
Abstract
Objectives
Early success treating incompetent perforator veins (IPVs) with radiofrequency ablation (RFA) and the trend to move varicose vein surgery into a walk-in walk-out service led to the design of a specific device enabling RFA of IPVs using local anaesthesia (ClosureRFS™ stylet). Our aim was to assess one-year outcomes of a clinical series of patients undergoing treatment with this device. Truncal reflux, where present, was treated initially, and RFA of IPVs was performed as a secondary procedure.
Method
Duplex ultrasound examinations were performed and the presence of IPVs documented. Results were compared with preoperative scans. IPVs were classified as closed, not closed/reopened or de novo.
Results
Of the 75 patients invited for follow-up, 53 attended at a median time of 14 months (range 11–25). Sixty-seven limbs were analysed (M:F 1:2.1, median age 62, range 25–81). Of the 124 treated IPVs, 101 were closed (82%). Clinical, aetiological, anatomical and pathological clinical score was improved in 49.3% limbs. IPV closure was reduced in patients with recurrent varicose veins compared with primary varicose veins (72.3% versus 87%, P = 0.056).
Conclusion
These results demonstrate the radiofrequency stylet device to be an effective treatment for IPVs.
Introduction
The importance of incompetent perforator veins (IPVs) in the pathogenesis of chronic venous insufficiency has long been recognized since classic studies by Linton 2 and Cockett 3 ; yet their treatment remains controversial. There appears to be a particular association with recurrent varicose veins, with studies demonstrating that IPVs are more common in patients with recurrent varicose veins and with larger numbers present in these patients. 4,5 Numerous authors have noted clinical benefits of treatment. 6,7
Subfascial endoscopic perforator surgery (SEPS) was developed by Hauer 8 in 1985 in light of high complication rates after open surgery for IPVs. Success rates of 78% at three years have been reported. 9 With the advent of minimally invasive ‘office-based’ procedures for varicose veins, new technical developments have enabled the treatment of IPVs in this setting.
Recently, we reported an 81% closure rate for TRansluminal Occlusion of Perforator (TRLOP), a technique that uses radiofrequency ablation (RFA) to treat IPVs under general anaesthesia, at five years. 10 The early success of this technique led to the design of a purpose-built stylet for the procedure. The aim of this study was to assess the one-year outcomes of patients undergoing treatment using this new device. We believe this is the first published study of treatment outcomes.
Method
All patients who underwent treatment using the new device during the first year of its use in the unit (a private specialist vein unit) were included in this study. During this time period all patients with proven IPVs underwent treatment with the radiofrequency stylet (RFS) device (ClosureRFS™ VNUS® Closure®, VNUS Medical Technologies Inc., San José, CA, USA) using local anaesthesia, unless they underwent treatment with general anaesthesia out of personal choice. Those patients who underwent treatment with the new device under LA in the defined period were identified from the unit database and theatre records and recalled for assessment. Initial contact was by letter, inviting patients to attend for assessment, followed by contacting by telephone those who did not initially respond.
Prior to surgery, all patients had duplex ultrasound (DUS) scans (SONOLINE Antares™, Siemens) of lower limbs performed preoperatively by experienced vascular technologists according to a previously described protocol. 11 As part of this protocol, the presence of any IPVs was sought and site recorded according to a set of coordinates: perpendicular distance to anterior tibial spine and vertical distance from the most prominent point of the malleolus (lateral or medial) to the level of the IPV in the calf, or to the midline and superior border of the patella in the thigh. Augmentation of flow in perforators was assessed with manual compression of the foot and/or leg. Perforator incompetence was considered to be present if any outward flow was present as visualized with colour flow, and if doubtful, confirmed with spectral Doppler trace. All IPVs were treated, regardless of diameter. Clinical, aetiological, anatomical and pathological (CEAP) classification was also recorded prospectively for all limbs. We treated all IPVs routinely as part of the primary treatment plan for varicose veins, regardless of clinical severity score or symptoms, and in patients with both primary and recurrent varicose veins.
