
Abstract
Objectives
Impact of pregnancies on great saphenous vein (GSV) reflux patterns deserves clarification. Which GSV segment is most affected? Is the saphenofemoral junction (SFJ) involved?
Methods
Colour-flow duplex ultrasonography was performed in 583 women extremities with primary varicose veins (clinical, aetiological, anatomical and pathological elements [CEAP C2]), without oedema, skin changes or ulcer. Women with previous thrombosis or varicose surgery were excluded. GSV reflux sources and drainage points were located at SFJ, thigh, knee and calf. Prevalence of most proximal reflux source was noted as a function of 0, 1, 2, 3 and 4 or more pregnancies. χ2 statistics was employed.
Results
Prevalence of GSV reflux was not dependent on 0, 1, 2, 3 or ≥4 pregnancies: 75%, 69%, 79%, 70% and 76% for right leg (P = 0.79) and 78%, 81%, 82%, 79% and 73% for left leg (P = 0.87), respectively. Prevalence of SFJ reflux and GSV reflux, starting at the thigh, knee or calf, was similar and showed no tendencies to increase with number of pregnancies.
Conclusions
Number of pregnancies did not influence GSV reflux patterns in women with primary varicose veins.
Introduction
Pregnancy is a risk factor for the development of varicose veins. 1 Common teaching based on clinical observations is that primary varicose veins are frequently noted first and progress during pregnancy, and often become more severe with subsequent pregnancies. 2–4 The prevalence of varices increases with number of pregnancies, 5 but this finding is not universal, particularly if only a small number of pregnancies are considered. 6
Both hormonal and haemodynamic forces influence venous dilation and elongation. 7 The diameters of superficial veins in pregnant women with varicose veins increase during pregnancy but decrease during the postpartum period to return to their baseline values. 8 In particular, the diameter of a competent or incompetent great saphenous vein (GSV) at the thigh dilate an average of 25% or 40%, respectively, during pregnancy.
Prevalence of GSV reflux is high in women with varicose veins. 9 Clear delineation of reflux at the GSV thigh segment and saphenofemoral junction (SFJ) has implications for modern endovascular treatment. Thermal and chemical ablations are gaining popularity and are commonly performed without ligation of the SFJ. Besides, some procedures may be restricted to the thigh segment. 10–17 The premises for the creation of CEAP (clinical, aetiological, anatomical and pathological elements) classification include, besides proper description of patients, emphasis on studies limited to specific populations. 18 Therefore, based on a frequently asked question, our study of patterns of reflux in women with varicose veins was further restricted to subgroups according to the number of pregnancies. The findings of this analysis may differentiate potential treatment approaches based on the number of pregnancies or may identify topics for further investigation.
Methods
Details of the patient population studied, medical history, physical examination and patterns of GSV reflux as determined by ultrasonography (US) have been previously described. 9 Specific details pertinent to number of pregnancies and determination of most proximal source of GSV reflux are described below.
Inclusion criteria
Subjects were referred to an independent, outpatient, non-invasive, vascular laboratory of a cosmopolitan, Brazilian state-capital with 1,500,000 inhabitants. The physicians of this vascular laboratory have more than 6–10 years of experience on vascular ultrasound and are used to performing over 1000 evaluations per year. The primary source of referral were vascular surgeons specialized on venous disease. This vascular laboratory has examined primarily a middle-class, European descent population with concerns about every-day function and cosmetic appearance. Most of these patients had private medical insurance and all sought treatment for their venous insufficiency.
Only extremities of women with primary varicose veins (C2) were included in this study.
Exclusion criteria
After exclusion of all men (n = 201 extremities), women with a history of previous venous surgery and/or past or present venous thrombosis or phlebitis (n = 44), and women in classes C1 (n = 289), or C3–C6 (n = 315), there were 590 extremities of women in class CEAP C2. The proportion of women with 0, 1, 2, 3 and 4 or more pregnancies in the subgroup C2 and subgroups C3–C6 combined were similar, varying by less than 4%. Due to the small number of extremities in each of the C3, C4, C5 and C6 classes, analysis was restricted to the C2 subgroup. Additionally, seven cases were excluded because of inadequate information to determine the site of the most proximal source of reflux. Reflux in deep or superficial veins besides the GSV were not reason for exclusion of the study.
