
Abstract
The clinical venous anatomy of the pelvis and its veins featured a break-through during the past few years. Not only the diagnostic and therapeutical methods but also the knowledge of the functional anatomy and nomenclatures of the veins underwent substantial changes. Eleven years ago, the most recent revision of the Latin anatomical nomenclature, Terminologia Anatomica (TA, 1998) was issued. In 2004, during the 21st World Congress of the International Union of Angiology, a consensus document (under the auspices of Federative International Committee on Anatomical Terminology and International Federation of Associations of Anatomists), reflecting phlebologists' requests for new terms and replacing several insufficient ones, was accepted. Six new terms were added in both Latin and English languages in the chapter concerning the veins of the pelvis. Eponyms are not considered equal synonyms and moreover only one of them was recommended for general use. Detailed anatomy of the veins of the pelvis is discussed. This consensus document will be incorporated in the next version of the Teminologia Anatomica.
Introduction
This article, extending the information on the superficial venous system of the lower limb, 1 concentrates on the veins of the pelvis, their precise anatomy and new nomenclature terms introduced in the last few years. The latest revision of the anatomical nomenclature (official in the Latin language only) was published by the Federative Committee on Anatomical Terminology (FCAT) in 1998 as the Terminologia Anatomica (TA), subtitled International Anatomical Terminology. 2 The Latin terms valid according to TA, used in this article, are written in italics. The old and invalid terms, used in this article, are written within quotation marks without italics and the English terms follow in brackets. Synonyms are separated (according to the TA pattern) with semi-colon. The English terms are only equivalents commonly used in the English-speaking countries. 3,4
The vehement development of diagnostic and therapeutic methods, together with the introduction of the clinical, aetiological, anatomical and pathological elements classification, brought the requirements for improvement of the anatomical knowledge of veins nomenclature. 5 In 2001, the presidents of the International Union of Phlebology (IUP) and International Federation of the Associations of Anatomists (IFAA) nominated an International Interdisciplinary Committee to revise the nomenclature of the veins of the lower extremity. At its second meeting, on 23 May 2004 (in Rome), within the extent of the 21st World Congress of the International Union of Angiology under the supervision of IUP, IFAA and Federative International Committee on Anatomical Terminology (FICAT), the committee prepared a document, focused on the veins of the pelvis and terms from everyday clinical practice, named ‘International Interdisciplinary Consensus Committee on Venous Anatomical Terminology: Nomenclature of the Veins of the Lower Limb: Extensions, Refinements, and Clinical Application’. 6 Several terms in TA were substituted by new ones, some until then unnamed terms acquired new denominations, derived from their anatomy, topography and their clinical importance. Eponyms are not considered equal synonyms and moreover only one of them was recommended for general use. The document was then approved by FICAT and will be incorporated in the future revision of the Terminologia Anatomica. 6–9
Veins of the pelvis
The veins of the pelvis are interconnected with the superficial venous system of the lower extremity both via pudendal, sciatic and gluteal perforating veins (venae perforantes pudendales, ischiadici et gluteales) and mainly with the deep venous system by several routes. Their anatomy is very complex and a bit difficult to understand because of the presence of venous plexuses of various extent, volume, size and communications. The nomenclature of certain pelvic veins has been reviewed and specified as summarized in Table 1.
Nomenclature of the pelvic veins of the lower limb according to TA 1998 (terms with the Identification number) and according to the Consesus Documents 2004
The bold copies the bold in Terminologia Anatomica emphasising the principal veins in the chapter ‘Cardiovascular System’ 2
The classification of the pelvic veins is not a simple and clear matter and that is why they are listed in the following paragraphs according to their draining area and direction of the blood flow, completed with the information on their exact position, course, tributaries and termination. Most of the blood is collected by the common iliac veins, the rest by the gonadal veins, ascending lumbar veins (and azygos/hemiazygos), vertebral plexuses and veins of the abdominal wall.
