
Abstract
Objectives
To discuss the differential diagnosis of a case with leg swelling and pain with special emphasis on soft-tissue malignancy.
Methods
Symptomatic deep vein thrombosis (DVT) of lower limb was treated with standard anticoagulants. In view of persistent symptoms for three months, repeat duplex venography, magnetic resonance imaging (MRI) and biopsy were undertaken to uncover the underlying pathology.
Results
Imaging and biopsy revealed a 5 × 11 cm myxoid liposarcoma, adherent to the vein, that was the cause of her persistent symptoms despite anticoagulation, possibly by its local mass effect and also by its potential to create a thrombogenic milieu. Excision of the tumour led to symptom relief. A Medline search of English language papers was undertaken to review related literature.
Conclusion
The report highlights the importance of considering neo-plastic masses as differential in painful leg swelling. Diagnosis is made by a high index of suspicion in atypical cases and confirmed by follow-up duplex or MRI. Treatment involves surgical excision that provides symptom relief as well as avoids potential tumour extension.
Introduction
The differential diagnosis of painful leg swelling, a common clinical presentation, includes deep vein thrombosis (DVT), cellulitis and ruptured Baker's cyst. Prompt evaluation to screen out a DVT is usually undertaken in the form of non-invasive imaging studies in view of high associated likelihood of complications related to a delay in anticoagulation initiation. Rarely may the imaging study be positive in an initial evaluation only to later reveal a pathology that, although different, imitates or co-exists with a venous thrombus. Various local inflammatory, vascular or neoplastic masses fall into such category. As the presented case illustrates, persistent symptoms of DVT while on appropriate anticoagulation should initiate a search for such pathologies as the management and prognosis are entirely different. The case also highlights the importance of a thorough duplex evaluation in all cases of suspected DVT.
Case report
A 42-year-old woman on combined formula birth control pills for 20 years and with a 20-pack-year history of smoking was diagnosed with ‘idiopathic’ DVT in the right distal femoral vein and the popliteal vein by her primary care physician. She was treated with therapeutic dose Enoxaparin and transitioned to Warfarin to maintain at an international normalised ratio (INR) range of 2–3. She did not have a prior history or family history of venous thromboembolic disease or miscarriages. She was also up-to-date on age appropriate cancer screening. She was referred to our vascular institute three months later as she had persistent right thigh ache and leg swelling despite adequate anticoagulation (INR checked every week and maintained within the range of 2–3).
On clinical examination she had trace oedema of the right calf area, but there was a focal swelling in the medial aspect of the distal thigh. We repeated the venous duplex study due to the continued symptoms and focal swelling of the thigh. Surprisingly, we identified a 5 × 11 cm mass that seemed to have arterial and venous supply in the distal thigh close to the femoral vein and superficial femoral artery (Figure 1) along with a DVT in the distal femoral and popliteal vein. The venous duplex study from the outlying vascular lab, saved as still image files, was reviewed thoroughly and there was no evidence of a mass in this study (Figure 2). As such, we felt that the prior study was in fact incomplete. A soft-tissue tumour was suspected based on our duplex examination and eventually confirmed by magnetic resonance imaging (Figure 3). Biopsy and histopathological examination suggested myxoid liposarcoma. With appropriate perioperative anticoagulation, she underwent a wide local excision of this tumour mass that was found to be adherent to the femoral vein and superficial femoral artery. During surgery, multiple small tumour vessels were noted arising from the femoral vessels that were clipped and dissected free of the tumour. She also received adjunct presurgical radiation therapy and intraoperative brachytherapy. No evidence of hypercoagulable state was identified after extensive testing; as such the DVT was felt to be secondary to the soft-tissue tumour. She was completely asymptomatic and had no evidence of malignancy at a six-week follow-up visit with her oncologist.
