
Abstract
Background
A too high resting pressure of compression devices is poorly tolerated and may cause skin defects, especially in patients with concomitant arterial occlusive disease.
Aim
To investigate whether low compression pressure will improve venous pumping function in patients with venous incompetence.
Material and methods
Venous pumping function was assessed in 20 patients with severe reflux in the great saphenous vein by measuring ejection fraction (EF) using strain-gauge plethysmography. Measurements were repeated after application of knee-high medical compression stockings and of inelastic bandages applied with a pressure of 20, 40 and 60 mmHg in the supine position.
Results
EF was significantly reduced compared with healthy controls. Compression stockings exerting a median pressure of 27 mmHg (interquartile range [IQR] 25–29) in the supine and 30.5 mmHg (IQR 28.25–34.25) in the standing position produced a moderate, non-significant improvement of EF of 17%. Inelastic bandages with a resting pressure of 20.5 mmHg (IQR 20–22) in the supine position resulting in a standing pressure of 36 mmHg (IQR 33–40.75) led to a significant increase of EF of 61.5% (P < 0.01). A further increase of the resting pressure to 40 and 60 mmHg achieved an increase of the EF of 91% and 98%, respectively (P < 0.001).
Conclusions
In patients with venous pumping failure, inelastic bandages produce a significant pressure-dependent increase of EF. A significant improvement in venous pumping function was achieved with inelastic bandages even at a resting pressure of 20 mmHg.
Keywords
Introduction
In a previous study we were able to demonstrate that inelastic compression bandages are haemodynamically more effective compared with elastic bandages applied with the same resting pressure and able to normalize the ejection fraction (EF) in patients with venous insufficiency when applied with high pressure. 1
Sometimes high resting pressure is not well tolerated by the patients and may even cause damage, especially in patients with mixed arterial-venous disease. For those cases a reduced initial pressure may be desired. Such reduced pressure may be sufficient to impede oedema or to increase venous blood flow velocity in the lying position 2,3 but it is not clear if it is still haemodynamically effective during daily activity. This question is also relevant when a correctly applied bandage is worn for several days. The effectiveness of such bandages may be doubtful because of the pressure drop, which is more pronounced with inelastic than with elastic bandages. 4
EF, which is a very meaningful parameter characterizing the efficacy of the venous pump, can be measured by different plethysmographic methods. In this investigation we have used a technique which has the advantage that volume changes not of the bandage but of the leg proximal to the bandage are measured. Compared with normal individuals patients with venous incompetence show approximately a halving of EF. 1
The main objective of this experimental study was to investigate whether low-pressure compression devices are able to improve the reduced venous pumping function in patients with venous incompetence.
Material and methods
Twenty patients (10 women, 10 men) aged between 47 and 83 years (mean 61.8 years), in the clinical aetiological, anatomical and pathological elements stage between C2 and C5, were investigated (Table 1).
Clinical characteristics of case report
CEAP, aetiological, anatomical and pathological elements
Inclusion criteria:
Candidates for venous surgery because of massive great saphenous vein (GSV) insufficiency; Incompetent terminal and preterminal valves; GSV diameter at the level of the junction greater than 10 mm and reflux time more than three seconds in the Duplex investigation; Good joint mobility allowing exercises requested by the protocol. Patients who did not fulfil the inclusion criteria or were unable to perform the exercise test described below.
Exclusion criteria:
Patients were informed about the details of the examination and gave their written consent.
Investigations and subsequent surgery were performed in a public hospital.
Duplex investigation of the superficial and deep veins of the lower extremity was performed with the patient in the standing position; the diameter of the GSV at the groin (in a cross-sectional view) and the venous reflux during Valsalva's manoeuvre and after manual compression of the calf were measured, both at the junction of the GSV and 5 cm distally.
Compression devices
The experiments were carried out with and without different compression devices applied in sequential order to all individuals. All experiments on one patient were done on the same day with an interval of 15 minutes between each measurement. The measurements were made five minutes after the bandage application with the patient resting in the supine position in a quiet room with constant humidity and temperature.
Ready-made knee-length compression stockings with a pressure range on the distal leg between 18 and 33 mmHg (Sigvaris 503®, Sigvaris, St Gallen, Switzerland; Gloria 261® Gloriamed, Menaggio, Italy) and inelastic compression bandages were used. As a model for short-stretch (‘inelastic’) material Mollelast® (10 cm wide applied with multiple layers) was applied over Cellona® cotton wool padding with an increasing sub-bandage pressure of 20, 40 and 60 mmHg (Mollelast® and Cellona® are trade marks by Lohmann & Raucher, Regsdorf, Germany). Different pressure levels were achieved by applying the bandages in a more or less tight manner and superimposing more or less layers.