It is our practice to perform treatment of truncal reflux, where present, as the initial procedure, and RFA of IPVs as a secondary procedure after an interval of approximately one week. Superficial varicosities were treated concomitantly or at a later date. In all cases, RFA of IPVs was performed in the awake, non-sedated patient using tumescent local anaesthesia by one of the three surgeons. IPVs were re-identified with the aid of recorded coordinates using intraoperative DUS scanning (Acuson Cypress™, Siemens, Issaquah, USA) with a 7.0 MHz probe (Acuson Cypress™) in the supine position, enabling a longitudinal view of the entire IPV and its confluence with the deep venous system. We did not routinely reassess competence of IPVs at this stage after treatment of truncal reflux.
Skin infiltration was performed with 1% lidocaine. Under DUS-guidance, a 12-gauge cannula (Intraflon 2, Ecouen, France) was introduced percutaneously and advanced into the IPV to the subfascial level, followed by removal of the needle trocar, confirmatory flashback of venous blood and deployment of a rigid 6 Fr RFS device. The device was advanced into place below the fascial level, maintaining as much distance from the deep vein system as practicable (at least 4 mm, in order to avoid energy transfer to the deep system). Further undiluted local anaesthetic was then infiltrated around the IPV itself. The patient was then placed in the reverse Trendelenburg position and the site re-checked with DUS. Direct manual pressure was then applied to the skin overlying the IPV, to improve contact between catheter electrodes and IPV wall. Radiofrequency energy was then delivered to the vein wall (RFGPLUS™ VNUS Medical Technologies Inc., San José, CA); a temperature of 85°C was generated for one minute. Appearances were then visualized by intraoperative DUS; if unsatisfactory, repeat attempts were made to obtain closure of the IPV, up to a maximum of three treatments.
All patients received a single oral dose of co-amoxiclav (625 mg, GlaxoSmithKline, Uxbridge, UK) or alternative if penicillin-allergic preoperatively. Low-molecular-weight heparin (4000 iu enoxaparin sodium, Sanofi-Aventis, Guildford, UK) was given postoperatively only to those patients thought to be at high risk for venous thromboembolism and not already receiving anticoagulants. After the procedure, all patients were given 20–30 mmHg graduated compression stockings (Venosan®, Saltzman, Switzerland) to wear 24 hours a day for at least three days. Postoperatively, repeat DUS was not performed unless patients were symptomatic. Patients were reviewed in the outpatient clinic 6–8 weeks after finishing their full course of treatment. All details of postoperative complications were prospectively collected and entered into the unit database.
At review, CEAP clinical status, patient- and observer-reported recurrence and patient-reported complications were recorded. DUS examinations (Acuson Sequoia 512, Siemens) were performed by experienced vascular technologists and IPVs designated as closed, not closed or de novo according to a protocol we have previously described. 10 IPVs present on the preoperative scan that were not treated were noted. Patient notes and the unit database were reviewed for the presence of complications and any other procedures performed in the intervening period.
Statistical analysis
Statistical analysis was analysed using Interstat 3 and Prism software (GraphPad Software, Inc., San Diego, CA, USA). Intergroup comparisons were made with the Student's t-test (TT) or Mann-Whitney U test, as appropriate for parametric and non-parametric data. Univariate analysis was performed to estimate the effect of selected risk factors using Fisher's exact test. The estimated effect of the risk factors is presented in terms of the odds ratio (OR), its 95% confidence interval (CI) and P value. A P value of ≤0.05 was considered statistically significant.
Results
Of the 75 patients invited to attend, 53 participated (71%). One patient was excluded from the analysis as they had not completed their course of treatment. Patient characteristics, presenting complaint, CEAP clinical severity score and limb characteristics are described. The median time to review was 14 months (range 11–25, Tables 1 and 2). Although patients with previous deep vein thrombosis (DVT) were not excluded in this study, all deep venous systems were normal on DUS.