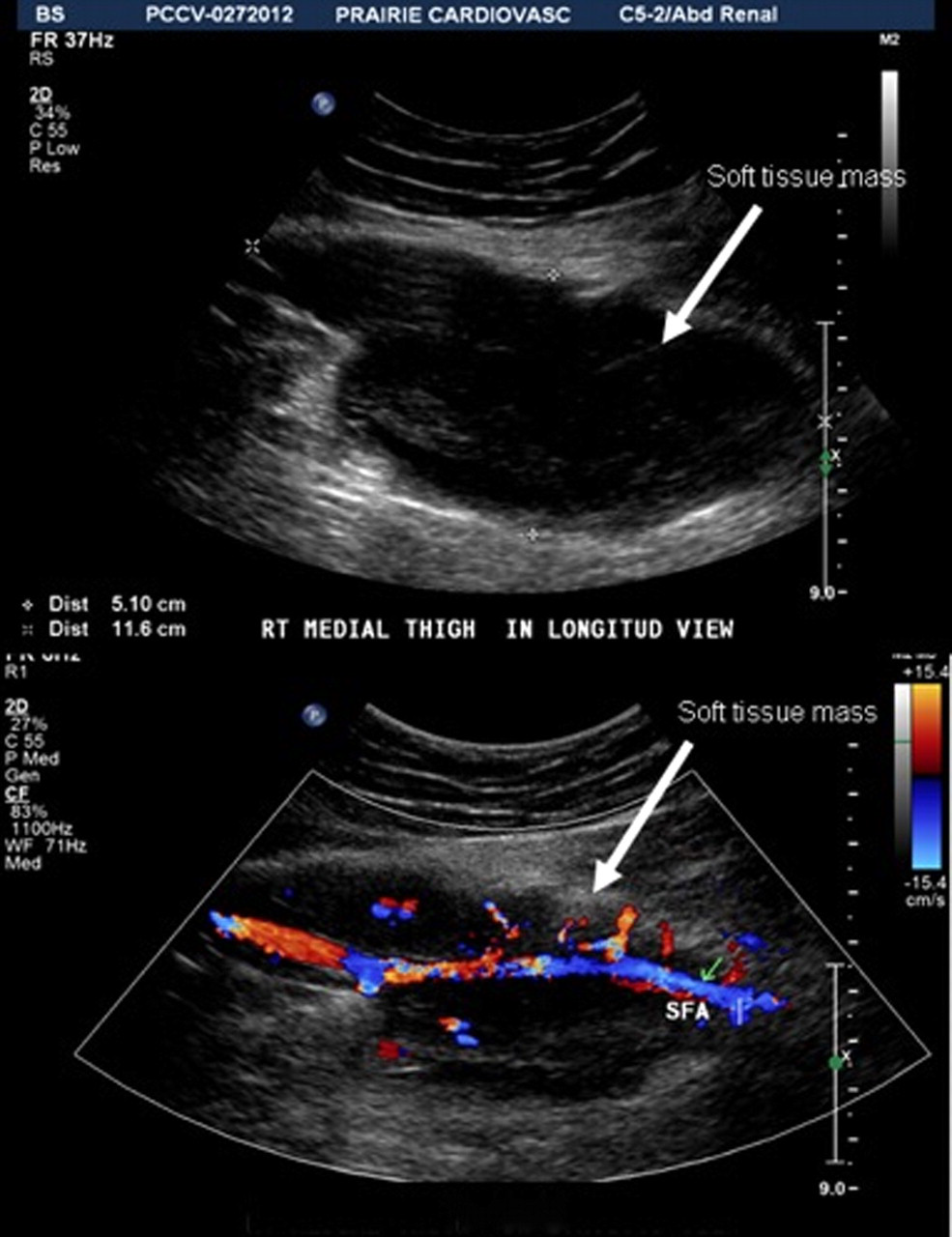
Soft-tissue mass with vascular supply noted (arrows)
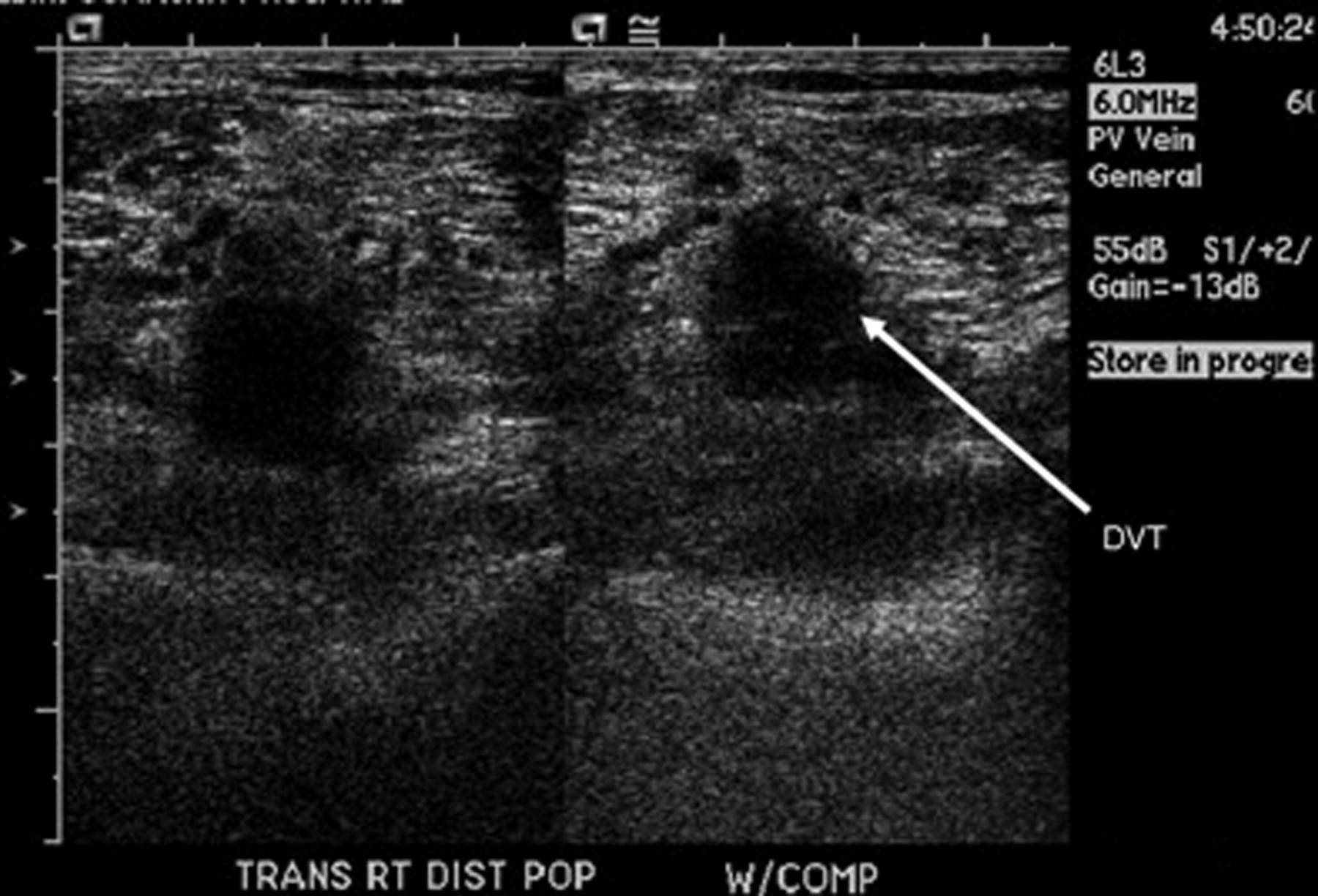
Venous duplex performed at an outlying vascular laboratory for the initial evaluation documenting the deep vein thrombosis (arrow) without any evidence of tumour mass
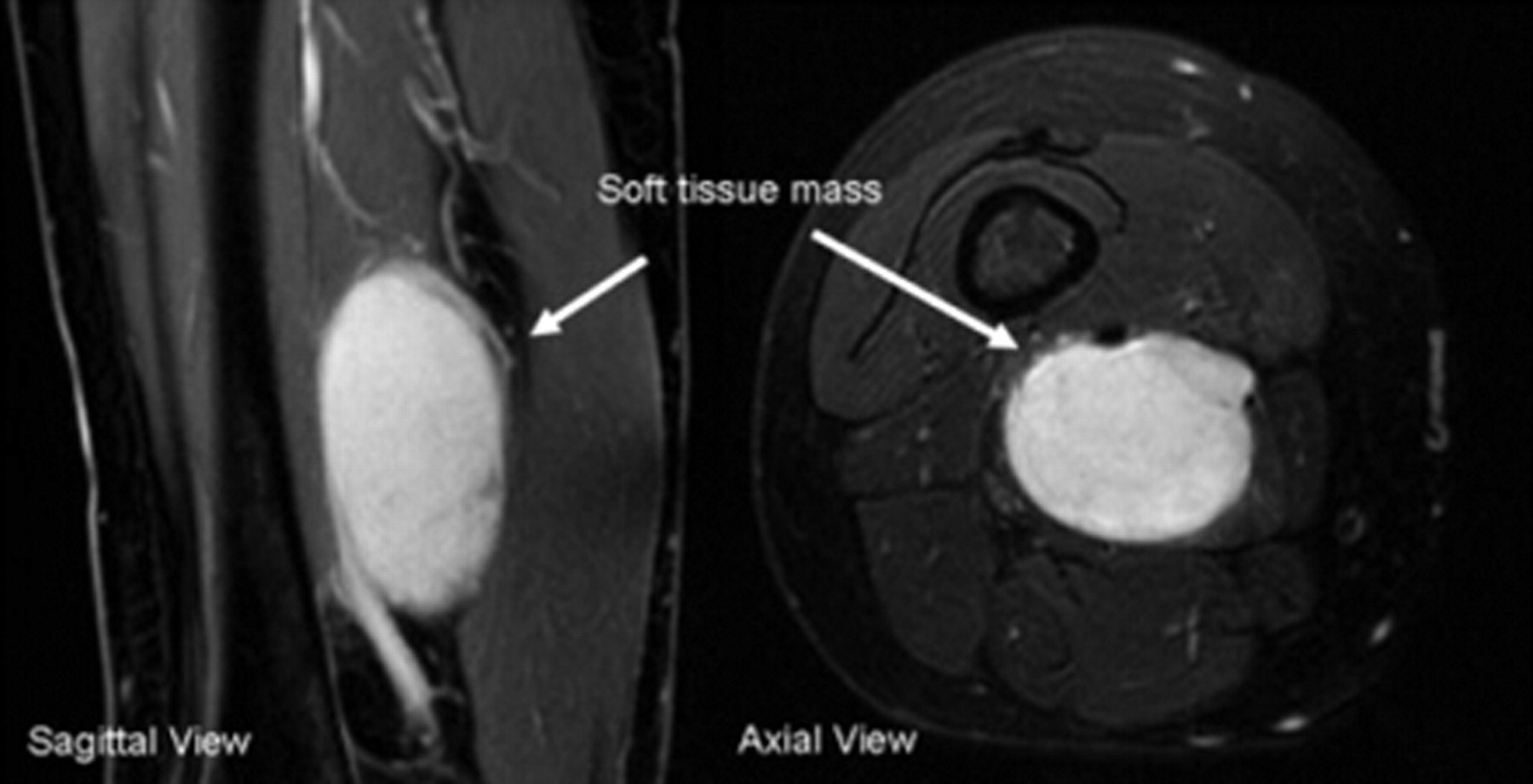
Magnetic resonance imaging of the thigh confirming the tumour mass (arrows)
Discussion
The most common differential diagnosis considered in patients undergoing venous duplex ultrasonography for a chief complaint of leg swelling includes DVT, ruptured Baker's cyst and cellulitis. Neoplastic masses are rare but important for a variety of reasons. As this case demonstrates, they should be considered even if a DVT has been documented on duplex. Moreover, a complete duplex evaluation should be performed