Drainage area of the common iliac veins
Common iliac vein (vena iliaca communis)
This largest vein of the pelvis commences with the junction of the internal and external iliac vein which is situated in front of the sacroiliac joint (Figure 1). The vein ascends towards the right side of the fifth lumbar vertebra where it fuses with the contralateral vein in an acute angle and together they form the unpaired inferior vena cava (vena cava inferior). The right-sided common iliac vein is shorter, having almost perpendicular course, and ascends dorsally and laterally to the right common iliac artery. It crosses the obturatory nerve (nervus obturatorius) and lumbosacral trunk (truncus lumbosacralis) ventrally. The left-sided vein is longer, featuring more oblique course, and runs medially and later dorsally to the left common iliac artery. It passes (dorsally) behind the sigmoid mesocolon (mesocolon sigmoideum) and superior rectal vessels (vasa rectalia superiora). Both veins do not usually contain any valves. Caggiati stated that a functionless valve can be present in 1–7% of cases; LePage reported 1.2% occurrence on the right side. 10,11 The left-sided veins can be compressed by the course of the right common iliac artery. This ‘locus minoris resistentiae’ is a possible site for the development of thrombosis (Figure 2). This condition is then denominated as the May-Thurner syndrome (one type of the Cockett syndrome or iliac vein compression syndrome).

Ultrasound image of the veins of pelvis. VIC, vena iliaca communis; VIE, vena iliaca interna
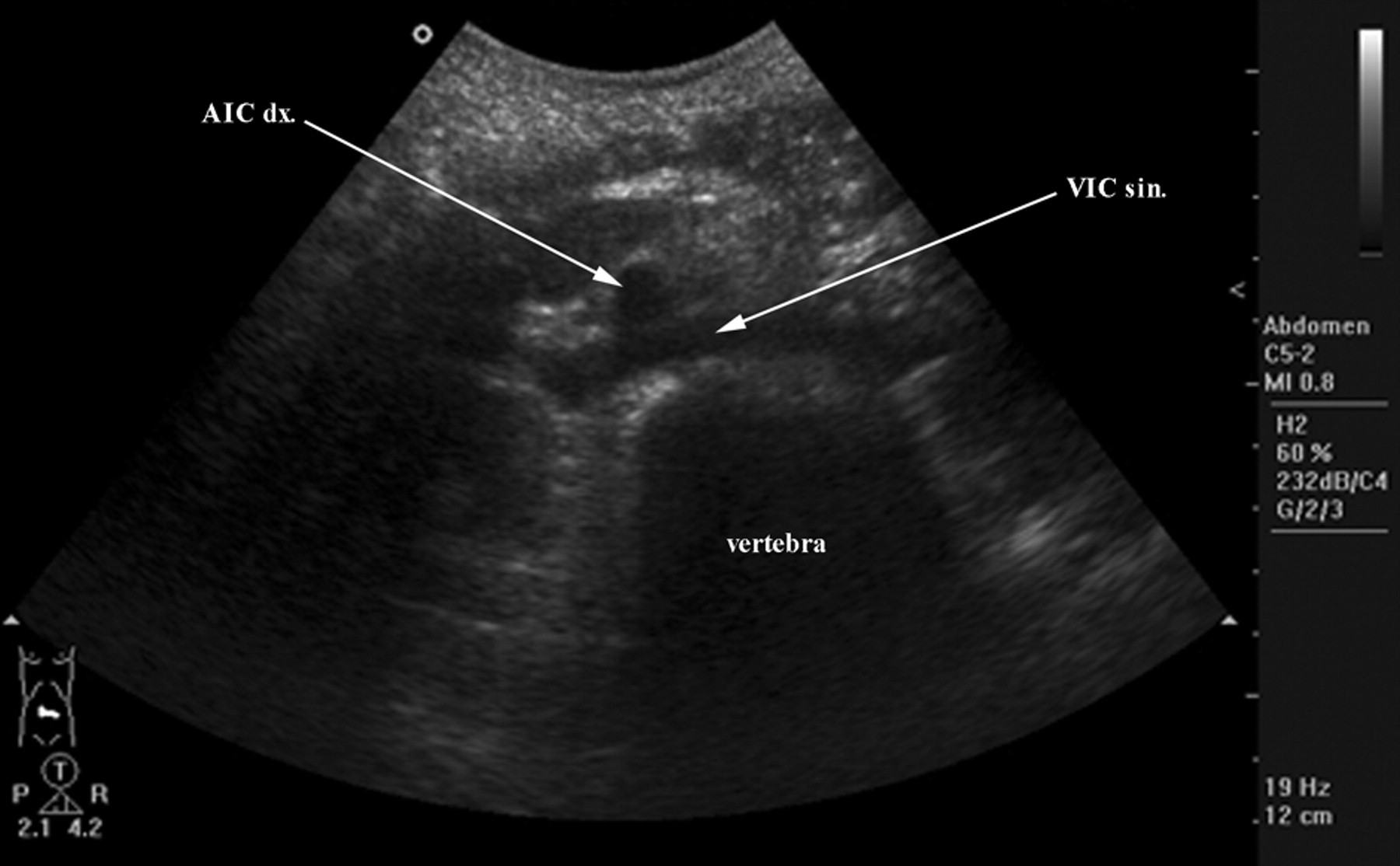
Ultrasound image of the veins of pelvis – the left common iliac vein can be compressed by the right common iliac artery (the site of thrombosis in the May-Thurner syndrome). AIC dx, arteria iliaca communis dextra; VIC sin, vena iliaca communis sinistra
The common iliac veins receive:
1a –
1b –
1c – Sometimes the
1d – Median sacral vein (vena sacralis mediana).
