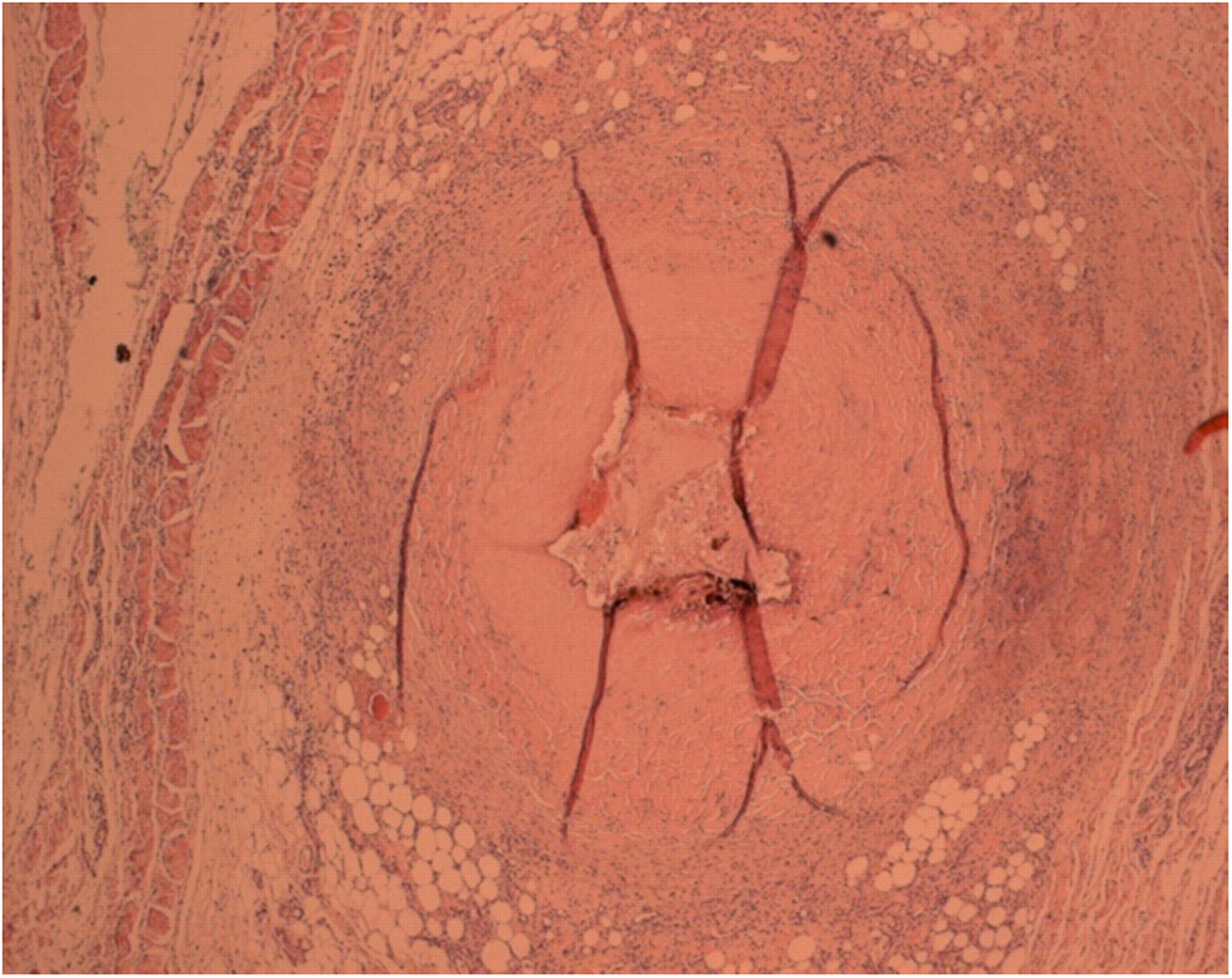
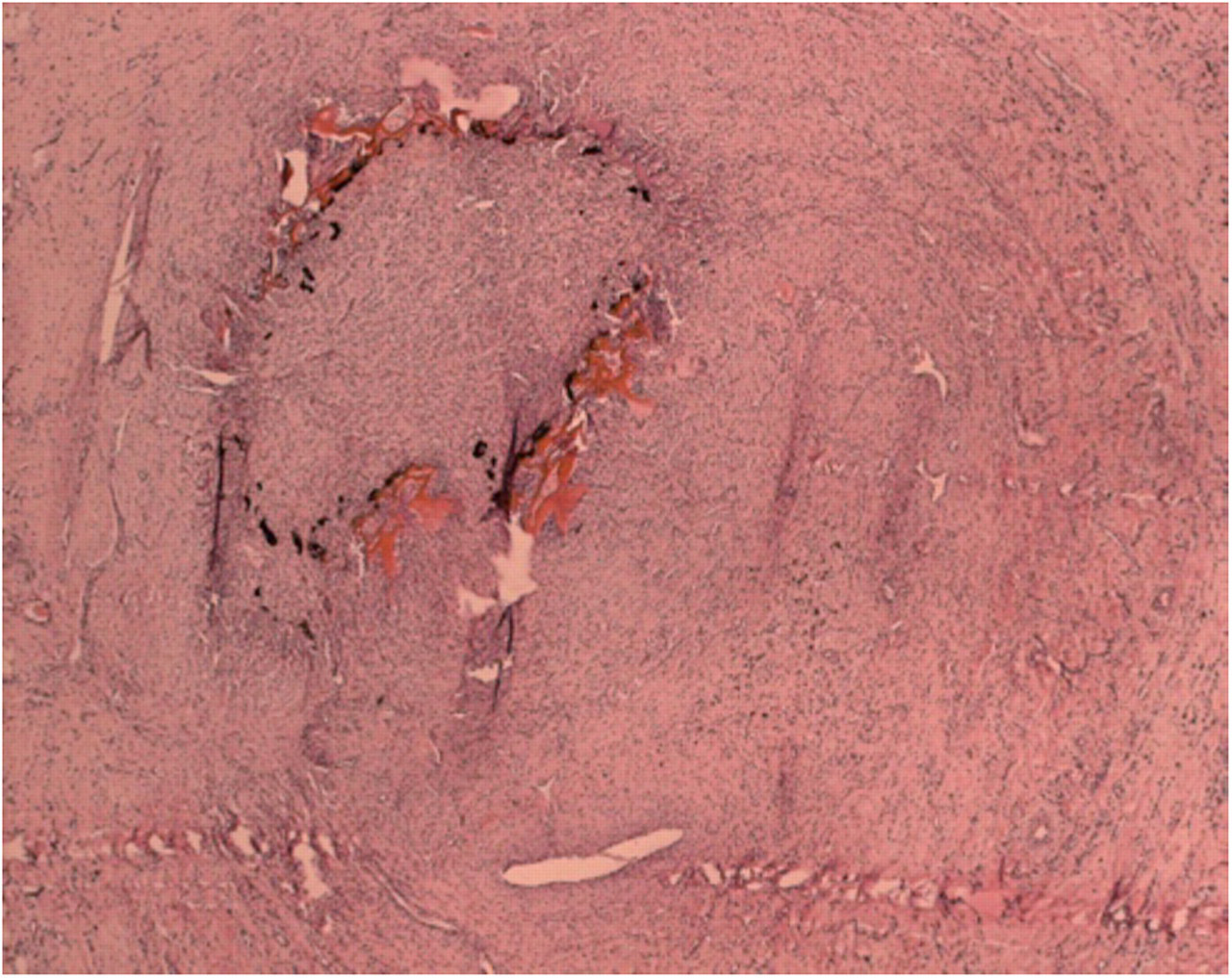
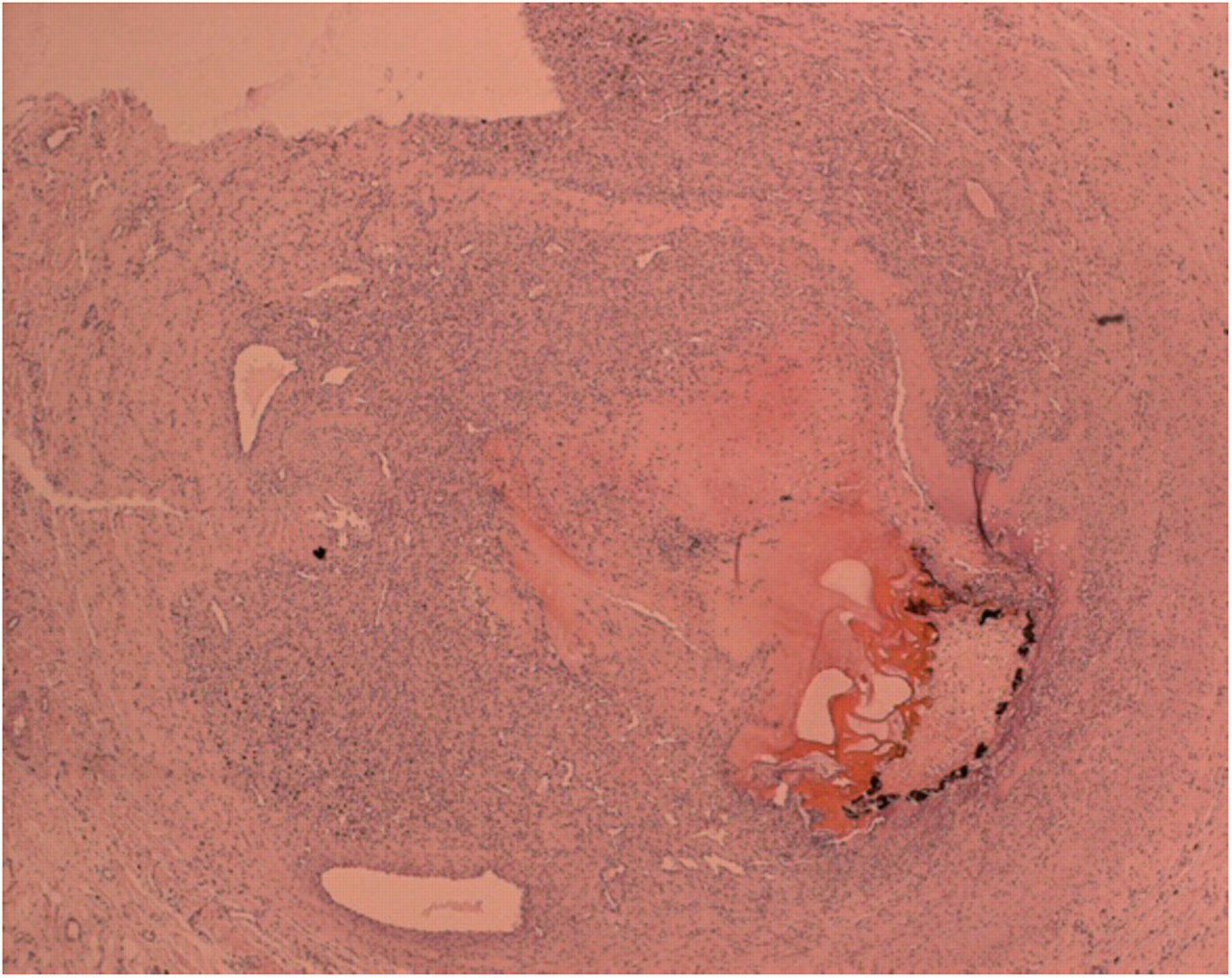
Veins harvested one week postoperatively show cellular inflammatory tissue at their periphery with the formation of new vessels and endothelial cells and migration of fibroblasts and phagocytes (Figure 3) at a distance from the ulcerations. All these veins show thrombus formation and occlusion of the vein and the blood is denatured; all the cells are dead and there is no organization of the thrombus in the lumen (Figure 4). Major parts of the vein wall are destroyed and muscle cells are necrotic, but in an uneven distribution. At the perforation sites, destruction of the perivenous tissue is seen. At these points, the organization and migration of cells are much slower and limited (Figure 4). Perivenous tissue destruction can be found at a distance from the treated vein using a 980 nm diode laser (Figure 5), affecting small vessels at a distance of the treated vein.

Formation of inflammatory tissue around a treated vein
Denatured and ‘boiled’ blood inside the vein. Vein wall with ulceration, carbonization and extravasation. Formation of limited inflammatory tissue at this point; 980 nm laser treatment, one week postoperatively
Inflammatory tissue around the treated vein wall. A small vein at a distance of 2 mm from the treated vein surrounded by inflammation tissue. The cells of the vein wall are denatured and dead, probably due to the heating. 980 nm laser treatment at seven days
Two and three weeks postoperatively, organization in and around the vein walls is very extensive. Inflammatory tissue around the treated veins shows the formation of new small vessels accompanied by macrophages and histiocytes, dissolving the destroyed tissue and forming scar tissue.
