
Abstract
Objective
To describe the histopathological changes of the vein wall caused by bipolar radiofrequency-induced thermotherapy (RFITT), and to examine influence of power and application time on the histopathological changes.
Material and methods
Twenty vein specimens atraumatically extracted near the saphenofemoral junction were treated by RFITT ex vivo. RFITT was applied with fixed (2 seconds) and varied (up to an impedance of 400 Ω) application time and increasing power (5, 10, 15, 20, 25 W). Specimens were processed histologically.
Results
RFITT induced coagulation of collagen bundles, shrinking of muscles, splitting and necrosis of the vein wall. Circumferential necrosis of intima and media was reached by a power of 20–25 W and an application time up to an impedance of 400 Ω. Only heterogeneous necrosis of intima and media in parts of the vessel was reached by lower power with long application time.
Conclusion
A homogeneous necrosis of the circumferential vein wall needs high power and sufficient application time.
Introduction
The bipolar radiofrequency-induced thermotherapy (RFITT) has been successfully used for volume reduction in the nasal concha in otorhinolaryngology 1 and for the treatment of tumours in otorhinolaryngology, surgery and radiology. 2,3 Since the beginning of 2007 there has been an RFITT applicator for phlebological treatment of insufficient saphenous veins. 4
Technical principle of bipolar radiofrequency
At the tip of the catheter two electrodes are arranged in an in-line configuration and separated by an electrical insulator. According to the information of the manufacturer, a high-frequency alternating current flows from the first electrode through the venous wall to the second electrode. The alternating electric field forces the ions of the tissue to move. The kinetic energy of the ions is transformed into thermal energy directly within the vein wall (microwave-effect). The wall tissue between the poles is heated to 85–95°C, becomes dehydrated and starts shrinking. The thermal energy is not created by the applicator but is originated directly in the venous wall.
Due to dehydration, the electric resistance of the tissue increases. There is a feedback of the electrodes to the generator. The RFITT generator measures the electric resistance of the tissue. When an impedance of 400 Ω is reached, energy of the generator is switched off automatically.
Histological findings
Although multiple patients have already been treated by RFITT, systematic evaluation of histopathological changes of the treated vein walls induced by RFITT is missing. So far, there is only a single case reported of a woman who had a laser treatment before the RFITT 5 and experimental findings are obtained from animal studies. 6
Therefore, we initiated a monocentric ex vivo study to evaluate the histological changes of the vein wall caused by RFITT. As data of a current publication showed the influence of application time in clinical recurrence rates, 7 we examined the influence of power and of application time on the histopathological changes of the vein wall.
Patients and methods
Patients
Overall, 20 vein segments of 15 patients were included in the study. All patients had a study-independent, stage-according vascular surgery of the great saphenous vein. All patients gave their written consent for vascular surgery and for their participation in the study.
Procedures
A junctional part of the great saphenous vein with a length of 3–4 cm was carefully removed and immediately placed in physiological saline solution to avoid a dehydration of the material. Only a few minutes later the vein material laying on a dry compress was treated by RFITT.
RFITT was conducted by the CelonLab PRECISION generator and the flexible CelonProCurve 1200-S15 applicator (both Celon AG medical instruments, Teltow, Germany). The generator can deliver a power of 1–25 W and has a frequency of 470 kHz. Applied energy per cm vein segment increases linearly depending on retraction speed and power (e.g. 20 W and 0.5 cm/second = 40 J/cm, 25 W and 0.5 cm/second = 50 W). The catheter has a diameter of 1.8 mm and a length of 1200 mm. The length of the electrode is 15 mm.
The vein segments were allocated consecutively to the treatment procedures (Table 1). The parameters of the therapy varied according to the protocol. Respectively, two specimens were treated in the use of the same parameters: in 10 specimens a fixed application time of two seconds was provided. In 10 specimens the application time was left open up to the 400 Ω shut-off (Table 1). The fixed application time of two seconds was chosen according to the preliminary available clinical results and the proposals of the manufacturer (1–2 seconds/cm). 8 Every specimen was treated once. There was no re-treatment of the vein segment in the ex vivo experiment.
Parameters of the study
Respectively two specimens were treated with the same parameters of power and application time
The experiments were carried out at room temperature, around 20°C. There was no control of temperature in the tissue around the vein during the experiments.