Patient and limb characteristics and presenting complaint

EVLA, endovenous laser ablation
CEAP clinical score at presentation and one year for each limb and IPV
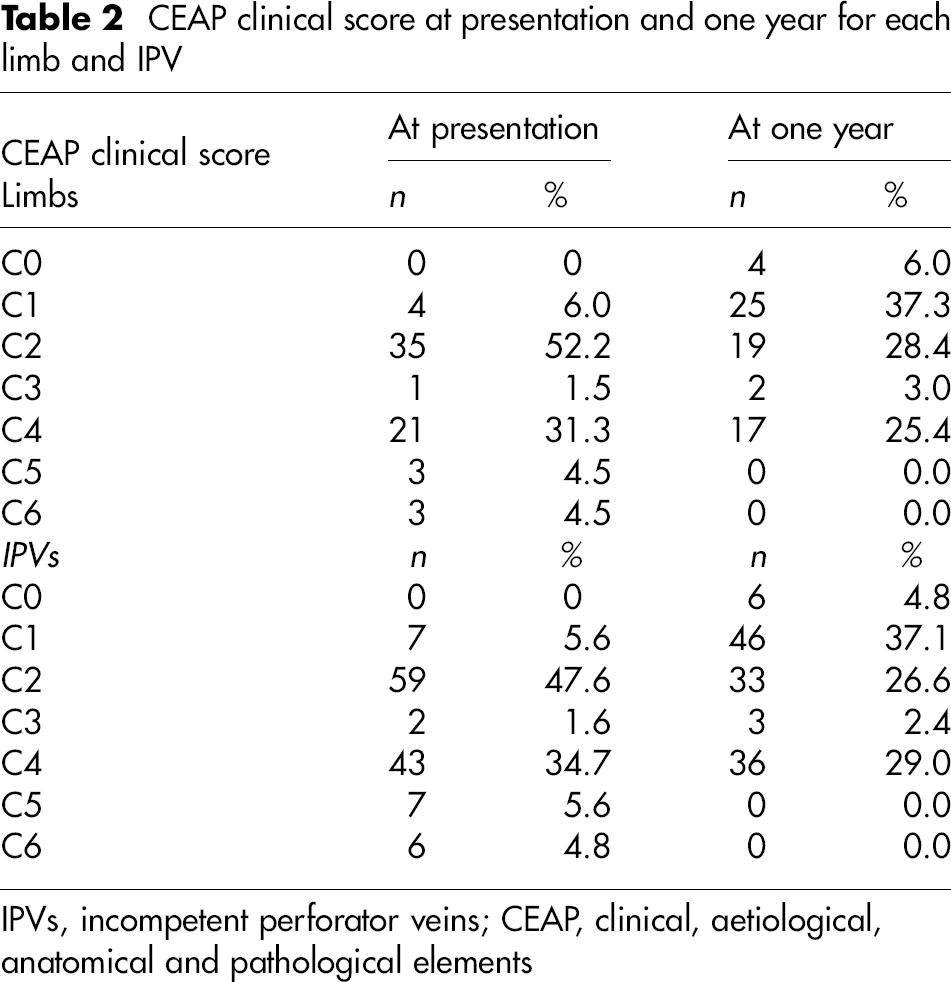
IPVs, incompetent perforator veins; CEAP, clinical, aetiological, anatomical and pathological elements
Of the 151 IPVs identified on preoperative DUS, 124 were treated with the RFS device. At review, 101 IPVs were closed (82%) and 23 were not closed or reopened (18%) in 19 limbs (28%) in 16 patients (30%). Of the 101 closed IPVs, 19.2% were identified on DUS with a characteristic sonographic appearance. A further 22 de novo IPVs were identified in 16 limbs (23%) in 16 patients (30%). Of the 27 IPVs not treated, at intraoperative DUS, five were identified as closed after thermoablation of truncal reflux, 19 were no longer identified and three were ligated due to surgeon preference. The 19 IPVs not identified occurred in 12 limbs in which nine had undergone prior thermoablation of truncal reflux. Ten of the 19 were lateral calf IPVs (Figure 1).
