
Abstract
Objective
To review the evidence regarding interventions (compression, sclerotherapy, surgery and endoluminal) for uncomplicated venous disease.
Method
A literature search of MEDLINE and EMBASE was performed. In addition, bibliographies of published data and the Cochrane Peripheral Vascular Review Group Specialist Register were examined. Publications describing an intervention for uncomplicated venous disease or trials comparing one intervention against another were considered.
Results
Uncomplicated but symptomatic varicose veins are associated with a significant reduction in quality of life (QoL). Evaluation must include a detailed history and examination supported by non-invasive imaging. Although HHD is useful, its utility is limited in the popliteal fossa. It can not provide morphological/anatomical detail when considering an endoluminal treatment option. Regardless of intervention, all treatments considered are associated with a significant improvement in QoL at acceptable cost.
Conclusion
Uncomplicated symptomatic varicose veins lead to a reduced QoL, which can be significantly improved by all interventions considered.
Keywords
Varicose veins affect between 10% and 25% of the adult population in the UK 1 with an estimated 100,000 procedures performed each year. 2 Recent evidence from Hospital Episode Statistics suggests that venous interventions for varicose veins have fallen over the last five years and in 2005–2006 was less than 60,000 per annum. The annual incidence is reported to be 2.6% in women and 1.9% among men. 3 Varicose veins remain a condition predominantly in developed industrialized countries,4,5 with national estimates of prevalence between 2% and 56% for men and 1% to 73% among women. 6 As such, venous interventions comprise a significant proportion of the workload of a vascular unit. 7 Currently, due to the increasing pressure on health-care resources and waiting times, there is renewed debate regarding the appropriateness of using scarce health-care resources to provide interventions for uncomplicated varicose veins. 8 This does, however, conflict with the increasing accessibility of medical information and rapidly evolving field of minimally invasive venous interventions. There exists currently an uncertainty among health-care commissioners, consumers and health-care professionals. The aim of this paper is to review the available interventions and the evidence for their use in patients with uncomplicated varicose veins. Details of individual techniques and in-depth discussion regarding their provision and training requirements will be presented in subsequent papers.
Varicose veins have been defined by Porter and Moneta 9 as dilated palpable subcutaneous veins generally larger than 3 mm in the upright position. While many varicose veins are associated with a variety of symptoms in the legs, most are not associated with complications such as skin change, oedema, bleeding or ulceration. The term chronic venous insufficiency is used to imply development of one of these complications.
Aetiology
Adult veins begin as a series of capillary plexuses which, following differential recruitment of supporting cells and remodelling processes, become transformed into mature veins. 10 At present there is no consensus agreement on the sequence of events that ultimately cause transformation to a varicose vein. There is evidence that appears to suggest key events include:
Vein wall weakness due to alterations in the supporting tissues (elastin/collagen); 11
Venous dilation resulting in valvular incompetence and subsequent reflux. 12
Clinical factors positively associated with varicose veins include: familial aggregation, increasing age, female sex, multiple pregnancies, obesity and reduced physical activity. 13
Anatomy
The normal adult vein consists of three distinct layers:
Tunica intima – consisting of endothelial cells supported by a delicate network of fibroblasts;
Tunica media – containing predominantly elastin fibres;
Tunica adventia – made from loose connective tissue.
The main truncal veins contain a series of valves situated mostly at predictable sites that normally encourage unidirectional flow against gravity. Microscopic examination of the valves reveals that they are inward projections of the tunica intima, strengthened by collagen and elastin fibres. 14 This venous architecture allows venous vessels to function as high volume, low pressure conduits for transporting blood back to the heart.
The superficial veins of the lower limb comprise the following:
The great saphenous vein
The great saphenous vein (GSV) arises on the medial aspect of the dorsum of the foot and passes anterior to the medial malleolus. It continues along the medial aspect of the leg, posterior to the medial tibial condyle and into the thigh. The GSV in the leg is often accompanied by two main tributaries – the anterior accessory saphenous vein of the GSV and the posterior accessory vein of the GSV. The latter may also receive drainage from perforating veins. The termination of the GSV is always located in the inguinal crease.