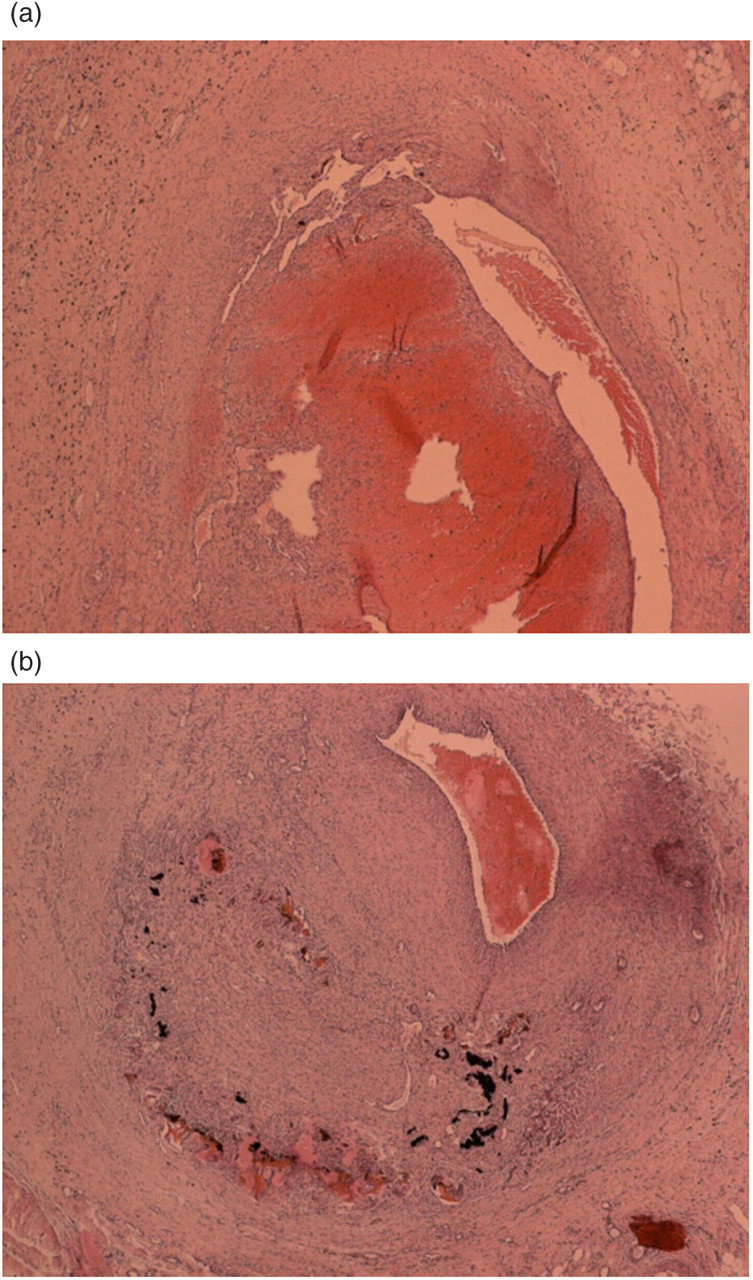
A more even destruction of the vein wall is found after treatment with a 1500 nm diode laser, with less eccentric vein wall destruction (Figures 6 and 7). In some veins, carbonized tissue is surrounded by cellular and inflammatory scar tissue (Figure 8). Some organization of the intraluminal clot is seen, with ingrowth of endothelial cells and phagocytes at the edge, especially at the proximal or distal end of the treated veins (Figure 9). At points of perforation of the vein wall, there is deeper destruction of the perivenous tissue (Figure 6). The appearance of reactive tissue at these sites is limited, and more perivenous tissue is destroyed. Veins treated with a 980 nm laser show a transmural destruction of the vein wall in a semi-circular manner, affecting on average 33% of the circumference (Table 4). The residual wall shows variable necrosis of the muscle cells with infiltration of inflammatory tissue and reorganization. Veins treated with the 1500 nm laser exhibit broader areas of tissue destruction, taking up 62% circumference on average (Table 4), with more homogeneous damage of the vein wall at a distance from the point of direct laser impact.
