
Abstract
Objectives
Chronic venous insufficiency (CVI) is an important cause of discomfort and inability to work. Hydroxyethylrutosides (Venoruton®; 0-[beta-hydroxyethyl]-rutosides) has been used for decades for the treatment of CVI. Studies have reported symptomatic relief and a decreased capillary filtration after the administration of the oral preparations. Calcium dobesilate is a synthetic venoactive drug acting on several levels. It inhibits capillary permeability; it has antioxidant properties; and it inhibits the synthesis of prostaglandins and thromboxanes, reducing platelet and erythrocyte aggregation, as well as blood viscosity. The aim of this study is to determine whether the combination of both drugs is more effective in decreasing patients' complaints.
Methods
One hundred and fifty patients with primary venous insufficiency were randomized into three groups: Group A receiving calcium dobesilate only, Group B receiving oxerutin only and Group C receiving both calcium dobesilate and oxerutin. Patients were evaluated with a questionnaire before and four weeks after treatment regarding following parameters: itching, fatigue, heaviness, numbness, cramp, swelling and sensitiveness. Patients rated their symptoms from 0 to 4 (0: absent; 1: mild; 2: moderate; 3: severe; 4: very severe).
Results
Complaints, which were scored by patients before and after treatment, decreased. Among the single-drug groups, itching score decreased more in Group B, whereas scores of fatigue, heaviness, numbness, cramp and swelling decreased more in Group A. But the difference was not significant, statistically. But all complaints decreased significantly in Group C. Difference of scores after treatment revealed no statistical significance in Group A and B, but scores of Group C produced a significant difference when compared with Group A and B.
Conclusion
Results demonstrate that a combination of calcium dobesilate and oxerutin shows a better improvement of complaints. These observations have to be confirmed in larger series with objective tests. Changes of quality of life after a combination therapy might also be of interest.
Introduction
Chronic venous insufficiency (CVI) is a condition in which veins are unable to transport blood unidirectionally toward the heart with a flow adapted to tissue drainage needs, temperature regulation and haemodynamic reserve, regardless of their position and activity. CVI first manifests as an increase in venous hypertension with or without reflux. 1 CVI is an important cause of discomfort and inability to work and many people find it difficult to live with this condition. Its prevalence has not been clearly determined because there are few available studies on the subject and those that are available present limitations. Some studies do not cover the whole pathological spectrum and focus only on varicose veins or ulcers, while others do not use standardized definitions of the illness and use a variety of different diagnostic criteria. 2 As a result, prevalence has been estimated between 1% and 50%. 3,4 The Framingham Study shows an annual incidence of 2.6% among women and 1.9% among men. 5 The causes of CVI are unknown, although it has been associated with venous dilation and deformity and valvular venous incompetence. Trophic skin disorders and venous ulcers result from severe varicose illness. 6 Clinical manifestations of CVI differ depending on the stage of the illness and can include feelings of heaviness in the extremities, paraesthesia (tingling), cramps, pain, oedema (swellings), varicose veins, skin pigmentation, varicose sores and signs of skin atrophy (wasting). Since 1994, an International Consensus has been used to define and classify CVI in a standardized fashion. 7 According to this Consensus, the clinical signs (C), aetiology (E), anatomical distribution (A) and pathophysiological conditions (P) classify CVI. Surgery, sclerotherapy and mechanical compression are generally the preferred treatments. However, pharmacological treatments or phlebotonics are often used because they are easy to administer and there is poor compliance with compressive treatments (such as elastic stockings). Phlebotonics are associated with effects on macrocirculation, e.g. they may improve venous tone, 8 and on microcirculatory parameters, e.g. decrease capillary hyperpermeability. 9 There are doubts about the clinical efficacy and safety of phlebotonics. Some case-controlled studies have shown an associated risk of agranulocytosis of some phlebotonics. 10
Hydroxyethylrutosides (HR) (Venoruton®; 0-[beta-hydroxyethyl]-rutosides) has been used for decades for the treatment of CVI and signs/symptoms associated with varicose veins and deep venous disease. Several studies have reported symptomatic relief and a decreased capillary filtration after the administration of the oral preparations. 11–18 In many studies, experimental settings and clinical reports, the efficacy of HR could be shown even in a short time after the beginning of therapy. 11,12,19
Calcium dobesilate is a synthetic venoactive drug acting on several levels. 20 Among others, it inhibits capillary permeability induced by serotonin, bradykinin and histamine; 21 it has antioxidant properties; 22 and it inhibits the synthesis of prostaglandins and thromboxanes, reducing platelet and erythrocyte aggregation, as well as blood viscosity. 23,24 In animal models, calcium dobesilate reduces experimental lymphoedema 25 and intralymphatic pressure, 26 increases lymphatic flow, 27 and decreases angiogenesis, 28 carboxymethyl-lysine-advanced glycation end product formation and vascular endothelial cell growth factor over-expression, as well as albumin leakage. 29
Here in our clinic, it has been observed that the relief of subjective symptoms related to venous insufficiency was better with a combination of both drugs. The aim of this study is to determine whether the combination of both drugs is more effective in decreasing patients' complaints.