in all cases of suspected and diagnosed DVTs. Appropriate image, preferably cine loop, records should be saved and be available for later review.
The majority of soft-tissue sarcomas are localized in extremities. Their prevalence in patients evaluated with venous disease is small. In a series of more than 200 patients evaluated for venous disease, only three patients had neoplastic masses. 1 One out of the three cases was a myxoid sarcoma. Despite their rarity they are important as these sarcomas are serious and potentially fatal malignant tumours characterized by local extension and occasional distant metastasis. 2 They may need special investigations (computed tomography, magnetic resonance angiography or even biopsy) and may require surgical resection. They may present along with or be misdiagnosed as DVT. 3–5 In one series, Benns et al. 6 demonstrated that 0.11% of patients with soft-tissue sarcoma presented with DVT. In unusual circumstances, as in our case, they may present along with DVT and thus distract the attention of the treating physician from other possibilities. Vascular technologists and physicians should consider soft-tissue sarcomas whilst evaluating patients with leg swelling, especially in those that present with atypical signs or symptoms and demonstrate an inadequate response to initial therapy. If a mass is identified, the management must include surgical treatment followed by anticoagulation and appropriate compression therapy to prevent postphlebitic syndrome.
Conflict of interests and funding
Dr R Kolluri is the Speaker for GSK, Sanofi-Aventis and The Medicines Company, and Consultant for Sanofi-Aventis. None for Dr N K Singh.