
Abstract
A rare case is reported of a 47-year-old patient who had residual tumour left in the stump of his left renal vein and inferior vena cava (IVC) after a left nephrectomy for renal cell carcinoma, having previously had a right nephrectomy for a non-malignant disease. He underwent delayed excision of the residual renal tumour after seven months with a prosthetic graft replacement of the IVC. Five years later he developed a graft infection caused by a graft-enteric duodenal fistula. The infected graft was excised and the duodenum closed. The patient has subsequently undergone a successful renal transplantation despite a lack of major venous outflow and remains alive and well eight years after initial removal of the tumour from the IVC.
History
A 47-year-old man presented with painless haematuria in September 2000. He had a past medical history of hypercholesterolaemia and intermittent iritis. He previously had a right nephrectomy in 1992 for unilateral reflux into an atrophic kidney. Apart from the scar of his previous nephrectomy no other abnormality was found on physical examination. Bilateral retrograde ureterograms, renal ultrasound scans and flexible cystoscopy were all normal. Computed tomography (CT) demonstrated a tumour extending from the renal pedicle into the lower pole of the left kidney. Preoperative assessment indicated that the tumour involved only part of the kidney and did not extend into the inferior vena cava (IVC). At operation, in October 2000, the planned left partial nephrectomy was not possible as the tumour mass was found to extend into the left renal vein and the IVC. A vascular surgeon was not present at the operation and a decision was made not to attempt IVC resection. A left nephrectomy was performed leaving residual tumour in the stump of the left renal vein and the IVC. The patient recovered well and was started on haemodialysis after surgery. Histology showed a moderately differentiated grade 2 renal cell cancer with tumour within the lumen of the left renal vein. After discussion with the oncologists, a decision was made not to treat him with adjuvant chemo- or radiotherapy.
A follow-up CT scan performed five months after the surgery demonstrated tumour extending from stump of left renal vein into the IVC. A cavogram confirmed the presence of a tumour thrombus in the sub-hepatic portion of the IVC. The patient requested further surgery and in April 2001 an exploration of the abdomen through a right thoracoabdominal approach was carried out. The liver was mobilized and the IVC was found to contain tumour from the left renal vein up to the hepatic vein confluence. This was resected en block and the IVC was reconstructed using an 18 mm polytetrafluoroethylene (PTFE) ring-supported graft anastomosed end to end between the proximal and distal portions of the vena cava. As the patient wished to have renal transplant in the future, graft replacement of the IVC was carried out to provide good venous outflow for the future transplant. The patient made an uneventful postoperative recovery. He was placed on heparin 5000 units twice a day for 10 days postoperatively, but was not maintained on long-term anticoagulation. He continued on haemodialysis while awaiting a renal transplant.
A CT scan performed three years later, as part of the work-up for renal transplantation demonstrated that the PTFE graft had occluded (Figure 1). The patient had developed good collaterals and remained symptom free (Figure 2). In October 2005, just prior to transplantation, he was admitted to hospital with fever, malaise and lethargy. Repeated blood cultures including those taken from the dialysis catheter were negative. A CT scan revealed an air fluid level in the IVC graft indicative of anaerobic infection (Figure 3). A white cell scan confirmed this and showed a heavy accumulation of labelled white cells in the region of the graft.