Afterwards, the vein material was histologically processed. The specimens were transversally cut and stained with haematoxylin–eosin (HE) and Van-Gieson (VG). The slides were surveyed with light microscopy in 10-fold to 100-fold magnification (Olympus BX51, Hamburg, Germany). Especially the extent of the RFITT-induced necrosis was surveyed. The spreading of the necrosis (isolated necrotic spots, narrow or wide necrotic zones, diffuse necrobiosis of the whole vein wall), the minimal and maximal extent of the necrosis (absolute and in correlation to the vein wall) and the minimum and maximum diameters of the venous lumen were determined. Measurements were done with a special ocular for measurements in dermatohistopathology, e.g. to define the depths of melanoma.
Ethics
The study protocol complies with the ethical rules for human experimentation stated in the 1975 Declaration of Helsinki and was approved by the ethics committee of the Ruhr-University Bochum (Vote No. 3243-08).
Statistics
The evaluation of the data was done descriptively. Given values are calculated as the mean of the analysed groups. The t-test for related samples was used to calculate the difference between the vein lumen before and after treatment in the 20 specimens. A P ≤ 0.05 was regarded as statistically significant.
Results
Basic data of the patients
Fifteen patients (12 women, 3 men; aged 56.5 ± 13 years) with primary varicosis of the great saphenous vein in 20 legs were included in the study. The diameter of the great saphenous vein before the surgical intervention was measured using duplex sonography with the patient in standing position. The junctional diameter of the great saphenous vein had an average of 10.1 ± 1.7 mm.
