
Abstract
Objective
The purpose of this study was to visualize the shunt flow of arteriovenous fistulas (AVFs) passing towards the top side of the foot from the plantar artery.
Methods
Colour-flow duplex Doppler ultrasonography was performed in 112 patients who consulted an outpatient clinic with varicose veins and/or symptoms such as foot oedema, dullness, cramp and coldness. Thirteen age-and sex-matched healthy subjects served as controls.
Results
AVFs were detected in 86 of 112 patients (77%). They were also detected in 10 (77%) of 13 healthy subjects. The shunt flow pattern consisted of two phases of flow corresponding to systole and diastole, and the diastolic fraction of time–velocity integral was larger, although the peak flow velocity in systole was higher than that in diastole.
Conclusion
Colour-flow duplex Doppler ultrasonography is useful for non-invasive visualization of the shunt flow of AVFs connecting the plantar artery with the venous arch of the top side of the foot.
Introduction
Arteriovenous fistulas (AVFs) in patients with varicose veins have been documented by visual observation during surgery with the use of high-powered microscopes or magnifying lenses. 1–6 In 1987, Haimovici 6 reported a precise distribution of AVFs, but most of AVFs were observed along the medial aspect of the calf. Here, we propose a new approach for the detection of AVFs passing towards the top side of the foot from the plantar artery using colour-flow duplex Doppler ultrasonography.
Methods
We studied 112 consecutive patients (21 men and 91 women), aged 18–88 years (mean 60.5) who consulted an outpatient clinic with varicose veins and/or symptoms such as foot dullness, coldness, oedema, cramp and ulceration. Seventy-four patients had primary varicose veins without any previous operative procedures. Twenty-six patients had undergone surgical ligation, stripping or endovenous laser surgery for the incompetent great and/or small saphenous veins. Among 26 patients, five patients had recurrent varicositis and 21 patients complained of foot coldness, oedema, clamp and ulceration despite successful operative treatment. The remaining 12 patients had symptoms without varicose veins. Thirteen age- and sex-matched healthy subjects served as controls. This study was approved by the institutional human ethical committee.
After footbath (temperature 38–40°C, for 5 minutes), all subjects were examined using colour-flow duplex Doppler ultrasonography (LOGIQ P5 Ultrasound System; GE Healthcare, Fairfield, Connecticut, USA) with a 12 MHz transducer. The ultrasound beam was placed perpendicularly just below the venous arch of the top side of the foot, and the first to the fourth interosseous space was scanned from the base of the toes to the venous arch in the standing position (Figure 1). When the AVFs were detected on the colour Doppler ultrasonography, the sample volume was located on the AVF and blood flow velocity was recorded using the pulse-wave Doppler ultrasonography. Furthermore, blood flow velocity and diameter of the dorsalis pedis artery at the proximal part of the first interosseous space were measured before and after footbath.