Sub-bandage pressure measurement
The pressure was continuously measured using a newly developed instrument and data were logged by a special computer program (Picopress®, Microlabitalia, Padua, Italy). 5 The pressure transducer consists of a flat plastic pressure probe (diameter 5 cm), which is filled with 2 mL of air for the pressure measurement. Fluctuations of pressure to this probe are transformed into electronic signals (Statham-element) that can be recorded continuously. After measurement the pressure probe is deflated and can be left on the leg for several days. The probe is attached to the B1 point, which is defined by the transition of the muscular part of the medial gastrocnemius into the tendinous part. Sub-bandage pressure is measured in the supine and standing position. Minimal and maximal pressure values during the exercise programme, described below, were also recorded. The difference between standing and resting pressure (‘Static Stiffness Index’, SSI) 6,7 and between maximal and minimal value during exercise (Walking Pressure Amplitude, WPA) was calculated.
Plethysmography
Using strain-gauge plethysmography (Angioflow ® , Microlabitalia, Padua, Italy), below the knee venous volume (VV), expelled volume (EV) and EF were assessed following the method described by Poelkens et al. 8 These authors could demonstrate the haemodynamic effects of pads applied under a plaster bandage on the lower leg in healthy individuals by placing the strain gauge above the proximal end of the plaster.
The indium–gallium alloy gauge (diameter of 1 mm) encircle the leg 5 cm distally from the patella and proximally to the bandage. The methodology has been described in detail in a previous study focusing on the effects of compression material with different elastic properties applied with high pressure in patients with severely disturbed venous pumping function. 1
The investigation starts with elevating the legs in order to empty the veins and the minimal volume of the leg segment proximal to the bandage is registered by the strain gauge. Then the patient stands up and the volume increase of the calf segment, which reflects venous filling, is measured continuously. ‘VV’ is defined as the difference between empty and filled veins. During a standardized exercise (20 steps on a 20 cm high stair in 20 seconds), simulating a walking exercise, the amount of blood that is expelled towards the heart (EV) reflects the quality of the venous pump. The proportion of EV in relation to VV expressed as a percentage is called EF.
In this paper only the values of EF are given.
For comparison the data from a group of 15 healthy controls published in a previous paper are used. 1
Statistics
Median values and interquartile ranges are given.
Repeated-measures one-way analysis of variance and Tukey's post-test were used to compare the repeated measurements of sub-bandage pressure and of EF under different compression systems. Paired data were compared by the Wilcoxon matched pairs non-parametric test. For the comparison of the healthy controls with the baseline data of the investigated patients, the non-parametric Mann-Whitney U test was used. Differences with a P < 0.05 were considered statistically significant.
Results
Sub-bandage pressure
The interface-pressure values measured under the stockings and bandages 12 cm above the inner ankle are summarized in Figure 1. The standing pressure is significantly higher than the supine pressure in every instance (P < 0.001). Inelastic bandages show a much higher pressure increase by standing up than stockings. The resting pressure of an inelastic bandage of 20 mmHg in the lying position increases to nearly double that value when the subject stands up. Inelastic bandages show significantly higher SSI and WPA values compared with elastic stocking even when applied with a pressure of 20 mmHg (P < 0.001) (Figures 2 and 3).