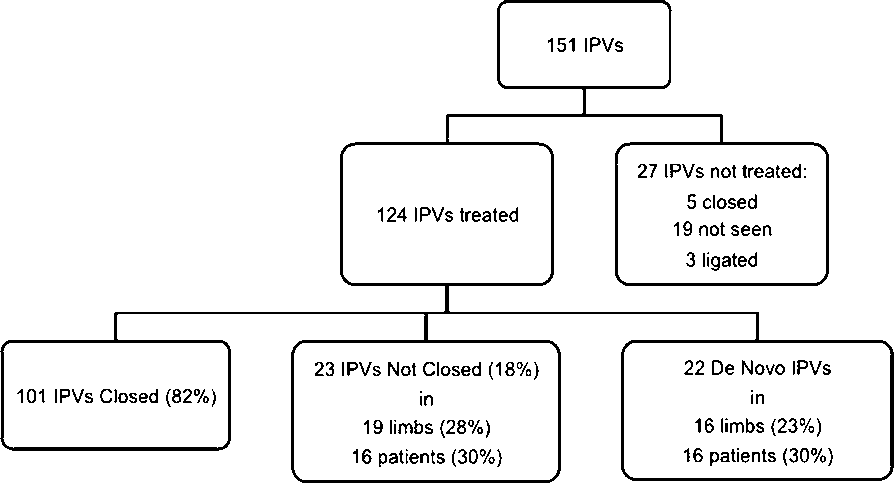
Fate of incompetent perforator veins
In one limb in which four IPVs were present initially, two were seen to be closed after treatment of great saphenous vein reflux and two were treated. At follow-up, two IPVs were present. It was not possible to identify accurately whether these were the former IPVs or those that were treated. Both were attributed to failure of IPV closure. Similarly, in another patient, an IPV seen at follow-up was seen to be a double IPV where one element was closed and the other not closed. This was noted as a treatment failure.
In 33 limbs (49.3%), CEAP clinical score was improved. It was unchanged in 30 limbs (44.8%) and worse in four (6.0%). Of the 27 limbs in CEAP C4–6 (40.1%), 15 (55.6) demonstrated an improved clinical score with 12 (44.4%) unchanged. Of the three patients with active ulceration at the time of treatment, all ulcers had healed at follow-up. Of the 19 limbs in which IPVs were not closed, recurrent varicose veins were noted by patients in six limbs and by observers in 12. In these limbs CEAP score was unchanged in 10, worse in three and improved in six (Table 2).
There was no difference seen for the initial CEAP clinical score for those IPVs closed and not closed (median 2.0 versus 2.0, P = 0.811, Mann-Whitney U test). However, in those limbs in which IPVs were not closed, patients were more likely to be older compared with those in which IPVs were closed, although not statistically significant (median 65 versus 59 years, P = 0.0773, TT). In those limbs in which IPVs were not closed, observed reduction in CEAP clinical score was significantly less than in those in which IPVs were closed (median 0 versus 1.0, P = 0.0333, Mann-Whitney U test, Figure 2).

Age, initial C (CEAP) score, change in C (CEAP) score and incompetent perforator vein closure
IPVs were more likely to be not closed or reopened in patients with recurrent compared with primary varicose veins (27.6 not closed or reopened versus 13.3%) though not significant (P = 0.056, OR = 2.56, 95% CI = 1.02–6.44), Fisher's exact test). De novo IPVs were significantly more common in limbs with recurrent varicose veins compared with primary varicosities (63.6% versus 17.8%, P = 0.0003, OR = 8.1, 95% CI = 2.54–25.7, Fisher's exact test). There was no difference in the proportion of closed and not closed IPVs in limbs having undergone prior endovenous laser ablation (EVLA) and no prior EVLA (OR = 1.20, 95% CI = 0.430–3.33, Fisher's exact test) or in limbs where concomitant procedures were and were not carried out (OR = 0.52, 95% CI = 0.24–1.12, P = 0.129, Table 3).