One or more veins accompanying the median sacral artery usually terminate into the left common iliac vein, less often directly into the lower margin of the confluence of both common iliac veins. The vein drains the anterior aspect of the sacral bone, has a wide connection to the sacral venous plexus (plexus venosus sacralis) and is regularly found as doubled (reported in 80% by Bacque). 12
External iliac vein (vena iliaca externa)
This vessel is a proximal continuation of the common femoral vein, located cranially to the vascular space (lacuna vasorum). It ascends along the arcuate line (linea arcuata), forming the brim of the lesser pelvis, and terminates in front of the sacroiliac joint by the confluence with the internal iliac vein (vena iliaca interna) from which the blood flows by the common iliac vein. The right-sided vein is located medially to the external iliac artery and successively it moves dorsally to it. The left-sided one is situated medially to the artery in its whole course. The vein is crossed ventrally and medially by the ureter (on the left side only) and the internal iliac artery and is covered with the parietal peritoneum. Further caudally, in men it is ventrally crossed by the ductus deferens, in women by the ovarian vessels (vasa ovarica) and the round ligament of the uterus (ligamentum teres uteri). Laterally to the vein, there is the psoas major (musculus psoas major) situated. There are usually no valves inside the vein, one is reported in 25–35% of cases (but frequently functionless), usually situated within 2 cm distally to the termination of the external iliac vein. 10,11 At the beginning, the vein receives two larger extrapelvic tributaries – deep circumflex iliac vein and inferior epigastric vein.
2a –
It collects venous blood from the lateral and inferior margin of the iliac fossa and empties into the external iliac veins approximately 2 cm proximally to the inguinal ligament. There is large communication with the tributaries of the iliolumbar veins and veins of the anterior abdominal wall. 13
2a –
This vein (often used as a part of the pedicle for muscular and musculo-cutaneous flaps in plastic surgery) drains into the external iliac vein approximately 1.25 cm proximally to the inguinal ligament and collects the blood from the lower half of the rectus abdominis (musuclus rectus abdominis), its sheath and the anterior abdominal wall. It is doubled in its peripheral segment and both trunks unite in different distances before the termination. In the muscle, it richly anastomoses with the superior epigastric vein – this route can serve as a cavo-caval anastomosis. 13
Inferior epigastric veins receive the venous blood from two systems of small veins: pubic veins (see below 3Ad1) and suprapubic veins.
These small veins form a system in the hypogastric (pubic) region of the anterior abdominal wall and serve as a communication between the left and right inferior epigastric vein. They are situated within all layers of the anterior abdominal wall: epifascially, subfascially in the abdominal muscles and between them and interfascially, i.e. beneath the thick layer of the condensed subcutaneous connective tissue, called erroneously Scarpa's fascia or subcutaneous abdominal fascia and correctly membranous layer (stratum membranosum telae subcutaneae abdominis) – this space corresponds to the saphenous compartment (compartimentum saphenum) of the lower limb. 1
Internal iliac vein (vena iliaca interna)
This complex vein originates at the greater sciatic foramen (foramen ischiadicum majus), usually as a confluence of the inferior gluteal vein and internal pudendal vein. It ascends posterolaterally to the corresponding artery and joins the external iliac vein to form the common iliac one. It can be duplicated in up to 30% of cases – then one trunk receives blood from the visceral tributaries and the other from the parietal ones (reflecting the arrangement of the internal iliac artery branching pattern) – or forms a network of more vessels (in 20% of cases). 11,12 As for the valves, the literary data are unreliable and inconsistent, ranking from the avalvular state as far as 40% presence in the right-sided internal iliac vein. 11,14 The same discrepancies are reported concerning the branches of the internal iliac vein as well: Kampmeier considered all tributaries as avalvular; on the contrary, LePage observed the valves at the estuaries of the tributaries in 7.6% and within their course in only 2.5% of cases (valves are present in only 10.1% of all internal iliac veins). 11,14 As for the tributaries, the estuary valves (‘ostial valves, terminal valves’) were reported in 4.9% and within their course (‘parietal valves’) in 4.2% of the specimens (total incidence thus being 9.1% of cases). 11
The internal iliac vein receives many vessels that can be classified into three different groups (3A, 3B, 3C). The first group covers vessels originating outside the lesser pelvis:
3Aa –
They drain the upper part of the gluteal muscles (they are considered as parietal tributaries), accompany the corresponding artery and enter the lesser pelvis via the suprapiriform foramen (foramen suprapiriforme), usually terminating in the internal iliac vein as one trunk.