The small saphenous vein
The small saphenous vein (SSV) begins at the lateral malleolus and passes superficially up along the lateral border of the tendoachilles. Commonly, it will perforate the deep fascia at mid calf level; continue up between the bellies of gastrocneumius and drain into the popliteal vein within the popliteal fossa. Unlike the great saphenous termination, there is considerable variation in the termination of the SSV The anatomical arrangements may include: union with the popliteal vein out with the popliteal fossa; continuation of the SSV with the medial gastrocneumius vein with or without a common trunk; continuation of the SSV into the Giacomini vein; or termination of the SSV without a saphenopopliteal junction either blindly in the calf or via a plexus of veins within the deep thigh muscles.
Perforating veins
These allow flow of blood from the superficial system to the deep veins via unidirectional valves. They are classically arranged into two groups: the anterior group that connect the anterior accessory saphenous vein to the anterior tibial vein and vary from three to 10 in number; and the posterior group that connect the posterior accessory vein of the GSV with the posterior tibial vein.
Clinical presentation
A variety of objective (varicose eczema, pigmentation, bleeding and ulceration) and subjective (heaviness, aching and itching) symptoms are known to be commonly associated with varicose veins. The correlation between symptoms or symptom severity relative to the extent of visible appearances of varicosities is at best poor. 15 Despite this, the presence of symptoms continues to play an important patient-centred role and is used in clinical decision-making. 16
Assessment
Assessment should begin with an inspection of the leg and the distribution of varicose veins, presence of oedema, induration and skin changes secondary to chronic venous insufficiency. Traditional examination has been superseded by hand-held Doppler (HHD) testing and duplex vein imaging. Clinical evaluation alone is unreliable for varicose veins, even when performed by experienced clinicians. 17 The presence of visible varicosities in any given site correlates poorly with the presence of truncal reflux in the corresponding vein on duplex imaging. 18 This disparity is even more marked when assessing recurrent varicose veins where clinical examination cannot distinguish between groin neovascularization and intact saphenofemoral junction/intact GSV. 19 The use of a HHD has become very popular and the technique is readily learnt. It is particularly useful in screening for absence of reflux. Nevertheless, it has limitations as follows:
It has better sensitivity/specificity when used for the assessment of the saphenofemoral junction compared with the saphenopopliteal junction, 20 explained largely by the anatomical variability of the latter; 21
It cannot be used to discriminate between superficial and deep venous reflux in the popliteal fossa; 22
HHD assessment gives no information on morphological/anatomical features of the structures involved, which may become increasingly important with the increasing use of endovenous therapies. 23
HHD examination is an essential requirement for the evaluation of all patients with venous disease being considered for treatment. In comparison formal duplex imaging allows identification of the highest point of reflux as well as providing anatomical and morphological features of the involved system. The use of HHD/duplex imaging is known to vary across the UK in the assessment of new patients with primary or recurrent GSV/SSV and may represent operator preference, resource availability, vascular laboratory workload and cost.24,25 If preoperative duplex imaging is to be used, it is argued by some that it is best performed by the operating surgeon, as duplex-derived information is not accurately communicable in the written form. 26 In terms of conventional surgical intervention, the utility of preoperative duplex imaging remains controversial. It is argued by some 27 that although its routine preoperative use reduces recurrence rates this itself does not result in a subsequent improvement in quality of life (QoL). Others argue preoperative duplex imaging did not assist in reducing clinical recurrence or neovascularization.25,28 With the advent of endovenous technologies, there is now a clear need for duplex imaging mandated by both case selection and technique. It is hard to maintain an argument against routine duplex imaging in the modern era given the extensive management options.29,30
Duplex ultrasound imaging has replaced venography as the standard investigation in assessing the pattern/severity of lower limb superficial venous reflux. 31 Duplex venous assessment of the leg should follow a structured protocol. The assessment of venous reflux is made with an augmentation manoeuvre (calf compression or Valsalva) and should include examination of the femoral and popliteal veins. Incompetence with reverse venous flow is regarded as significant if persisting for more than 0.5 seconds. 32 On completion of the examination, information regarding patency/competency of the deep venous system, anatomical configuration at the saphenofemoral/saphenopopliteal junction, competency and duration of reflux at the junction, extent of the reflux and location of incompetent perforating veins can be used to define reflux categories that may help define intervention protocols. 33
The case for intervention in uncomplicated varicose veins
It has been argued that treatment of uncomplicated varicose veins would prevent late complications such as skin change or ulceration. However, there are no long-term studies in the literature to justify this concept. Many patients have visibly significant varicose veins for years without ever developing complications.