Sub-bandage pressure measured proximally to the inner ankle in lying (L) and standing position (St) under compression stockings and under inelastic bandages applied with a resting pressure of 20, 40 and 60 mmHg. In all instances pressure was significantly higher in the standing than in the lying position (***P < 0.0001). The lying and the standing pressures in each group differed significantly from each other (P < 0.001)
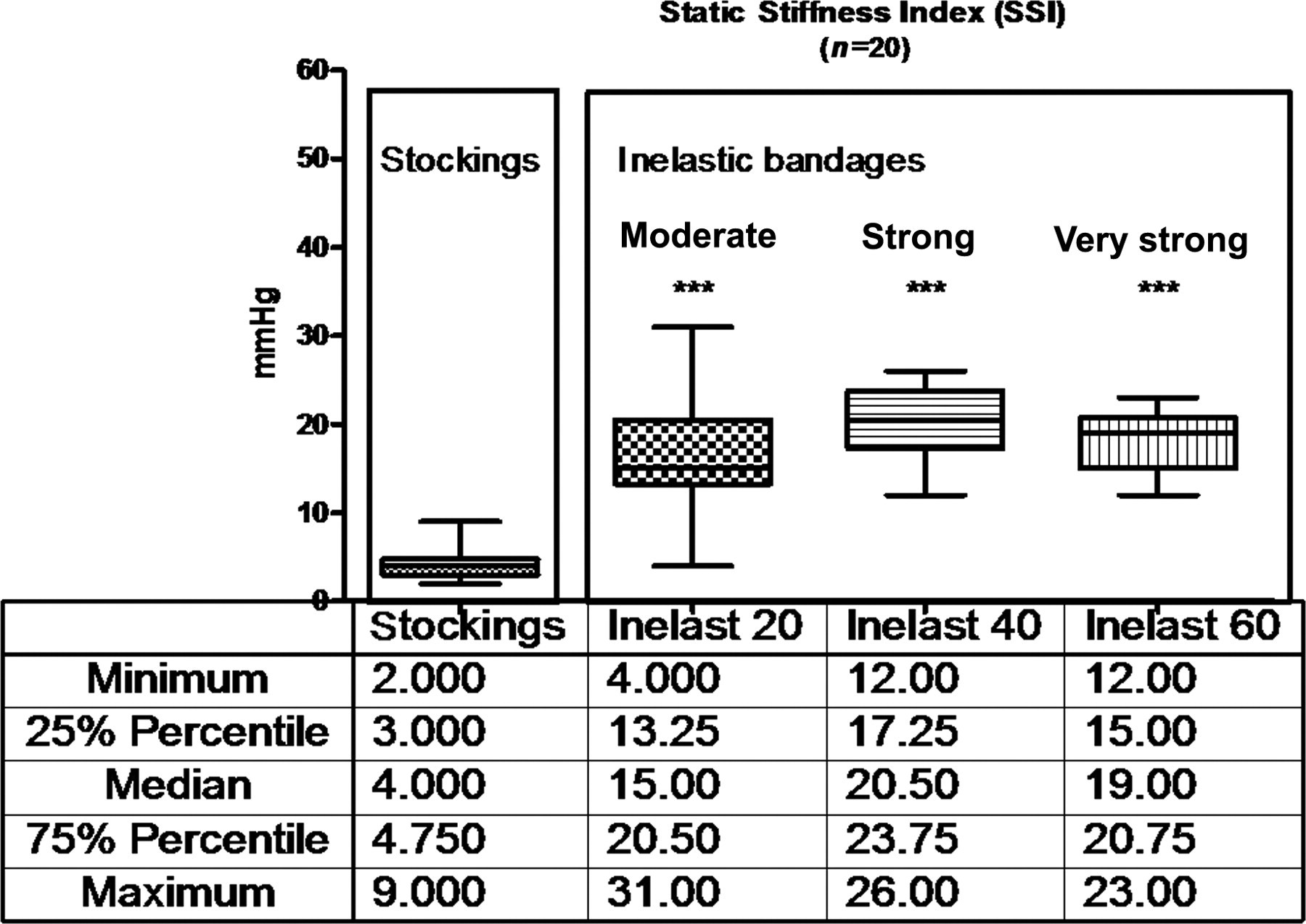
Static Stiffness Index of elastic stockings and inelastic bandages applied with 20, 40, 60 mmHg. SSI is significantly higher with inelastic bandages compared with elastic stocking (P < .001) independently of the pressure at application. There is a significant difference between 20 and 40 mmHg bandages (P < 0.05)
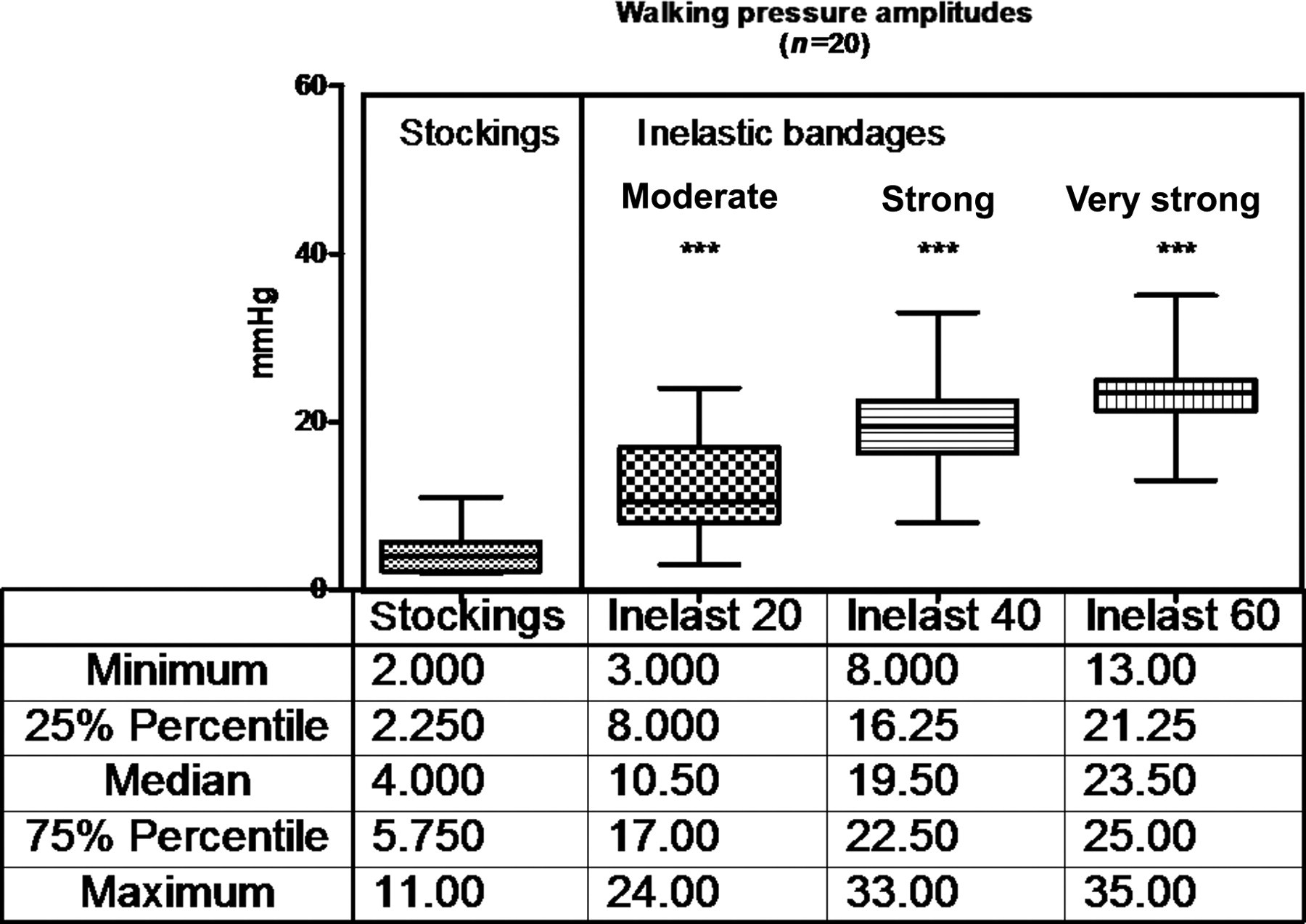
Walking pressure amplitudes of elastic stockings and inelastic bandages applied with 20, 40, 60 mmHg. Amplitudes are significantly higher with inelastic bandages compared with elastic stockings independent from the pressure at application (P < 0.001). Inelastic bandages applied with a pressure in the range of 40 and of 60 mmHg achieve significantly higher walking pressure amplitudes than those with 20 mmHg (P < 0.001)
Ejection fraction
Median values and interquartile ranges of EF measured in 20 legs with venous incompetence were 32.2 mL% (20.9–41.6), which is about half the values found in healthy controls: 65 mL% (63.7–67.8). Compression stockings increase EF by 17% (NS) while inelastic bandages exerting a comparable resting pressure in the lying position improve EF significantly by 61.5% (P < 0.01) (Figure 4).

From left to the right: values of ejection fraction in a healthy control-group, in the group of our 20 patients without compression (‘baseline’), with compression stockings, and with moderate, strong and very strong inelastic bandages. The values of ejection fraction were significantly reduced in the 20 legs with massive venous reflux (‘baseline’) compared to the healthy control group (P < 0.0001). Bandages exerting a supine pressure of only 20 mmHg increased EF significantly (P < 0.001) in contrast to compression stockings in the same pressure range, which did not show a significant difference. Increasing the sub-bandage pressure, a further increase of EF was recorded with inelastic bandages (P < 0.01)
Inelastic bandages applied with a resting pressure of 40 and 60 mmHg result in a further increase of EF of 91% and 98%, respectively (P < 0.001).