Methods
This study was a single-blind trial where 150 patients with primary venous insufficiency were randomized into three groups: Group A receiving calcium dobesilate only, Group B receiving oxerutin only and Group C receiving both calcium dobesilate and oxerutin. All patients were advised to use compression stockings. Patients were evaluated with a questionnaire before and four weeks after treatment regarding the following parameters: itching, fatigue, heaviness, numbness, cramp, swelling and sensitiveness. Calcium dobesilate as well as oxerutin were administered 1000 mg t.i.d. Patients rated their symptoms from 0 to 4 (0: absent; 1: mild; 2: moderate; 3: severe; 4: very severe). The circumference of legs was measured at two levels (10 cm below the lower margin of the patella and 5 cm above the malleoli). Venous ulcer diameters were measured if present. Age, sex, body mass index, waist-to-hip ratio, smoking habit, history of hemoptysia and/or dysponea, and the presence of pigmentation were also recorded. Whole blood count as well as renal and hepatic function tests were performed.
Statistical analysis
All data were reviewed prospectively. Data are expressed as mean ± SD. Descriptive statistical analysis was performed for demographic data and analysis of variance test (Fisher's PLSD) was performed to analyse the differences between the three groups using StatView statistical software package 5.0.1 (SAS Institute, Inc, Cary, NC).
Results