Basic data of the vein specimens
Overall, 20 specimens were surveyed. The thickness of the vein wall (intima + media) had a mean diameter of 1 ± 0.2 mm and varied between a minimum of 0.2 mm and a maximum of 1.6 mm. In some cases, extensive differences of the diameter of the vein wall were seen.
The diameter of the vein lumen, before treatment in vivo (measured by duplex sonography) and after treatment and histological processing ex vivo (measured at the specimen), decreased significantly from 10.1 ± 1.7 to 2.7 ± 2.0 mm (P < 0.01).
Histopathology after RFITT
Low power
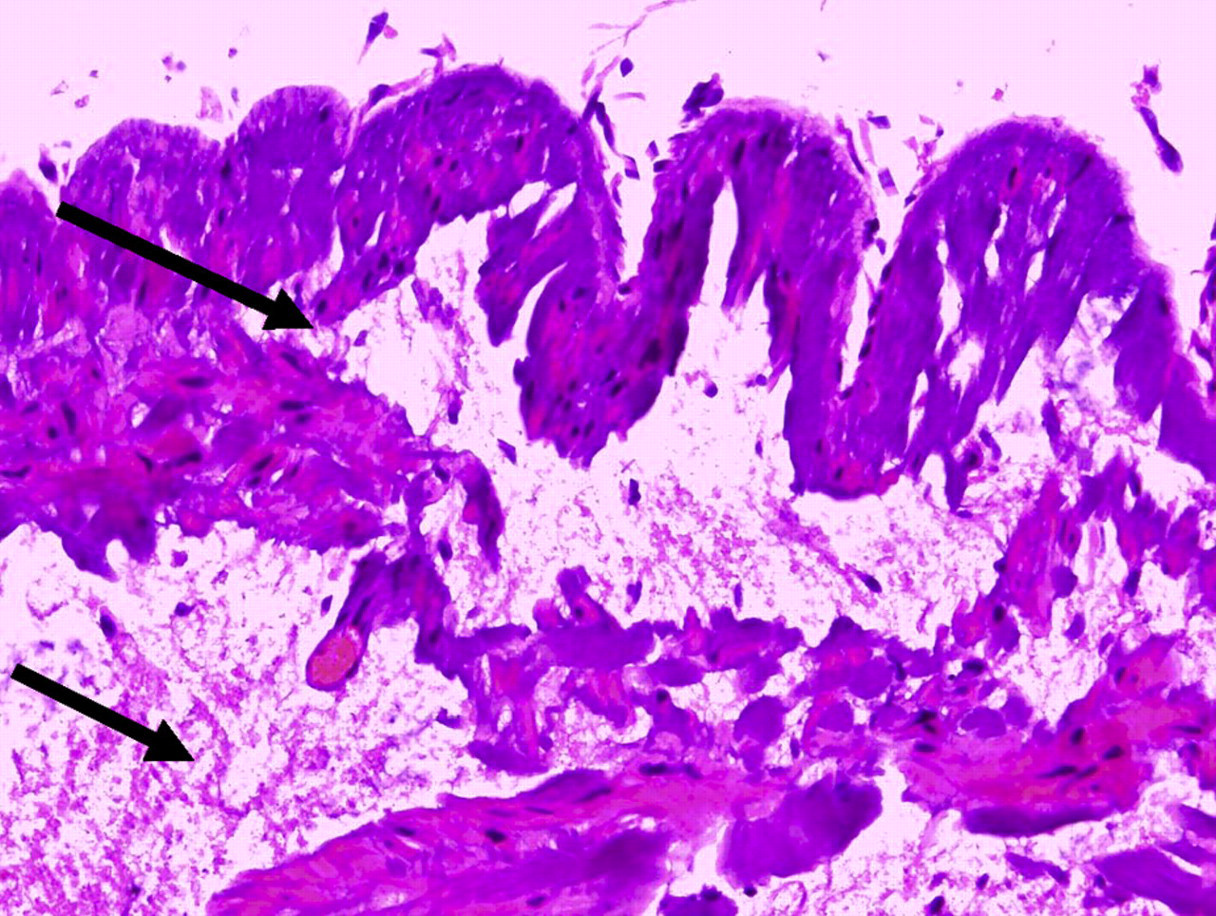
In application of low power (5 W) and an application time up to an impedance of 400 Ω with an average application time of 20 seconds, a heterogeneous extent of necrosis and clefts were seen (Figure 1). In parts of the vein wall necrosis reached the media. Other parts just had a necrosis of the endothelium.

Low power (5 W) and an application time to an impedance of 400 Ω heterogeneous extent of necrosis and clefts: more basophilic coagulation of collagen and clefts on the left than on the right half of the specimen (details of intima and media, haematoxylin–eosin stain, original magnification ×40)
Medium power
In application of medium power (15 W) and an application time up to an impedance of 400 Ω, tissue alteration reached the intima and the media. Clefts between intima and media and within the media were detectable (Figure 2). The changes were irregular and heterogeneous, and did not include the whole circumference of the vessel.