Vein wall perforation with perivenous tissue damage. Limited (or delayed) organization at the points of perforation and perivenous tissue injury. (a) 1500 nm laser treatment, day 16 and (b) 980 nm laser treatment, day 18
Complete necrosis of the tunica media, surrounded by inflammatory tissue; 1500 nm laser treatment, day 21
The carbonized tissue is surrounded and encapsulated the inflammatory tissue; 980 nm at 18 days
Organization of the clot, with ingrowth of phagocytes. Circumferential necrosis of the vein wall, carbonization at the point of direct laser impact; 980 nm laser treatment, day 18
In some cases recanalization begins in a semi-lunar manner at the contralateral side of the laser impact (Figure 10). This part of the vein remains unaffected, and a new endothelial layer is formed at the opposite side. The destroyed part is infiltrated by macrophages and neutrophilic granulocytes that clean up the carbonized tissue.
Formation of a new endothelial layer near the untouched contralateral side, leading to recanalization. (a) 1500 nm laser treatment, day 16 and (b) 980 nm laser treatment, day 18
The intraluminal content is preferentially damaged with eosinophilic denaturation of the intravascular material.
From the 26 harvested veins, 186 sections were taken for histological examination. As we were looking for morphological differences between the two laser types, we selected 128 sections in which an ulceration was cut transversally. Eccentric or longitudinal cuts through the ulcerations were not included. From these 128 sections, 59 were taken from veins treated with a 980 nm laser and 69 from veins treated with a 1500 nm laser. In all the sections, we measured the depth of the ulcer as well as the diameter of the destroyed tissue (Tables 4–6; Figure 11). As the measured diameter is not exactly the original diameter due to spasm of the vein after treatment and due to the shrinkage postfixation, we preferred to express the diameter as a percentage of vein wall circumference. The depth of the ulceration was measured in millimeters. In the immediately removed veins, we found a statistically significant difference in depth and diameter comparing the two wavelengths: ulcers in the veins treated with a 980 nm laser are deeper (P < 0.001) but affect a smaller part of the circumference (P = 0.01). In the veins harvested one week postoperatively and later, the exact border of the ulcer due to direct contact is often difficult to outline. At a distance of the point of direct contact major parts of the vein wall are destroyed and muscle cells are necrotic, but in an uneven distribution. We measured the part of the circumference where complete destruction was found and expressed it as a percentage of circumference of the vein wall (Figure 11). Depth was measured at the point of direct contact. Again we find a significant difference comparing both wavelengths: in veins treated with a 980 nm laser the ulcers are much more penetrating but the circumferential destruction is significantly lower (P < 0.001) (Tables 4–6).
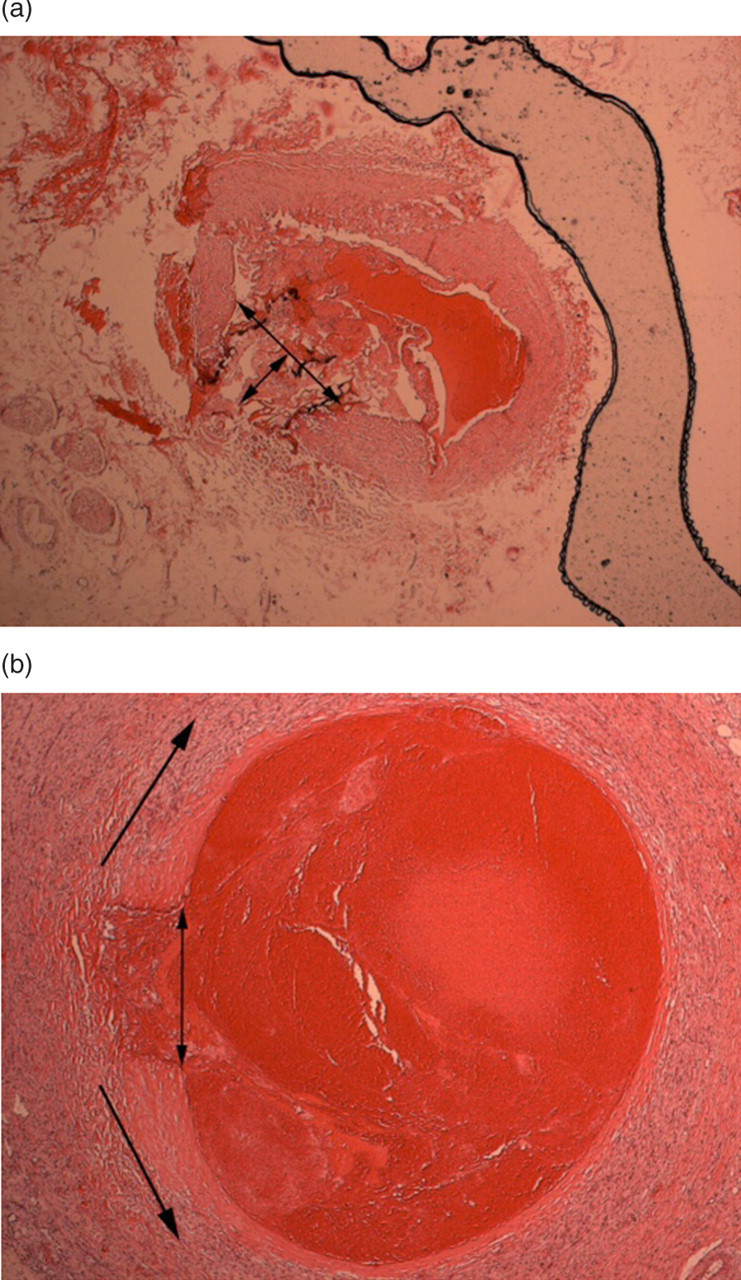
Measurements of depth and diameter of ulceration (day 0) and circumferential total destruction (day 21). (a) 980 nm day 0: depth 0.3 mm, ulcer takes 15% of the circumference and (b) 980 nm day 21, 28% of the circumference shows total destruction