Therefore, the only argument for intervention in patients with uncomplicated varicose veins is to relieve symptoms. While many patients also seek treatment for cosmetic reasons, the justification for commissioning venous intervention in nationally funded health-care systems relies on the successful treatment of symptoms.
The World Health Organization has defined health as a state of complete physical, mental and emotional wellbeing and not merely an absence of disease.34,35 In the context of clinical trials, health-related quality of life (HRQoL) can be considered as the functional effect of a condition and its consequent therapy on a patient, as reported by that patient. Instruments used to measure HRQoL may be generic and cover a wide range of health dimensions or be disease-specific. Disease-specific instruments are considered to be more sensitive at detecting minor changes in patient's health status.
Data regarding the natural history of venous disease and its impact on HRQoL are limited. Many studies have used the generic instruments and it is difficult therefore to separate the impact of the venous disease from other co-morbidities. In some studies, the sampling time-frames have been very heterogeneous, as have the patients, where both those with and without venous ulcers have been included. Despite these limitations, all studies reported to date described that symptomatic varicose veins have a negative effect on QoL compared with the general population without varicose veins. This is most noticeable in physical domains.36–42 The VEINES project 43 was an international (Belgium, Canada, France and Italy) prospective cohort collaborative study based on a sample of 5688 subjects conducted over a five-year interval. The patients aged from 18 to 75 years were recruited from outpatients. A random sample was then selected to be studied further. The primary outcome measure was QoL as measured by generic and disease-specific tools. Both generic and disease-specific QoL were directly linked to the clinical severity of the varicose veins, whether this was assessed by a validated staging/scoring system or the reviewing clinician alone. In addition to these prospective data are the results of QoL studies done before and after venous interventions, which universally show an improvement, irrespective of the type of treatment. Indeed, the health-gain benefits after superficial venous surgery are comparable with those gained after elective laparoscopic cholecystectomy.44,45
Options in management of varicose veins
Compression
Compression treatment of the leg can have a variety of objectives when used in the context of superficial venous disease management. In certain circumstances it may be primary therapy, for example, in patients with leg ulceration where four-layer compression bandaging is an evidence-based primary treatment. Compression is also an adjunct following an invasive intervention, such as surgery, sclerotherapy or endovenous thermal ablation. Postintervention compression has benefits in reducing the risk of thromboembolism and improving comfort, but may also contribute to speed of recovery. The optimum period of compression after intervention remains unclear, however, there seem to be few benefits beyond one week. 46
Compression stockings may be employed as a primary treatment for patients with symptomatic varicose veins. They act by providing graduated radial pressure between ankle and knee/thigh, depending on the length. This combined with the action of the calf muscle pump facilitates cephalad blood flow and venous return. 47 In addition to the radial pressure, another important parameter of the compression garment is the elasticity (stiffness). Measurement of capillary filtration rate using air plethysmography has suggested that significant oedema associated with venous disease may be managed best with a higher stiffness stocking. 48 Classification systems for level of compression may vary but in the UK compression stockings are divided into three different classes based on their radial compression force:
Class 1 – 15–20 mmHg;
Class 2 – 20–30 mmHg;
Class 3 – 30–40 mmHg.