Demographic data revealed no statistical difference. Mean age was 47.6 ± 12.9 in Group A, 46.7 ± 13.5 in Group B and 48.1 ± 12.3 in Group C. A summary of demographic data is demonstrated in Table 1. Data regarding whole blood count, renal and hepatic function tests before treatment and four weeks after treatment are demonstrated in Table 2. None of the parameters revealed statistically significant difference (P > 0.05), except aspartate aminotransferase (AST) and blood urea nitrogen (BUN) in Group B. BUN decreased slightly which is clinically not important. AST increased from 35.0 ± 9.4 to 36.9 ± 9.3, which is statistically significant but clinically not, because even increased values are in the normal range.
Demographic data
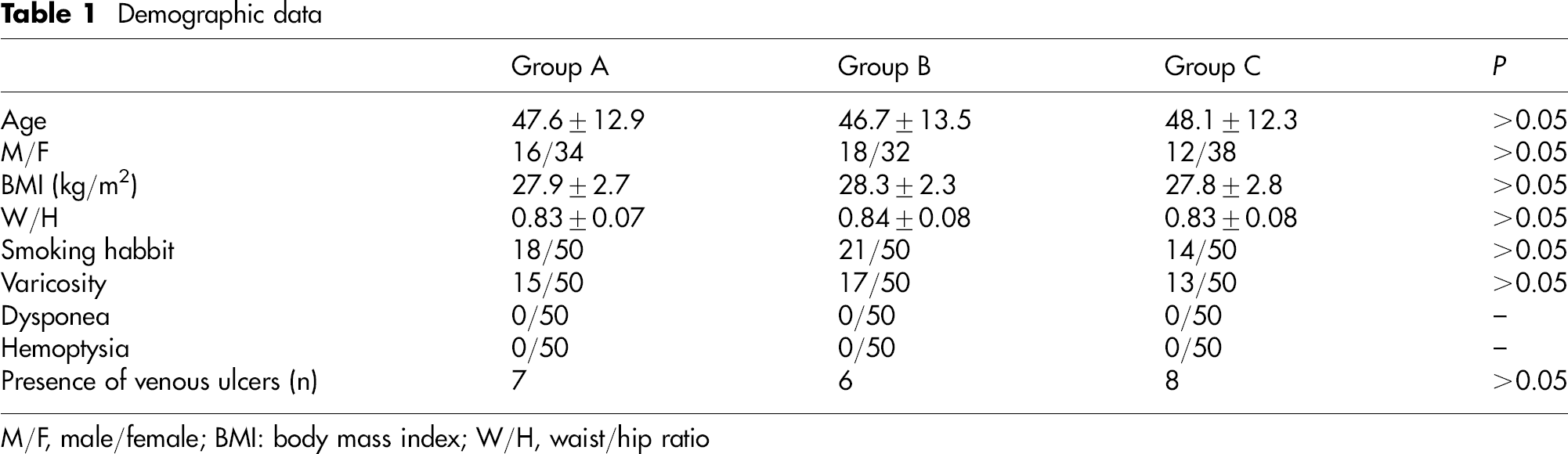
M/F, male/female; BMI: body mass index; W/H, waist/hip ratio
Blood parameters before and after treatment
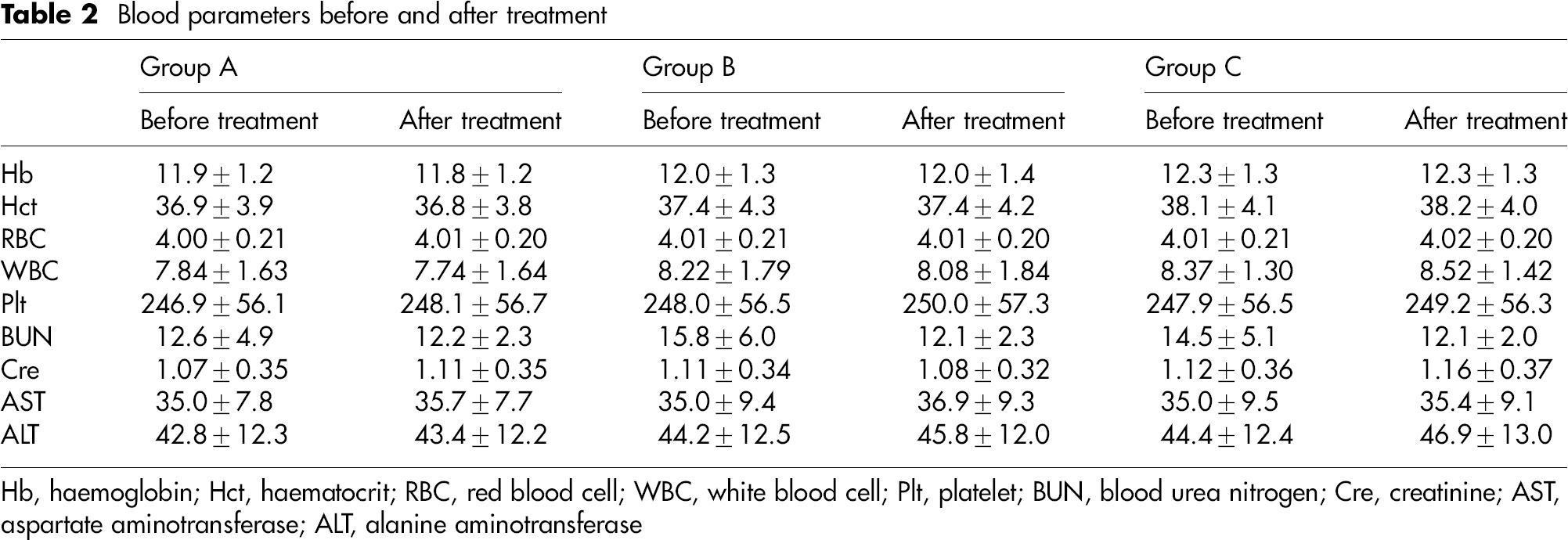
Hb, haemoglobin; Hct, haematocrit; RBC, red blood cell; WBC, white blood cell; Plt, platelet; BUN, blood urea nitrogen; Cre, creatinine; AST, aspartate aminotransferase; ALT, alanine aminotransferase
Venous ulcers were present in seven patients of Group A and ulcer diameter reduced from 4.1±0.6 cm to 3.4±0.7 cm. Ulcer diameter reduced from 4.1 ± 0.9 to 3.5 ± 0.5 in Group B (6 patients) and from 4.2 ± 0.7 to 2.8 ± 0.3 in Group C (8 patients).
The ratio of patients who used compression stockings were low: 13 (26%) patients in Group A, 15 (30%) patients in Group B and 16 (32%) patients in Group C. Overall use of compression stockings was 29.3%.