Selected population
A total of 583 extremities with primary varicose veins of 339 women were included in the analysis; 244 studies were bilateral and 95 were unilateral examinations. Average age was 42 ± 14 (SD) (median 40, range: 8–87) years. This was not a screening population, but included patients who sought treatment. The objective of the exam was a detailed preoperative or pre-treatment mapping.
US examination: GSV
The US examination of the GSV was part of a complete evaluation of leg veins including the small and accessory saphenous veins and their interconnections, and other unusual anterior, lateral and posterior veins, either dilated and/or associated with varicose veins. Deep veins were evaluated for thrombosis or reflux. The examination was performed with the subject standing, from the groin to the ankle. Reflux was determined following release of compression distal to the site of US observation. Multiple manual compression/release manoeuvers provided an extensive evaluation of reflux. Vascular physicians with extensive experience including thousands of cases provided their report and were not directly or indirectly connected with treatments proposed to the patients. Automatic compression/decompression devices were considered in the past but were disregarded as not providing as diverse and complete clinical assessment as multiple manual compressions at different sites. Reverse flow lasting longer than 500 milliseconds was considered reflux; in the vast majority of cases, however, reflux was longer than one second. The source and drainage of each refluxing segment was noted. The standard reporting included distance measurements for exact location of source, drainage and other significant findings (Figure 1). The type of source and drainage was ascertained. Besides the common femoral vein via the SFJ, sources of reflux could be a tributary of the SFJ, a tributary of the GSV or a perforating or communicating vein. GSV reflux could drain via a GSV tributary or a perforating or communicating vein.
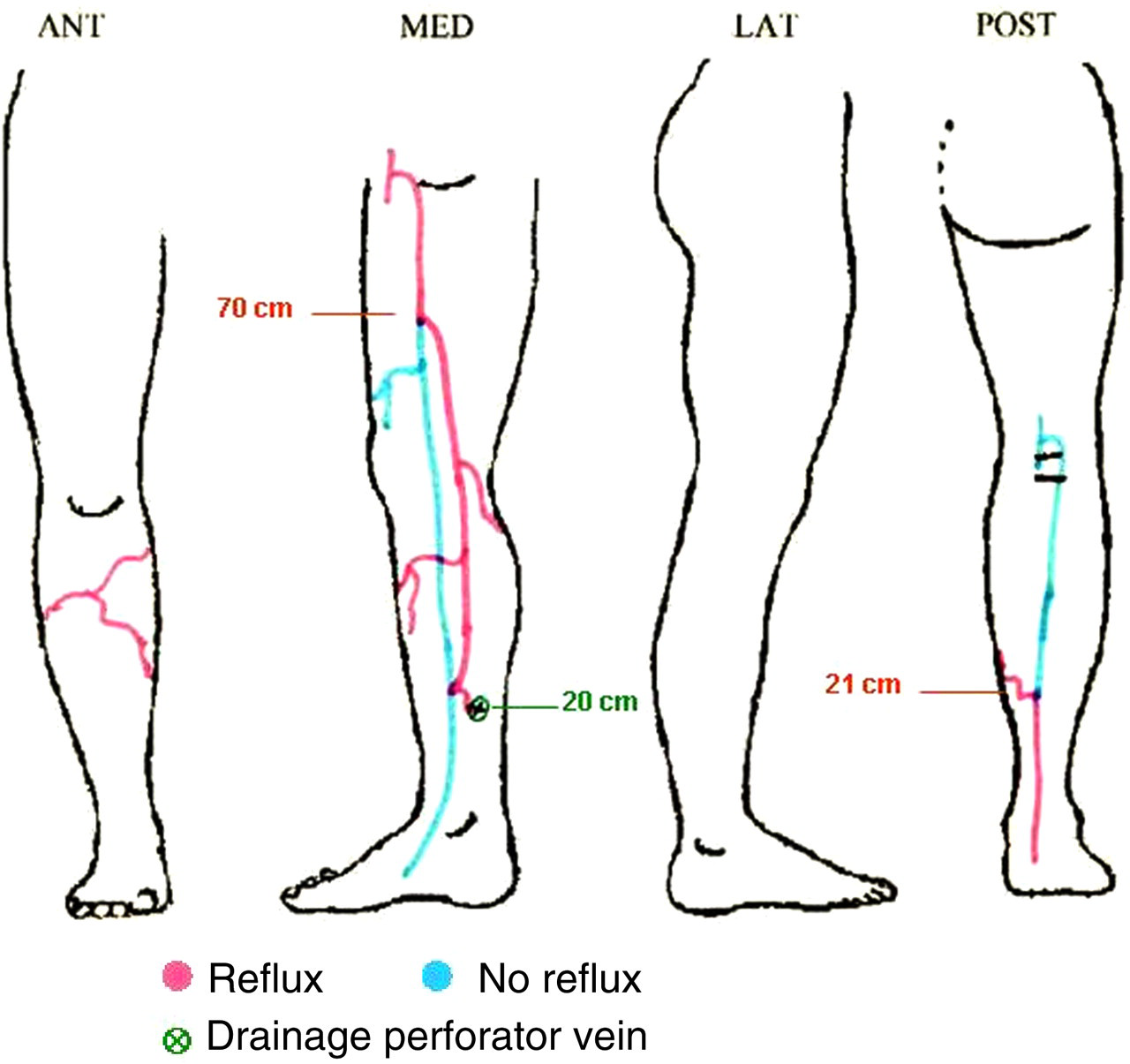
Example of the schematics of a lower extremity vein mapping for evaluation and treatment of chronic venous valvular insufficiency. Normal forward flow in blue, abnormal reverse reflux in red. Colour version available online
Patterns of reflux were determined as previously described (Figure 2):
9