Rigorous scientific data regarding specific outcomes for compression hosiery as a primary therapeutic intervention are lacking. However, data from the REACTIV trial can be used to shed some light on this issue. 49 In this NHS-funded study, patients with varicose veins were categorized into one of the three groups:
Group 1 - Minor below knee varicose veins without truncal reflux;
Group 2 - Moderate below knee varicose veins with truncal reflux;
Group 3 - Significant varicose veins above and below the knee with truncal reflux.
Patients in Group 1 were randomized to either conservative treatment with compression hosiery or sclerotherapy. Subjects in Group 2 received either standard surgery or sclerotherapy. Participants in Group 3 were randomly allocated either conservative compression therapy or surgery. In addition, careful follow-up logs were kept of those patients refusing randomization within each group.
Overall, 57% of those randomized to conservative management with compression hosiery (Groups 1 and 3) expressed significant unhappiness with their treatment at one year; just over half requested alternative intervention. In Group 3, 63 of 122 (52%) patients allocated to receive conservative therapy had actually crossed to the surgical arm by three years. Furthermore, among the 290 patients in Group 3 who declined to participate, 198 (68%) had undergone varicose vein surgery within 12 months of follow-up.
Sclerotherapy
Sclerotherapy involves the injection of a sclerosant into the vein followed by compression, a technique that has been available for decades. 50 Sclerotherapy was popularized after results published in 1971 by Henry and Fegan, 51 who reported success in applying this technique to the treatment of venous ulcers. Currently, the technique has been modified for use in both axial (GSV/SSV) and non-axial veins. A number of variables are thought to be related to effectiveness and have been investigated. These include: type of sclerosant; physical state (liquid or foam); concentration; method of delivery; and finally method and duration of post-treatment compression.
The main studies identified using sclerotherapy and comparing outcome with standard surgery is summarized below while Table 1 summarizes the outcome from studies involved in the management of both truncal and non-truncal varicosities using different sclerosant(s)/preparation/compression regimens.52–64
Summary of clinical trials comparing different sclerosants and preparation techniques
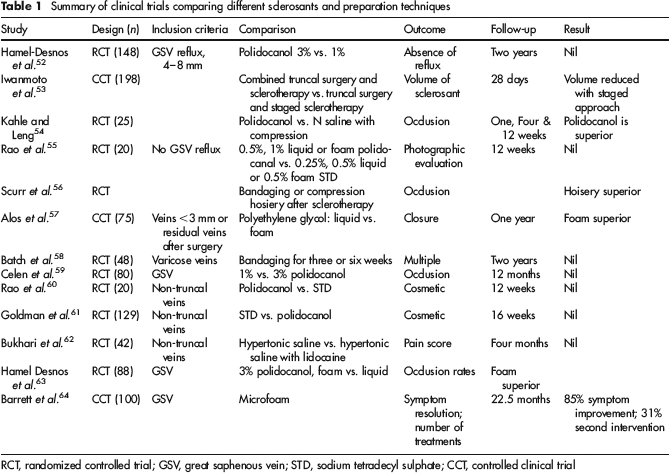
RCT, randomized controlled trial; GSV, great saphenous vein; STD, sodium tetradecyl sulphate; CCT, controlled clinical trial
Belcaro et al. 65 conducted a multicentre international study with 887 patients randomized between three sclerotherapy regimens, two surgical groups and one combined arm. Follow-up included regular duplex examination and continued for 10 years, with only 16% attrition. In the groups receiving only sclerotherapy, recurrence rates after five and 10 years varied between 29–32% and 34–38%. For the surgical arm corresponding figures were 22–28% and 24–29%. For the combined group, recurrence at five years was 22% and at 10 years 24%. Data regarding QoL or cost were not available.