Medium power (15 W) and application time to an impedance of 400 Ω: clefts between intima and media, and within the media (arrows) (details from intima and media, haematoxylin–eosin stain, original magnification ×40)
High power
Application of high power (25 W) with a short application time (<2 seconds) induced a circumferential and homogeneous necrosis of the endothelium. But in some parts there was no alteration of the subendothelial tissue (Figure 3).
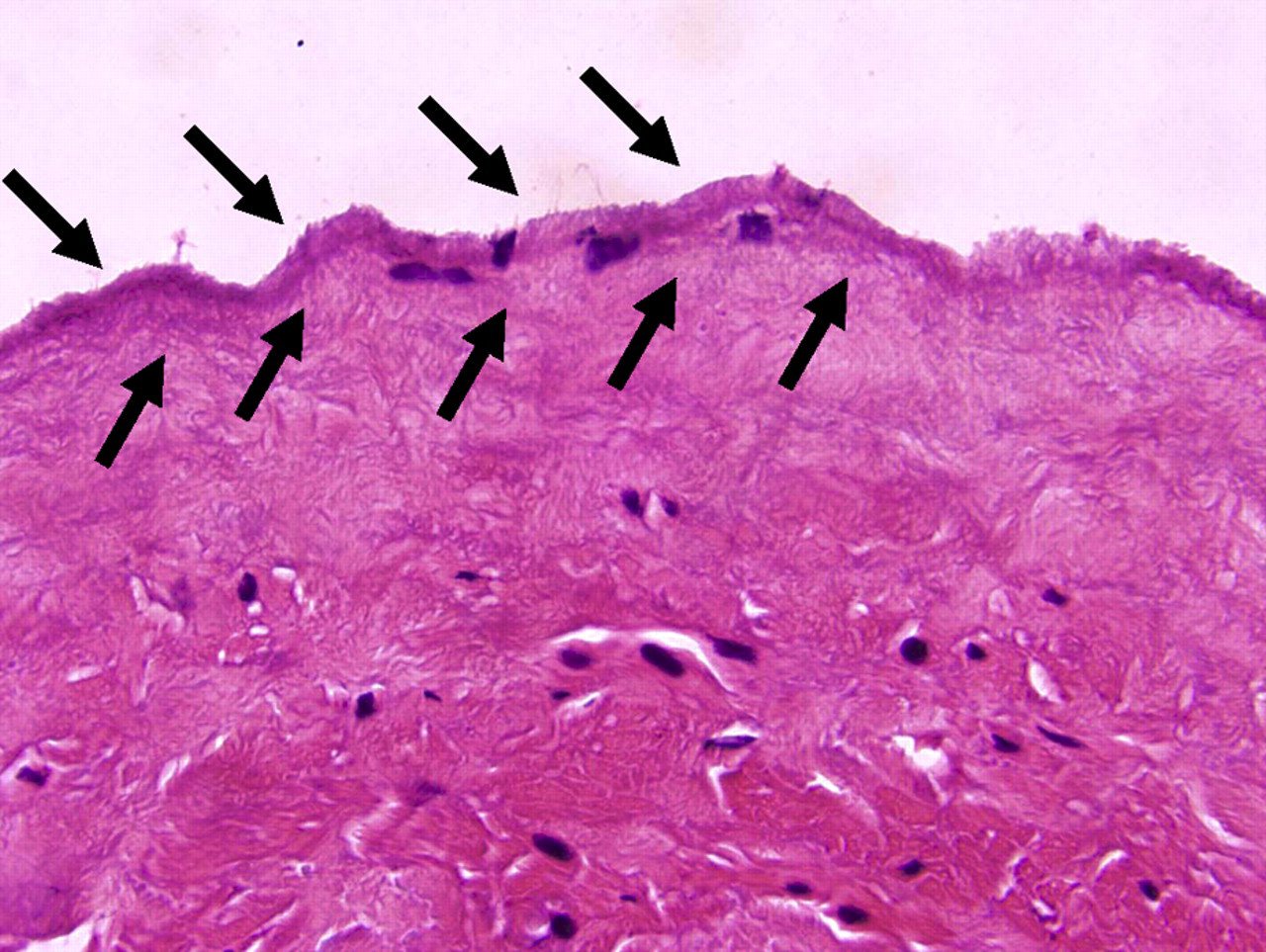
High power (25 W) and short application time (2 seconds): only a necrosis of the endothelium (arrows) but no alteration of subendothelial tissue could be seen (details from the intima, haematoxylin–eosin stain, original magnification ×100)
In use of high power (20 W) with an application time up to an impedance of 400 Ω, a widespread necrosis of the entire intima and media was detectable as well as a coagulation of collagen bundles (Figure 4). Furthermore, there was a shrinking of muscle cells that led to clefts (Figure 5).
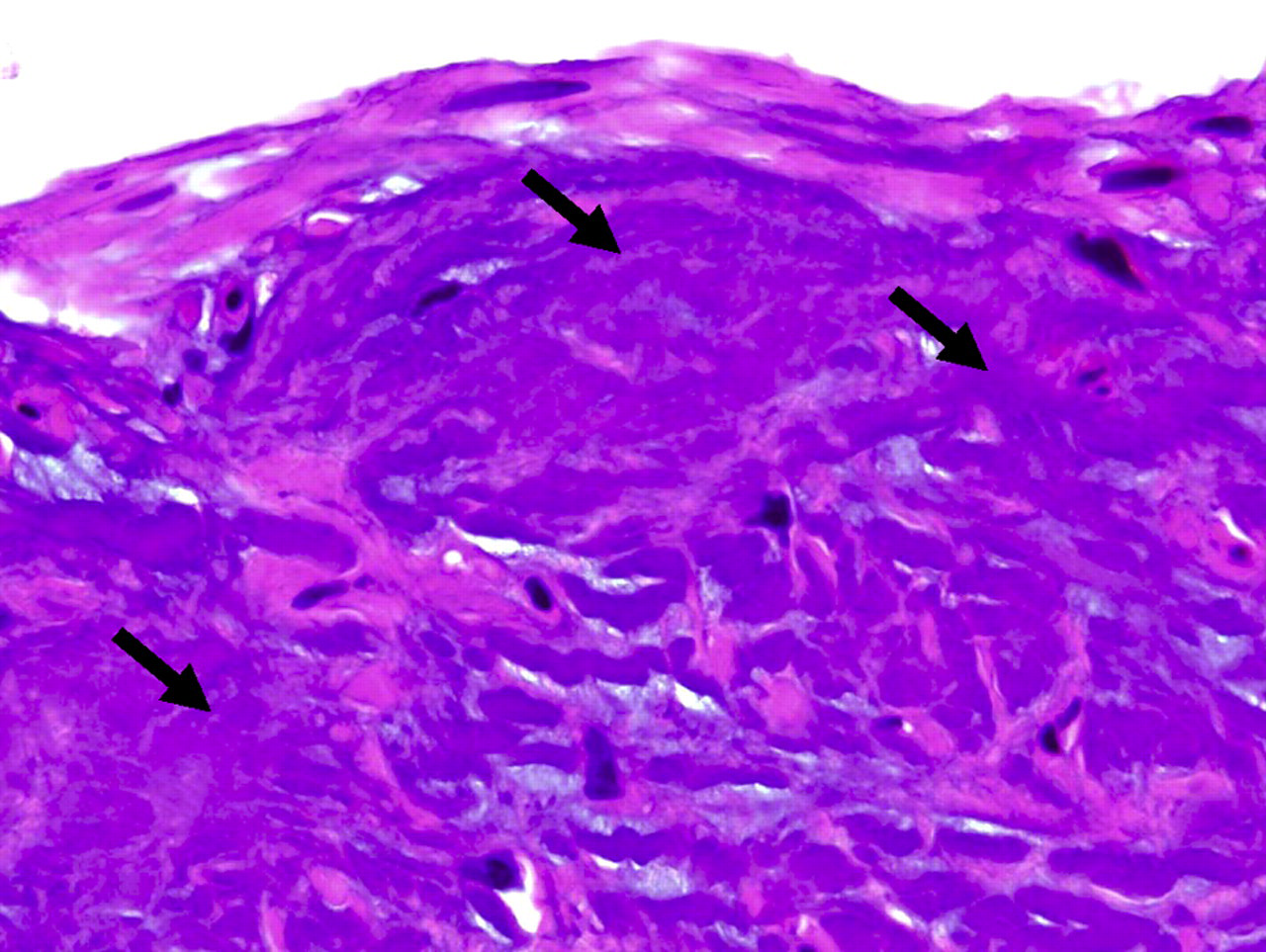
High power (20 W) and application to an impedance of 400 Ω: coagulation of collagen bundles (arrows) and widespread necrosis of the entire intima and inner media (details from the intima, haematoxylin–eosin stain, original magnification ×100)

High power (20 W) and an application time to an impedance of 400 Ω: coagulation of collagen bundles (upper arrow), shrinking of muscle cells and clefts (lower arrow) (details from the media, E Van-Gieson stain, original magnification ×100)
Influence of time
The data show that the extent of the necrosis induced by RFITT depends on both the applied power and the application time. In use of short application of RFITT in spite of high power, only heterogeneous necrosis can be induced. But if application time is extended up to a tissue impedance of 400 Ω, a heterogeneous and circumferential alteration of tissue is possible.