Coronal computed tomography scan showing thrombosed (arrowed) inferior vena cava graft

Cavogram showing thrombosed inferior vena cava graft with collateral flow of contrast through the azygos and hemi-azygos veins
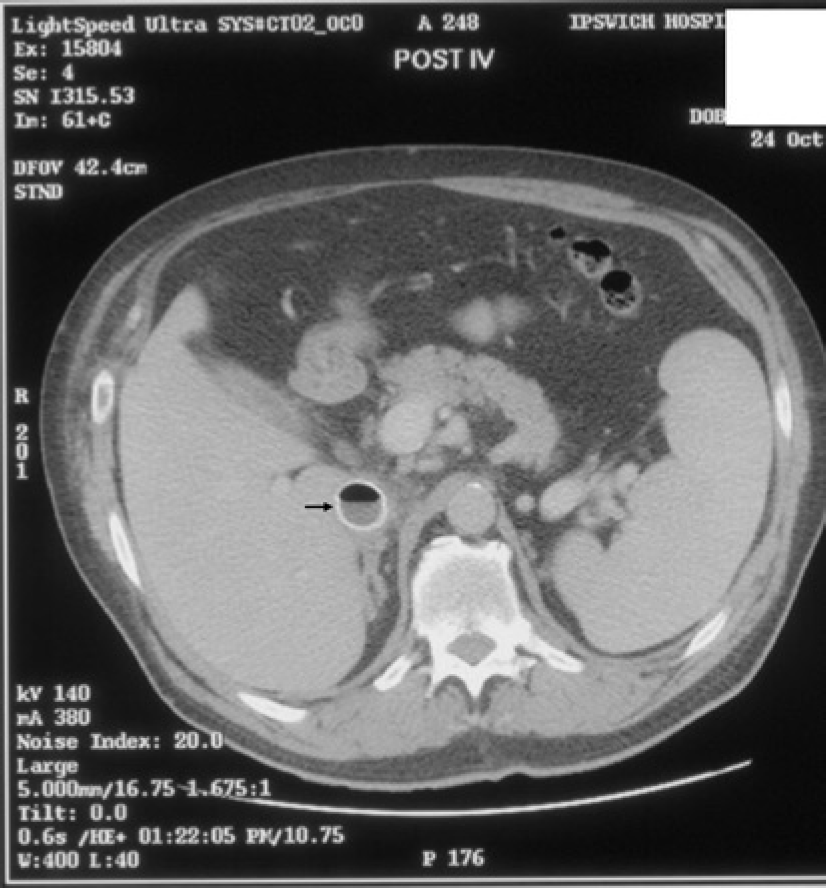
Axial computed tomography scan showing an infected inferior vena cava with air fluid level (arrowed)
A decision was made to remove the infected IVC graft. The abdomen was opened through a Mercedez Benz incision. A fistula was found between the graft and the duodenum and this was closed by primary repair of the duodenum which was then covered by omentum. The infected PTFE graft was removed with oversewing of the lower end of the IVC. The graft was dissected out behind the liver and became free; haemostasis was not required. There was no evidence of tumour recurrence and the patient made a good recovery. A year after the removal of the infected graft the patient underwent renal transplantation, despite the absence of an IVC. The renal artery and vein were anastomosed to the left external iliac artery and vein, respectively. A Lich-Gregoir ureterocystostomy was performed in which the donor ureter is anastomosed extravesically to the recipient bladder. The patient again made a good postoperative recovery. The renal function that was poor initially has steadily deteriorated and after a year a recent creatinine level was 410 µmol/L. He is being considered for a second transplant.
Discussion
The incidence of renal cell carcinomas involving the vena cava is between 4% and 10%.
1
IVC involvement is more common on the right than on the left because of the
shorter renal vein. Symptoms usually appear late, are often non-specific and include
abdominal pain, back pain and pedal oedema.
2
CT and magnetic resonance imaging are useful techniques for making the diagnosis.
Treatment options for tumours extending into the IVC include: Complete excision and oversewing of the IVC with no graft; Replacement using prosthetic interposition graft; Partial excision of the vena cava with primary closure; Partial excision of the vena cava with patch graft; and
Resection of the IVC without reconstruction has been advocated by some authors
especially when the vessel is occluded or extensively scarred and well-developed venous
collaterals have developed.
6
There are no clear cut criteria to suggest a benefit of IVC replacement over
primary excision with no replacement. The presence of good collaterals, however, may
tilt the balance towards excision without replacement. Yoshidome et
al.
3
have reported a survival of up to 150 months, in a patient after circumferential
excision of IVC without a replacement graft.
There is evidence that concurrent reconstruction of the vena cava and excision of tumour can improve the overall survival of the patients. 7,8 The five-year survival rate in patients undergoing nephrectomy with IVC replacement for non-metastatic renal cell cancer range between 18% and 68%. 9,10 Survival in the same group of patients is, however, less than one year with nephrectomy alone. 11 The involvement of perinephric fat, lymph nodes or distant metastases are poor prognostic factors. 12
Complications of prosthetic replacement of the IVC include lower limb oedema, graft infection, graft occlusion, chylous ascites and cardiopulmonary complications. 13 Acute graft occlusion often requires an additional intervention, e.g. re-operation or stenting 8,14 but some patients remain symptom-free after a late postoperative occlusion of IVC. 15,16 This is only possible if the patient has developed good collaterals, as in this patient. Our patient subsequently underwent renal transplant based on the external iliac vein draining through the collaterals. Renal transplantation has been reported in patients with a thrombosed IVC 17 and it has also been carried out after IVC reconstruction. 18 This is the first report of renal transplantation after IVC excision without reconstruction.