In a parallel group randomized trial conducted by Chant, 66 115 of 214 patients underwent sclerotherapy, the remainder had standard surgery. The primary outcome measure chosen was the need for further treatment and follow-up extended to five years. The attrition rate was 7% at three years. There was no difference in reintervention after three years, but at five years 40% of the sclerotherapy group had required some form of reintervention compared with 24% in the surgical arm.
Einarsson et al. 67 studied 164 subjects, 84 underwent sclerotherapy and 80 had surgery. Follow-up extended out to five years with a 22% drop out rate. Although outcome as measured by ‘treatment failure’ was similar initially, by five years there was significant difference: 74% in the sclerotherapy arm and 10% in the surgical cohort. In this three-arm randomized trial, 516 patients were randomized by Jacobson et al. to receive surgery under general or local anaesthesia consisting of saphenofemoral/saphenopoliteal ligation, compared with sclerotherapy alone. Outcome was based on assessing the level of recurrent visible varicosities at follow-up in conjunction with subjective patient assessment. After three years there was a significant superiority in favour of truncal surgery under general anaesthesia (GA).
Finally, Rutgers and Kitslaar 68 studied 156 patients randomized to truncal surgery under GA or ligation of the saphenofemoral/saphenopopliteal junctions under local anaesthetic combined with sclerotherapy. Outcome was well structured and included duplex examination. Recurrence rates after three years were least in the surgical arm.
Standard surgery
Standard surgery for varicose veins was first described over a 100 years ago 69 and remains the basis for treatment. 70 Careful informed consent is a vital component to reduce the risk of medical litigation, since varicose vein surgery is a common cause.71–74 A number of components of the procedure can affect the outcome, such as stripping the GSV to minimize the risk of recurrence.75–77 Stripping does, however, increase postoperative morbidity, including pain, bruising and sensory loss in up to 40%. 78 Infiltration of the strip track with local anaesthesia has been shown to reduce early postoperative analgesic requirements, while use of a surgical tourniquet may reduce blood loss. 79 Whether the saphenofemoral junction is transfixed or flush-ligated appears to make little difference in terms of recurrence rates when combined with GSV striping, but both techniques produced significant improvements in QoL postoperatively. Similarly, in the short saphenous system stripping is associated with reduced recurrence and improved QoL. Although there appears to be no standardized technique for stripping, most techniques utilize an inversion principle.
There are a number of alternative methods of dealing with the GSV.
Cryostripping
Investigators found that both surgical stripping and cryostripping of the GSV improved QoL. There was no difference in postoperative pain or sensory deficit at six months. Bruising was significantly less after cryostripping. 79
Bipolar coagulation
In this technique, during stripping the GSV is withdrawn into the stripper while side branches are severed by coagulation. 80 Compared with conventional stripping, this technique has shown significantly less postoperative haematoma formation in the strip track and subsequent reduction in time of work and pain scores. A recent study that observed a relationship between strip track haematoma and later neovascularization suggests that any technique that reduces postoperative haematoma may improve long-term recurrence rates. 81
Phlebectomy
Following removal of the GSV, calf and thigh varicosities are usually dealt with by individual phlebectomies. The use of phlebectomy instruments allows this to be performed through micro-incisions. 82 Transilluminated powered phlebectomy is a new device that can remove superficial veins over a wide area using fewer incisions, but it is associated with significant postoperative pain, increased bruising and sensory deficits are common. This method decreases the usual improvements in HRQoL after varicose vein surgery.83–87
Thermal ablation of the GSV
Modern technology has enabled minimally invasive techniques to be developed for the treatment of varicose veins. This is an alternative for the management of incompetent GSV and SSV segments. These new techniques include endovenous laser therapy ablation (EVLA) and radiofrequency ablation (RFA). Although achieved by different technologies, the basic mechanism of action is similar, with initial endothelial and subendothelial thermal damage with organization of thrombus and subsequent vein wall damage. 88 The vein may subsequently disappear as normal healing leads to re-absorption and elimination of the vein from the leg. In both techniques, the procedure can be performed in the conscious patient using regional (tumescent) anaesthesia and does not require a sterile operating theatre environment. They represent the transfer of treatment for varicose veins away from provision in hospital to outpatient and ambulant therapy. The early and intermediate outcomes, occlusion and QoL following RFA/EVLA are summarized in Table 2.