Evaluation of possible risk factors for failure of IPV closure (Fisher's exact test)
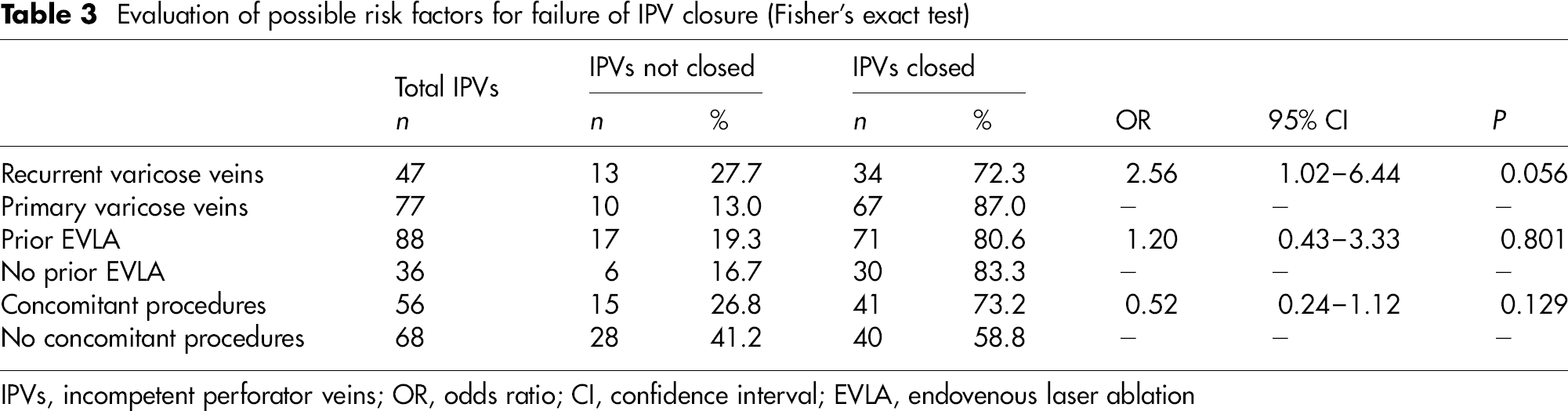
IPVs, incompetent perforator veins; OR, odds ratio; CI, confidence interval; EVLA, endovenous laser ablation
Complications
Prospectively documented complications included one DVT, one neuropraxia, one episode of phlebitis, one cellulitis and one chemical ulcer. The DVT (posterior tibial vein thrombus) occurred in a patient two weeks after foam sclerotherapy administered four weeks after RFS treatment. The chemical ulcer occurred after subsequent microsclerotherapy. There were no skin burns or arteriovenous fistulae in this series. Patients reported a further seven neuropraxias (total of 8, 12% of limbs), one restless legs and five skin staining (all of whom received concomitant or subsequent duplex-guided foam sclerotherapy) at one-year review.
These results incorporate one patient who had further treatment of an IPV in the period between initial procedure and this study. This was a denovo IPV treated six months after the initial procedure. At this time the original IPV was closed, as were both IPVs at one year. The de novo IPV has not been included in the results. No other patients had further treatment of IPVs.
Discussion
In this study, 82% IPVs remained closed at one year. This compares favourably with 79% in another study of RFA of IPV using the TRLOP technique at one year, although less favourable than SEPS at one year (92%) and 78% at three years. 9,11,12 Other treatment options include laser ablation, foam sclerotherapy and cryosurgery, though as yet no long-term results are available. 13–15 Complication rates were low in this study but there is a significant incidence of neuropraxia (12%) that should inform the consent process.