Perijunction SFJ tributary to the GSV; From the SFJ through the proximal GSV; From a tributary or perforating vein through the distal GSV to the ankle level; From a tributary or perforating vein to another tributary or perforating vein through a segment of the GSV; Through more than one segment of the GSV, subdivided into two subgroups:
V-1: competent SFJ; V-2: incompetent SFJ as source of proximal segment reflux; Diffuse reflux of the entire GSV from SFJ to the ankle.

Great saphenous vein (GSV) reflux patterns. Patterns of GSV reflux. I: perijunction, proximal; II: junction, proximal; III: distal; IV: segmental; V-1: no junction, multisegmental; V-2: junction, multisegmental; VI: diffuse from junction to ankle
The site of the most proximal refluxing segment was determined by the most proximal source of reflux. GSV reflux patterns II, V-2 and VI indicated SFJ reflux. Patterns III, IV and V-1 were analysed in detail to determine if the source was at the thigh, knee or calf level.
Statistical analysis
Prevalence of GSV reflux patterns, as preliminary descriptive statistics, was estimated as a function of number of pregnancies. Prevalence of GSV reflux was calculated as a function of number of pregnancies for the right lower extremities and for the left lower extremities.
Prevalence of most proximal source of reflux at the SFJ, thigh, knee or calf was estimated as a function of number of pregnancies for all right and left lower extremities in the database. Prevalence of GSV reflux patterns as a function of number of pregnancies was compared using the χ2 function available on the Excel program.
Results
Prevalence of GSV reflux did not increase with number of pregnancies as shown in Table 1, regardless of whether the analysis was performed for the right or for the left extremity. Comparative χ2 statistics were similar regardless of whether the comparison was performed for right or for left extremity.
Prevalence of great saphenous vein (GSV) reflux as a function of number of pregnancies in extremities of women with primary varicose veins, CEAP clinical class C2
NP: number of pregnancies; R LE: right lower extremity; L LE:left lower extremity; CEAP, clinical, aetiological, anatomical and pathological elements
Prevalence of GSV reflux patterns as a function of number of pregnancies are shown in Table 2. For all subgroups of number of pregnancies, the most common pattern of GSV reflux was IV: single segment. The second most common pattern for all subgroups was V-1: multisegmental without involvement of the SFJ. The patterns involving the SFJ, II, V-2 and VI, were slightly more common than the distal pattern of reflux III.