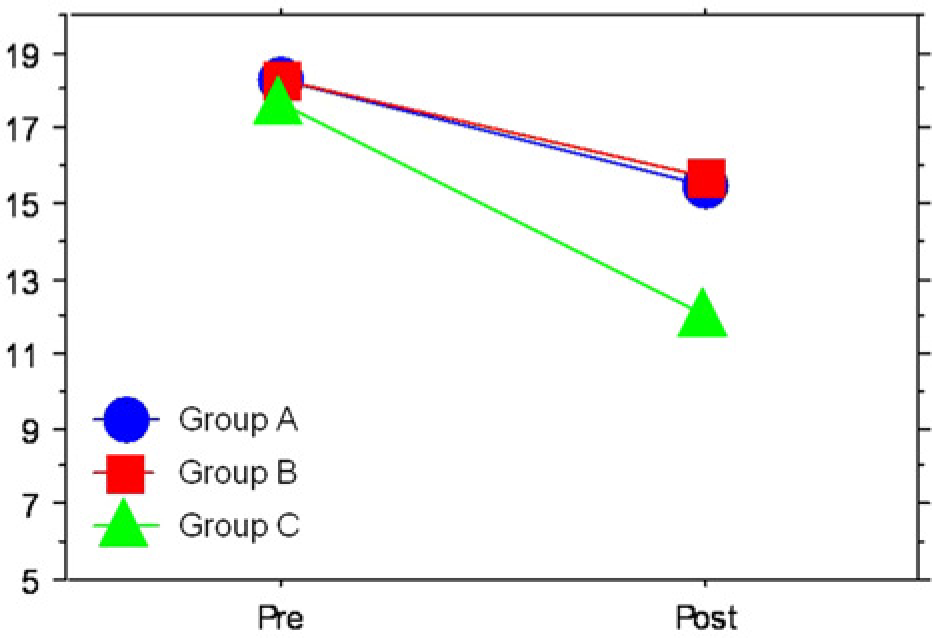
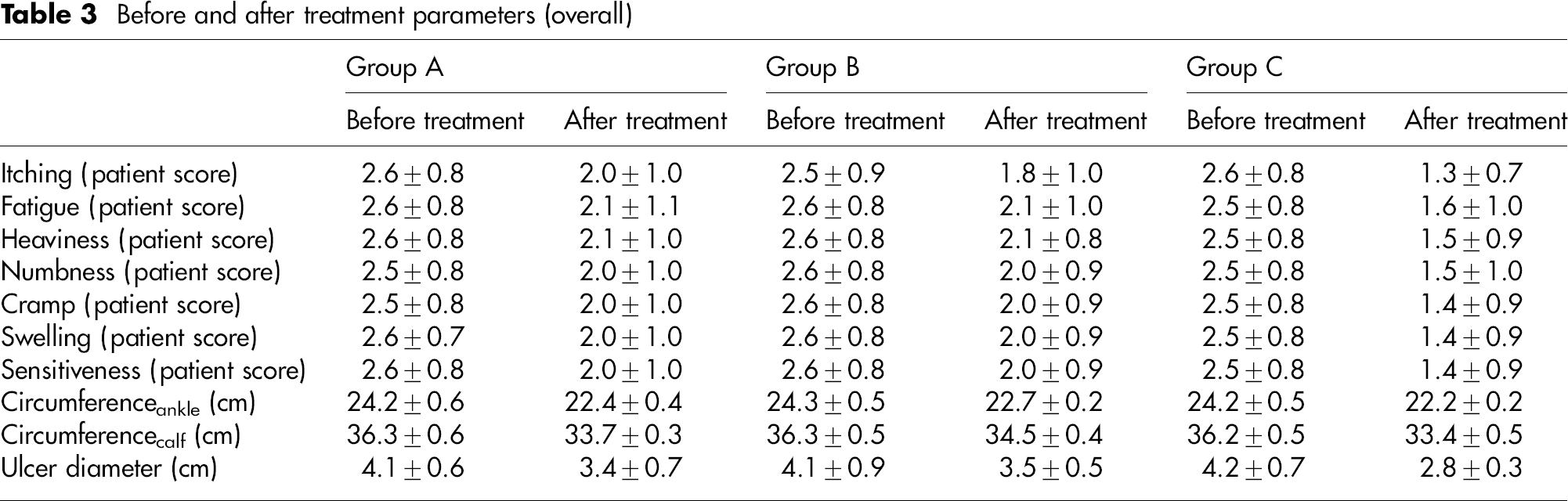
Complaints (subjective parameters) (Figure 1), which were scored by patients before and after treatment, decreased (Table 3). Among the single-drug groups (Group A and Group B), itching score decreased more in Group B, whereas scores of fatigue, heaviness, numbness, cramp and swelling decreased more in Group A. But the difference was not statistically significant. However all complaints decreased significantly in Group C. Scores were similar in all groups before treatment (P > 0.05). Difference of scores after treatment revealed no statistical significance in Groups A and B, but scores of Group C produced a significant difference when compared with Groups A and B (P < 0.05). This was an analysis of overall patients with and without the use of compression stockings. Scores in subgroups with patients using compression stockings (A1, B1 and C1) decreased more when compared with patients not using compression stockings (A2, B2 and C2) (P < 0.05), but decrease of scores in Group A2, B2 and C2 also produced statistical significance (P < 0.05) when compared with starting point. The difference between A1 and B1 as well as between A2 and B2 was not significant (P > 0.05). Finally, the decrease of scores was highest in patients receiving combination therapy together with using compression stockings. The sum of scores, which may indicate patients' complaints in total, decreased most in combination therapy together with compression stockings. Details are demonstrated in Table 4 and Figures 2 and 3.