Participation in this study was high despite the fact that enrolment was not prospective although overall numbers are small. We used a significant sized area to define the original IPV site, making it less likely that any IPVs that were not closed or reopened were misclassified as de novo according to a method we have previously described. 10 Despite the strict classification system used, success rates were acceptable.
None of the not closed or reopened IPVs in this study displayed evidence of neovascularization and thus all were attributed to treatment failure consistent with our previous findings with the TRLOP technique. 10 De novo IPVs were seen in 23% of limbs, a figure similar to our observations of RFA of IPVs in a previous study. We feel this further supports the use of a minimally invasive method of IPV treatment in light of higher rates (75.8%) reported by others using more invasive methods. 16
Although this study took place in a private institution, a significant proportion of limbs were in CEAP clinical classes 4–6. Despite the fact that improved score was seen in a more than half of these limbs, this may not be reflective of other minor degrees of improvement within the CEAP class (e.g. severe lipodermatosclerosis and eczema progressing to residual pigmentation at follow-up, all within C4) and thus underestimate clinical benefit.
Surprisingly, initial CEAP score was not found to be a risk factor for failure of IPV to close. Increasing age and the presence of recurrent varicose veins are likely to be risk factors although neither of these effects was statistically significant in this sample. This deleterious effect of recurrent varicose veins on IPV closure has been noted by others after SEPS. 17 Interestingly, failure of IPV closure was present in three out of the four limbs in which CEAP clinical score deteriorated and observed closure of IPV correlated with reduction in CEAP score. It should be noted that we have employed simple univariate analyses in this small sample group to observe such trends.
This study solely examined clinical and DUS outcomes of RFA of IPVs. We have been able to correlate anatomical outcomes with clinical outcomes by means of the CEAP clinical score although optimally, the study would also include pre- and postoperative patient questionnaires to assess venous clinical severity scores or similar such parameters for which other investigators have demonstrated improvements with SEPS. 9 It was noted by vascular technologists that some of the IPVs that had not closed or reopened were of a large calibre. The diameter of IPVs was not measured preoperatively, so we are unable to make a firm comment to whether this has any effect on treatment efficacy. Ideally, we would include this measurement in any future studies. Similarly, future study would include a prospective record of ablation times to evaluate whether this variable influenced treatment outcome.
As it is difficult to prove a causative association between IPVs and skin changes associated with chronic venous disease, whether to treat IPVs at all remains debated. Worsening of chronic venous disease has been observed with the development of new IPVs; 18 the number of IPVs present has been found to correlate with clinical severity of disease 16 and IPVs are more common in patients with recurrent varicose veins. 4 Nevertheless, other factors are likely to be important. It has been suggested that treatment of truncal superficial venous reflux itself may render treatment of IPVs unnecessary with correction of reflux IPVs occurring after abolition of superficial venous reflux. 19 However, this effect is short lived with the majority of IPVs closed immediately post-high saphenous tie and strip reopened at one year. 11 Interestingly, the IPVs in this study that closed after thermoablation of truncal reflux remained closed at one year. Of those other IPVs not seen at preoperative DUS, these may not have been identified also due to closure after prior thermoablation of truncal reflux. Other possible causes include lack of identification on lower resolution intraoperative DUS or changes in venous physiology in the supine position.
Although the results of this study represent the first patients whom we treated using the RFS device, we do not feel that they are reflective of a learning curve, as we already have had considerable experience with the technique using other catheters. We look forward to the results of the multicentre study that will hopefully demonstrate these results are reproducible.
Footnotes
Acknowledgements
The Whiteley Foundation, registered charity 1099614, provided the funding for Petra Marsh's post. We would like to thank Charmaine Harrison and Craig Smith without whose input this study would not have been possible.