Early and intermediate outcome following endovenous laser and radiofrequency ablation
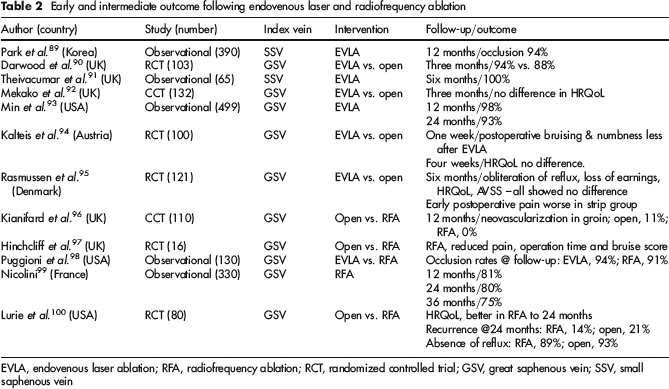
EVLA, endovenous laser ablation; RFA, radiofrequency ablation; RCT, randomized controlled trial; GSV, great saphenous vein; SSV, small saphenous vein
Economic considerations
Since treatment for uncomplicated varicose veins is designed to improve QoL, an assessment of the cost-benefit ratio is important and should be compared with other similar interventions. The REACTIV HTA 51 study was designed specifically to deal with these issues (see above). The cost analysis compared conservative treatment with compression and standard surgery 24 months after randomization and included all NHS costs. Because of small numbers in the group, the results for sclerotherapy are less generalizable. The results are summarized in Table 3.
Total NHS discounted cost and QALY gain

QALY, quality-adjusted life-year
Although standard surgery was associated with a significantly greater cost, it also had a slightly greater cost per quality-adjusted life-year (QALY). Both economic analysis and modelling strongly suggested standard surgery for subjects in Group 3 (truncal varicose veins), there was a 70–80% certainty that the QALY was well below the £30,000 upper limit suggested for therapies in the NHS by the National Institute for Health and Clinical Excellence. It was concluded that for patients with truncal reflux associated with varicosities in the calf and thigh, surgical treatment offers a modest health benefit for a small additional NHS cost relative to conservative treatment.
Although data from Group 1 (minor veins and no truncal reflux) was not subjected to an economic analysis, modelling suggested that sclerotherapy resulted in a benefit of 0.044 QALY. This when adjusted yields a cost of £3500 per QALY. Similar analysis of patients in Group 2 suggested incremental QALY benefits of 0.046 and 0.214 for sclerotherapy and surgical intervention, respectively. This translates to £3388 and £2083 per QALY for sclerotherapy and surgery, respectively. If the calculations and assumptions are extended to surgical patients in Group 3, the cost per QALY becomes £1864.
Conclusions
Uncomplicated but symptomatic varicose veins remain a common health-care problem and are associated with reduced QoL. Without exception all interventions, regardless of their associated potential morbidity, considered thus far are efficacious and individually contribute to improved HRQoL. This is achieved at well within the target tariff set by the publicly funded health-care system in the UK. All interventions principally abolish truncal reflux and either remove or occlude the incompetent axial venous conduit. Modern endovenous techniques differ from standard surgery in that general anaesthesia is not required and they may be performed in settings other than standard operating theatres. In order to offer endovenous techniques, clinical evaluation must be combined with detailed non-invasive imaging. If only surgery is to be considered, the role of preoperative duplex imaging remains unclear. At present there appears to be some evidence, albeit of varying quality/grade, to suggest that the endovenous techniques are superior to surgery in terms of QoL improvement and future recurrence. Future randomized studies will hopefully clarify issues of effectiveness between treatment options and provide insight into cost-effectiveness in both the short and long term.
Footnotes
The author hereby declares no conflict of interests.