In increase of the applied power, the application time to reach the 400 Ω shut-off decreased (Figure 6). While in lower power levels longer application time with an average of 20 seconds was necessary to reach the 400 Ω, in higher power levels an application time of 2–3 seconds was sufficient (Figure 6). Here, in spite of the short application time, a homogeneous, circular necrosis was seen.

Application time to reach the 400 Ω varied according to the applied power. Given values are calculated as an average of the two specimens treated at each power level
An increasing power and application time led to an increasing necrosis of the vein wall. While in use of a fixed application time up to two seconds with a power of 5–15 W, a small zone of intima and media could be damaged (5 W 0%, 10 W 0.5% and 15 W 2.5%), a power of 20–25 W induced necrosis of 50–100% of the intima and media layer. In use of variable application time up to a resistance of 400 Ω, the extent of necrosis of the intima and media was higher even in application of lower power (10 W 20%, 15 W 30%, 20 W 60%).
Discussion
This pilot study shows that the necrosis of the intima and media was reached especially by the use of high power at 20 and 25 W (extent of necrosis 50–100% of the intima and media layer). A further modification of the application time up to a resistance of 400 Ω (varying with the applied power) allows an increase of the homogeneity of the necrosis. A perforation of the vein wall was not seen in any of the specimens, not even in the use of high power (25 W).