Discussion
The ELT of saphenous vein reflux is a popular alternative treatment to classical crossectomy and stripping, and is proven to be safe and effective. 10,11 Nevertheless, this new technique still has some imperfections such as postoperative ecchymosis, pain, bruising and periphlebitis. These complications may be due to uneven energy application during the procedure. 4 When the laser fibre is introduced into a saphenous vein, which usually has some small twists and turns, the fibre always has a tendency to stretch. As a consequence of this stretching, the fibre tip frequently hits the vessel wall. Examining the fibre localization on peroperative ultrasound control, we found the fibre tip to be situated most often very eccentrically in the vein, with the tip touching the vein wall. 9 Tumescent anaesthesia induces spasm of the vein around the fibre and can diminish this effect. Even then, however, especially in larger veins, the fibre tip remains eccentric. In larger veins, the vein folds in the tumescent fluid and this hampers uniform energy distribution to the vein wall.
When energy is delivered from the fibre tip in such a situation, direct contact between the fibre tip and the vessel wall results in destruction and ulceration or perforation of the vein. 9 This correlates with our histological findings examining the removed veins: the immediately removed veins show ulcerations and perforations, and the rest of the vein wall remains untouched (Figure 2). These ulcerations are broader in veins treated with a 1500 nm laser, but on the other hand the ulcerations and perforations are deeper in veins treated with a 980 nm laser (Table 4).
Nevertheless, when we examined the veins removed one week later, the destruction of the treated veins appears to be far more extensive than in the immediately removed specimens. At the point of ulceration and perforation the cells are all destroyed, and outside the vein tissue necrosis is noted, due to energy leakage through the perforations especially in veins treated with a 980 nm laser (Figures 4 and 5). Perivenous tissue destruction was found at the closed proximity of the target veins. This tissue might be attached to the vein after tumescent injection. The liquid injection certainly diminished the non-target tissue destruction but could not avoid it completely.
However at a distance from these perforations, the cells of the media and intima show necrosis and a cell-rich necroinflammatory process accompanied by fibrosis surrounds the vein. This process takes place to eliminate the dead cells and to reorganize the vessel wall into scar tissue (Figure 3). This cell necrosis can only be the result of the thermal energy created by absorption of the light energy. If the temperature rises above 42°C, protein denaturation starts. Due to the transformation of light energy into thermal energy, the temperature in and around the treated vein rises. 12 The vein wall cells at a distance from the point of direct laser impact are heated and their intracellular proteins denature. As a consequence of this protein denaturation, the cells become necrotic. This effect cannot be seen if the vein is removed immediately, but only later.