Duplex Doppler ultrasonographic approach. The ultrasound transducer was placed perpendicularly at the site of the venous arch of the top side of the foot in the standing position
Results
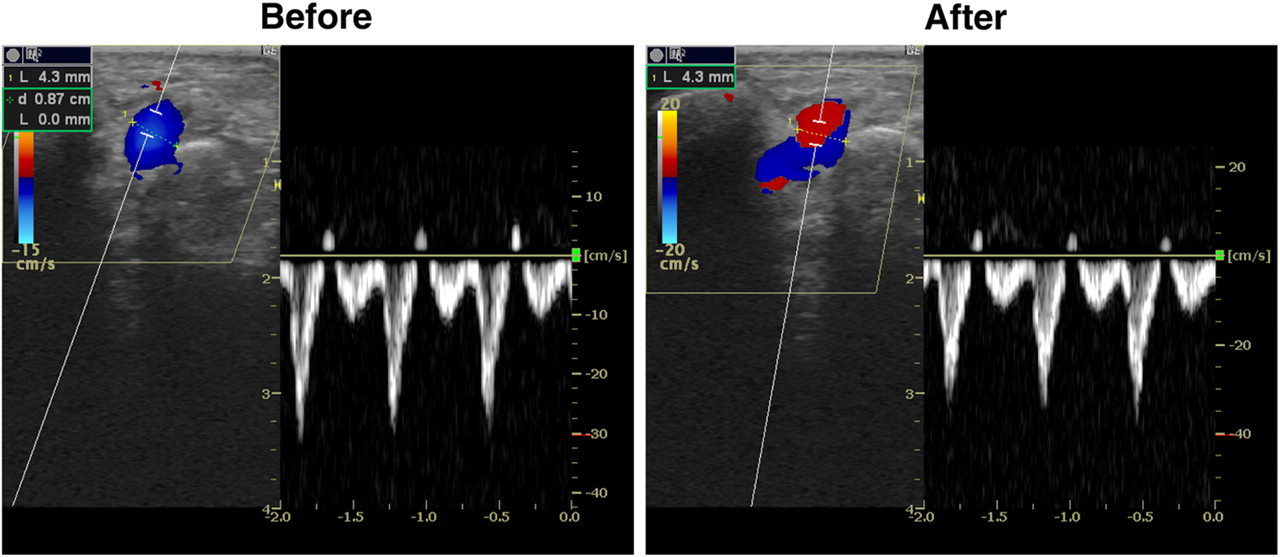
The AVFs were visualized with the colour Doppler ultrasonography in 86 (77%) of 112 patients and they were also detected in 10 (77%) of 13 health subjects (Figure 2). Blood flow velocity was successfully recorded with pulsed-wave Doppler ultrasonography. The number of AVFs was one to four in the one foot, usually symmetric in both feet. The size of AVFs ranged from less than 1.0 to 6.0 mm in diameter. The flow pattern of AVFs consisted of two phases corresponding to the systole and diastole. Diastolic flow velocity was predominant in the time–velocity integral, although the peak flow velocity in systole was higher than that in diastole (Figure 3). There were no significant differences in the blood flow velocity and diameter of the dorsalis pedis artery before and after footbath (Figure 4).

Colour Doppler ultrasonographic image of an arteriovenous fistula (AVF). Red signal shows an AVF flow into the venous arch of the top side of the foot from the plantar artery (colour figure can be seen in online version)

Flow pattern of an arteriovenous fistula. Biphasic flow velocity pattern was obtained with the pulse-wave Doppler ultrasonography
Blood flow velocity of the dorsalis pedis artery before and after footbath
Discussion
The pathogenesis of varicose veins is recognized as the result of primary valvular insufficiency of the great and small saphenous veins and incompetence of the perforating veins. AVFs were postulated as one of the underlying causes of varicose veins. Although the presence of AVFs in patients with varicose veins was documented, the distribution was limited from the ankle to the thigh. 6 To the best of our knowledge, the presence of AVFs on the top of the foot has not been reported until now.
Colour-flow duplex Doppler ultrasonography enabled us to visualize the shunt flow of AVFs arising from the plantar artery. In the majority of cases, the AVFs are closed under the normal temperature. However, blood flow through the fistula appears in the presence of relatively high temperature. Therefore, we attempted to detect the AVFs after footbath for an optimal recording. In this study, the prevalence of AVFs in the top side of the feet was 77%. The AVFs are natively pre-existent as natural vascular channels connecting the artery with venous circulation. 6 They allow the arterial blood to pass directly into the veins bypassing the capillary bed. However, if the shunt flow is persisting or occurring relatively often, this condition predisposes the abnormal pathological milieu. 6 Recently, endovenous laser surgery has been introduced as a minimal invasive alternative of surgical ligation and stripping for varicose veins. 7–9 The treatment of AVFs on the top side of the foot with the new therapeutic modality is now being studied, since the arteriovenous shunting is logically eliminated. Implications of AVFs on the foot should be investigated in future studies, focusing on the relationships with clinical symptoms and signs.
In conclusion, with the use of colour-flow duplex Doppler ultrasonography, visualization of the shunt flow of AVFs from the plantar artery towards the venous arch of the top side of the foot was successful in about three-quarters of individuals irrespective of clinical symptoms and signs of the foot.
Footnotes
Acknowledgement
The authors thank Yukiko Okumura for her meritorious assistance as secretary.