In our study we had veins with a wide variety of vein wall diameter, even with enormous differences within one specimen (0.2–1.6 mm). From the literature it is known that vein walls can be very heterogeneous. Neovascularization can consist of parts with aneurysms or parts that consist of just an endothelial tube. 9,10 According to those findings, a targeted application of energy is necessary. The applied energy has to be chosen so as to reach a sufficient alteration of the full thickness of the wall but to avoid a perforation of the vein.
What is different in the ex vivo experiment compared with the in vivo situation? It is necessary to consider the following aspects:
The ex vivo diameter of the vein is probably wider than in vivo. In vivo vein diameter can be decreased via tumescent anaesthesia, compression by the hand of the therapist or vasospasm evoked by the catheter. Therefore, in vivo a better conduction of electricity with a more intense effect can be assumed;
In vivo the vessel is filled with blood. The blood is included in the conduction of the electricity resulting in coagulation. In contrast, the specimens of our ex vivo experiment are not filled with blood and had been embedded in physiological saline solution before being treated with RFITT. While the saline solution is not coagulated by the electricity but evokes a further moisture penetration of the treated tissue, that is not possible for the coagulated blood in vivo. Probably, the increase of the resistance of the specimen ex vivo is slowed up by the bedding of the vein in the saline solution. Therefore, the optimum application time in vivo is shorter than the periods measured in the ex vivo experiment. According to our own clinical experiences in vivo an application time of about 3 seconds/cm with a power of 20–25 W provokes a sufficient obliteration of the vessel. Zierau and Lahl
5,11
proposed a power of 18 W and an application period of 3–4 seconds/cm as optimum for a long-term obliteration of the vein; The histological post-treatment diameter (2.7 ± 2.0 mm) is significantly minor to the pretreatment duplex controlled lumen diameter of the varicose vein (10.1 ± 1.7 mm). The essential mechanism of action for the reduction of the vein lumen is via RFITT-induced contraction of the vein wall. According to animal studies of Burgmeier et al.
12
the shrinking of the collagen of the vein wall depends on the applied power and the time of treatment. Additionally, it has to be recognized that the histological specimens are influenced by different contraction processes. But especially the RFITT-induced shrinking of the vein wall with a reduction of the lumen is an intended phenomenon. The histological preparation (e.g. bedding in formalin, dehydration) led to a further unintentional shrinking of the specimen with a maximum of just 20–25% reduction;
13
Furthermore it has to be recognized that the temperature of the surrounding of the vein was much lower in the ex vivo experiment than in vivo. The experiment was carried out at room temperature of about 20°C, in vivo the temperature was between 36 and 37°C. It can be assumed that in vivo the time to reach the 400 Ω can therefore be reached earlier than ex vivo.
As seen in the results, a lower power and short application time is only able to induce heterogeneous necrosis including parts of intima and media. Here, it can be assumed that in an in vivo setting, recanalization would be possible as the vein wall is not completely damaged. While a circumferential and homogeneous necrosis of the intima and media seems to be finally destroyed. The character and the extent of the necrosis ex vivo at power levels of 20–25 W and the very short application time in vivo (1–2 second/cm) probably provide a sufficient obliteration of the vessel – even in long-term follow-up. A re-naturation of the symmetric, homogeneous and circular damaged vein wall seems to be unlikely.
Up to now, there are no clinical long-term results of the initially referred multicentre study. 4,14 Intermediate results after a follow-up of 133 days revealed a complete obliteration of the vessel in 88.8%. 7 First results of a 12-month follow-up after a modification of the application parameters (18 W, 3.4 second/cm) showed a success rate of 97.6%. 5 The higher rates of recurrence in the study of Camci et al. 7 are probably due to the short application times they used. In the study of Zierau et al. 5 application time was elongated.
Conclusion
In conclusion, data of the pilot study shows that RFITT induces:
coagulation of collagen bundles; shrinking of muscles; splitting of the vein wall; necrosis of the vein wall.
For a circumferential necrosis including the full thickness of the intima and media, not only is a high power of 20–25 W necessary but also a sufficient application time up to a resistance of 400 Ω. The feedback mechanism of RFITT allows a safe application of energy and protects against an overheating or perforation of the vein wall also in use of high power. A circumferential and homogeneous destruction of the intima and media may decrease the risk for a recurrence of the varicose vein.