Discussion
Up to now the pressure chosen for compression stockings and bandages has been entirely based on experience. In general, it is recommended that the sub-bandage pressure is adjusted to the severity of the underlying disease: strong and very strong bandages for advanced stages of venous and lymphatic disease, and mild and medium pressure devices for the maintenance phase to prevent recurrence of swelling. This regimen is endorsed by some clinical outcome studies performed especially in leg ulcer patients but only by few experimental studies measuring physiological effects of compression as a function of the sub-bandage pressure. 1,9–11 Following a recent consensus recommendation, the chosen bandage pressures were termed as mild, medium, strong and very strong corresponding to pressure levels on the distal lower leg in the lying position of <20, 20–40, 40–60 and >60 mmHg, respectively. 12
Compression pressure has almost never been measured and the elastic property of the material used was assessed based only on the manufacturers' descriptions of the single bandages. Although pressure measurements are not recommended for everyday practice, they are of crucial importance to define the physical properties of compression devices and can be easily performed in different body positions and also during exercise thanks to newly developed pressure sensors working with high precision. 5 By comparing the pressure readings during standing and exercise with those in the lying position, the elastic property and stiffness of the final bandage can be assessed on the individual leg. When leg muscles contract as the subjects stand up or exercise, an inelastic bandage will lead to a higher pressure increase than a yielding, elastic bandage: SSI and WPA will be significantly higher (Figures 2 and 3). 13–15
In a previous study investigating the influence of different compression devices on the venous pumping function, we used strain-gauge plethysmography in order to measure EF by recording volume changes of the uncovered leg. 1 This is not possible using other methods like foot-volumetry 10 or air-plethysmography, 11 which record changes of the bandage and not of the leg by putting plethysmographic devices over the bandage.
In that experiment, 1 which took into consideration not only the pressure but also the elastic property of the bandages, we showed a correlation between standing (and working) pressure, SSI and WPA on one side and an improvement of venous pumping function as reflected by EF on the other side. Stiff, inelastic bandages applied with high pressure were even able to normalize a highly reduced venous pumping efficiency.
However, the question concerning a minimal pressure, which is still able to improve a disturbed venous pumping function, has not yet been answered.
While normal individuals will expel more than 60% of the blood volume from a lower leg segment, the amount of ejected blood will be much less in patients with massive venous reflux. An improvement of EF induced by therapy can be explained by a reduction of venous reflux.
A necessary prerequisite for reflux reduction by compression is the narrowing of refluxing veins in the upright position, which depends mainly on the relationship between the intravenous pressure and the externally applied pressure. 16
Elastic compression stockings exerting a pressure of around 27 mmHg in the lying and 30 mmHg in the standing position are obviously too weak to narrow the veins to an extent where major reflux is impeded.
In contrast, inelastic bandages even when applied with a pressure of 20 mmHg in the lying position may increase the pressure upon standing up to 37 mmHg in average and show much higher WPA compared with elastic stocking. As shown in this study, the high increase of standing pressure, which may go up to 52 mmHg, is associated with a significant improvement of pumping function.
The demonstration that inelastic bandages are haemodynamically effective even when applied with a low pressure of 20 mmHg has mainly two practical implications: one is the well-known pressure loss of inelastic bandages occurring immediately after application, which is the reason for applying such bandages with initially higher pressure. After some days of wearing, the pressure may well drop to a range around 20 mmHg. 4,17
The other practical consequence of our findings is the clinical condition of mixed-arterial-venous disease with a systolic ankle pressure between 70 and 100 mmHg, where low pressure bandages may be indicated. 18
In both situations inelastic bandages exerting a pressure of 20 mmHg, but not elastic stockings even with higher resting pressure, are able to improve venous pumping function.
This finding should not encourage bandagers to apply bandages always in this low-pressure range: higher initial pressure is definitely more effective. Furthermore when an inelastic bandage is applied too loosely, the final pressure after a number of days may decline to nearly zero, because of its pressure loss, resulting in minimal haemodynamic effect.
Practical consequences
A short stretch bandage exerting a pressure of 20 mmHg in the lying position significantly increases EF during walking in patients with venous incompetence.
This finding may have practical importance in patients with mixed arterial-venous disease where reduced bandage pressure is indicated (taking care to reapply the bandage every few days) and in patients wearing strong compression devices for several days when a considerable pressure drop occurs. Based on our findings such bandages should still be haemodynamically effective even if this has to be proved by future studies.
Footnotes
Acknowledgement
The authors gratefully acknowledge the help by Dr Jerry Hutchinson, Convatec GDC, UK, in editing the text. The work was carried out at Clinica M.D. Barbantini, Lucca, Italy.