This secondary cell destruction can be circumferential or semi-circumferential. If the vein wall is not circumferentially destroyed, the damaged part can be encapsulated and a semi-lunar recanalization can be formed (Figure 10). This can be seen at the contralateral side of the direct laser impact. So incomplete endothelial destruction can lead to recanalization. Clinically, this explains the higher recanalization rate in larger veins, if the delivered energy is not sufficient: after catheterization and injection of fluid around the saphenous vein, the vein will fold and the fibre will be located eccentrically in the lumen. In such a case, it will be difficult to destroy the endothelial cells at the contralateral side of the vein.
These recanalizations can give rise to varicose recurrence. Using a 980 nm laser the recanalization rate can reach 10% six months postoperatively. 9,13,14
There is still a discussion about the mode of action of ELT. The light energy released from the fibre tip is absorbed by the blood and/or the vein wall. Proebstle et al. stated that laser-induced local heat injury of the inner vein wall by steam bubbles originating from boiling blood is the pathophysiological mechanism of action of the ELT. 5,15 Mordon, 16 Zimmet 17 and Fan and Rox-Anderson 18 stated that the steam produced by absorption of laser energy by the blood is a tiny fraction of the energy necessary to damage the vein wall and cannot be the primary mechanism of injury to the vein with an endovenous laser. The bubbles grow, and when they extend into a cooler area they collapse. The boiling zone is therefore within the lumen of the blood vessel and vapour bubbles have no effect on the vessel wall. Steam bubbles originating from boiling blood cannot be the pathophysiological mechanism of the action of ELT.
The carbonization and tract within the vein walls seen by histology following endovenous laser treatment can only be the result of direct contact between the laser fibre tip and the vein wall. Consequently, light absorption by the vein wall would be the main mechanism. As the presence of blood could reduce the light transmitted to the vein wall, it is usually recommended that the vein lumen is emptied, using leg elevation (Trendelenburg positioning) and perisaphenous subcutaneous tumescent saline solution infiltration. Concerning patient positioning, Desmyttere et al. 19 have demonstrated that clinical results were statistically superior when the great saphenous vein was emptied of its blood. If the laser light energy is entirely absorbed by the blood, the initial success rate is mainly due to a thrombotic effect but thrombus dissolution leads to recanalization. 13 Burning of the vein wall by local contact between the fibre tip and the inner vein wall could be the mechanism of action. Tissue effects, such as ulceration and perforation, are achieved not only by direct absorption of laser light, but by convection of heat energy from the fibre tip into the surrounding tissue. 18,20 At these points of direct contact the temperature can rise to 300°C. Due to heat dissipation, vein wall cells at a distance from this point of direct laser impact become necrotic. This can only be seen in the veins removed after one week or later. Furthermore, by emptying the vein, the light energy will be absorbed by vein wall cells directly and converted to thermal energy. The cytoplasm will be heated causing denaturation of intracellular proteins. So not only direct contact but also light energy absorption by intracellular cytosol of vein wall cells takes part in the mechanism of action of ELT.
The energy delivered from the 980 nm diode laser is, compared with the 1500 nm wavelength laser (Figure 1), less well absorbed by the vein wall cells and induces more local convection of heat energy. This explains the deeper ulcerations and the more intense carbonization (Figures 2, 4, 6, 8 and 10) at the points of direct laser impact. Therefore, using a 1500 nm laser gives less eccentric vein wall destruction with less penetrating ulcerations. These findings could correlate clinically with less perivenous tissue destruction and less postoperative pain using a 1500 nm laser, but of course this should be controlled by a comparative prospective clinical trial.
The formation of a cell-rich necroinflammatory process at a distance from these perforations is responsible for the cicatrization of the treated vein, resulting in a fibrotic cord several months after treatment. This is the most important morphological effect of laser treatment on vein walls.
Conclusions
The ELT of veins gives an unequally distributed damage to the vein wall, due to direct contact of the fiber tip and the vein wall. This results in perforations and perivenous tissue injury. The destruction is more penetrating using the 980 nm laser. The 1500 nm laser gives less eccentric venous wall injury with broader ulcerations. Vein wall destruction and cell necrosis are much more extended than was expected. Uneven vein wall destruction can lead to recanalization of the treated veins. Using a 1500 nm laser could correlate with more homogeneous vein wall destruction, with less perivenous tissue destruction and possibly with less postoperative pain.
Footnotes
Acknowledgements
This trial was funded by Bard Benelux, Sanofi-Aventis and Datascope.