Great saphenous vein (GSV) reflux patterns as a function of number of pregnancies
NP: number of pregnancies I-…-VI: GSV reflux patterns; I: peri-saphenofemoral junction (SFJ), post-terminal valve source of reflux; II: proximal GSV reflux from SFJ; III: distal GSV reflux from tributary/perforator vein to ankle level; IV: segmental GSV reflux from tributary/perforator to tributary/perforator; V-1: GSV multisegmental reflux not involving the SFJ; V-2: multisegmental reflux having the SFJ as the most proximal source of reflux; VI: diffuse GSV reflux from SFJ to ankle; total right, total left: number of refluxing GSV
Table 3 shows the prevalence of the most proximal sources of reflux as a function of the number of pregnancies. The low prevalence of reflux starting at the SFJ was independent of number of pregnancies.
Most proximal source of great saphenous vein (GSV) reflux as a function of number of pregnancies
NP: number of pregnancies; SFJ: saphenofemoral junction; total right, total left: number of refluxing GSV
Discussion
Prevalence of right or left GSV reflux in women with primary varicose veins was not dependent on number of pregnancies. Prevalence of the most proximal source of GSV reflux was not altered by number of pregnancies. These findings were pertinent for a specific patient population of Brazilian women, mostly of European descent, clinical CEAP class C2. As C3–C6 patients were excluded, these findings may represent early stages of disease. GSV reflux was primarily segmental and primarily in the calf. Only about 1/3 of the extremities with simple varicose veins were potential candidates for endovascular ablation of the thigh segment of the GSV, and only about 1/5 may have needed correction of the SFJ. These observations are independent of the number of previous pregnancies. The analysis design complied not only with a specific description of patients (C2) as prescribed by the CEAP committee but also with an implied intension of research limited to very specific sample populations. We suggest that patients with healed or open ulcers, skin changes and oedema should not be grouped together with patients having only primary varicose veins. Patients with more advanced disease may very well have different patterns of GSV reflux. Other pertinent factors related to the influence of pregnancy on chronic venous valvular insufficiency should be studied in very specific populations.
Most likely, the women in this study had varicose veins with simple patterns of GSV reflux before becoming pregnant, or developed such patterns of GSV vein later, regardless of any pregnancy. Based on our results, we raised the hypothesis that it is not the number of pregnancies but other factors during a ‘bad’ pregnancy that may lead to deterioration from a clinical class C2 with primary varicose veins to a class C3 representing venous oedema, or even C4 for significant skin changes. This ‘bad’ pregnancy could be the first or any other.
Another narrow focus of this investigation was on patterns of GSV reflux. Larger study populations would be necessary to evaluate the small saphenous or the saphenous accessory veins. 9 Our findings do not contradict previous reports of alterations in superficial vein diameter 8 or increased prevalence of varicose veins with numbers of pregnancies. 5 One must realize, however, that changes in diameter during pregnancy may fail to result in permanent alterations of diameter. A recent study of GSV diameter in Equatorian women also failed to demonstrate GSV diameter enlargement with number or pregnacies. 19,20 Other parameters of the venous circulation may not be affected by number of pregnancies also. Kriessman 21 indicated that abnormal venous pressures detected in the third trimester did not correlate with the number of previous births. Future investigation is warranted to determine whether the number of pregnancies is most related with development of varicose veins in other venous networks besides the GSV.
Patterns of superficial vein reflux may be different for populations of cold climates, different social classes such as those living in the Brazilian rural areas, different ethnicity, male gender, patients who only seek medical attention with advanced disease or screening of a general population. The focus of this analysis was on early stages of disease.
In summary, prevalence of GSV reflux in women with primary varicose veins in the absence of oedema, skin changes or ulcers was not related to the number of pregnancies. The prevalence of the anatomical site of the most proximal source of reflux, be it at the SFJ, thigh, knee or calf, also failed to be related to the number of pregnancies. Number of pregnancies may be a crude factor to describe the effects of pregnancy on venous valvular insufficiency. Other pregnancy-related factors besides number, such as duration of pregnancy, twins or more babies, duration and mode of labour, should be evaluated as potential causes of clinical degeneration, deterioration of patterns of GSV reflux and/or varicose veins associated with other venous networks.