Graphical demonstration of subjective parameters in sums (blue: calcium dobesilate; red: oxerutin; green: combination of calcium dobesilate and oxerutin). Colour version available online

Graphical demonstration of subjective parameters in sums, subgroup with compression stockings (blue: calcium dobesilate; red: oxerutin; green: combination of calcium dobesilate and oxerutin). Colour version available online
Graphical demonstration of subjective parameters in sums, subgroup without compression stockings (blue: calcium dobesilate; red: oxerutin; green: combination of calcium dobesilate and oxerutin). Colour version available online
Before and after treatment parameters (overall)
Sum of subjective parameters before and after treatment

The circumference at the level of ankles decreased from 24.2±0.6 to 22.4±0.4 in Group A, from 22.4±0.4 to 22.7±0.2 in Group B and from 24.2±0.5 to 22.2±0.2 in Group C. Similarly, the circumference at the level of calfs decreased from 36.3±0.6 to 33.7±0.3 in Group A, from 36.3±0.5 to 34.5±0.4 in Group B and from 36.2±0.5 to 33.4±0.5 in Group C. The decrease of circumference was better in the presence of compression stockings in Group A and Group C when compared with Group B (P < 0.05), but there was no difference between Groups A and C (P > 0.05). The highest decrease in circumference is in Group C together with the use of compression stockings (P < 0.05). Results are demonstrated in Table 5. None of the patients had adverse effects like fever, gastrointestinal disorders or skin reactions.
Circumference of legs before and after treatment split by compression stocking use

Discussion
Patients in this study group experienced an improvement after treatment. Studies confirm the efficacy of calcium dobesilate as well as oxerutin. 30–32 Adverse effects like fever, gastrointestinal disorders, skin reactions and agranulocytosis are associated with the use of calcium dobesilate 33 but none of them were observed in our series.
Martínez-Zapata et al. demonstrated an improvement in the quality of life of calcium dobesilate versus placebo. This difference was significant at 12 months but not at three months (primary outcome), statistically. 31 This may indicate that single therapy with calcium dobesilate should be supported with others to achieve more improvement.
Oxerutin has been shown to have a high degree of safety and to be particularly active on oedema, swelling, and signs and symptoms of CVI. 32,34–36
Although all patients were advised to use compression stockings, patients feel uncomfortable with compression stockings, which might be due to climatic conditions.
Studies have demonstrated that the circumference of legs decreased after a four-week period of treatment with calcium dobesilate or with oxerutin, 37,38 similar to the present study. But the best decrease of circumference was achieved in the subgroup with combination therapy together with using compression stockings.
The goal of this study was to evaluate patients' comfort or discomfort after medical therapy; therefore, it seemed to be more suitable to use a simple but subjective test instead of validated tests.
In conclusion, although this study has limitations like being based predominantly on subjective criteria and having no placebo control, results demonstrate that a combination of calcium dobesilate and oxerutin show a better improvement of complaints, especially when used together with compression stockings. These observations have to be confirmed in larger series with objective tests (e.g. pletysmography, Doppler ultrasound). Changes of quality of life after a combination therapy might also be of interest.