3Ab –
These veins, again considered as parietal, run along the corresponding artery and originate in the proximal part of the posterior surface of the thigh as the sciatic vein (vena ischiadica) where they anastomose with the tributaries of the medial circumflex femoral veins (venae circumflexae femoris mediales) and first deep femoral communicating vein (accompanying veins of perforating arteries; vena comitans arteriae perforantis primae). The inferior gluteal veins enter the lesser pelvis through the infrapiriform foramen (foramen infrapiriforme) and unite into one trunk which drains into the beginning of the internal iliac vein. They feature multiple communications with the superficial veins of the gluteal region, arranged into three groups and denominated as gluteal perforating veins (venae perforantes gluteales). They serve as possible collaterals between the femoral and internal iliac vein draining areas.
3Ac –
They originate in the ischio-anal fossa (fossa ischioanalis) from:
3Ac1 – Deep veins of penis ♂/of clitoris ♀ (venae profundae penis ♂/clitoridis ♀)
Then the internal pudendal veins receive:
3Ac2 – Veins of bulb of penis ♂/of clitoris ♀ (venae bulbi penis ♂/clitoridis ♀);
3Ac3 – Posterior scrotal ♂/labial ♀ veins (venae scrotales ♂/labiales ♀ posteriores);
3Ac4 – Perineal veins (venae perineales);
3Ac5 – Inferior rectal veins (venae rectales inferiores);
3Ac5 – Sometimes the deep dorsal vein of penis ♂/of clitoris ♀ (vena dorsalis profunda penis ♂/clitoridis ♀).
The internal pudendal veins communicate with the prostatic venous plexus (plexus venosus prostaticus). They accompany the corresponding artery and run together dorsomedially with the pudendal nerve (nervus pudendus) through the pudendal canal of Alcock (canalis pudendalis), pass the lesser sciatic foramen (foramen ischiadicum minus), turn around the sciatic spine (spina ischiadica) and enter the lesser pelvis via the infrapiriform foramen (foramen infrapiriforme). There they unite into one trunk and form the origin of the internal iliac vein. 13
3Ad –
This parietal vein originates within the proximal portion of the medial group of thigh muscles, enters the lesser pelvis through the obturator canal (canalis obturatorius), together with the corresponding artery and nerve, and runs dorsocranially, along the lateral wall of the pelvis, covered by the artery. Further centrally, it is situated between the ureter and internal iliac artery and empties into the proximal segment of the internal iliac vein. In some cases, it may be replaced with a widened pubic vein or pubic branch (vena pubica, ramus pubicus), which conveys blood into the external iliac vein. Then it is termed the accessory obturator vein (vena obturatoria accessoria). It has important communications in the proximal part of the thigh with the circumflex femoral veins (vena circumflexa femoris medialis et lateralis).
3Ad1 –
One or more veins located on the posterior surface of the pubic bone. The vein usually branches from the obturator vein just after it emerges from the obturator canal, ascends and traverses the superior pubic ramus (ramus superior ossis pubis) in the distance of 39–82 mm from the pubic symphysis (symphysis pubica) and joins the pubic ramus (pubic tributary) of the inferior epigastric vein, which is then used as a canal to lead the venous blood into the external iliac vein. It is present in 52–96% of cases. It is accompanied by a less frequent arterial communication, called ‘corona mortis of Hesselbach’ by clinicians (present in 8–43% of cases). Anatomically it is an anastomosis between the pubic branches of the obturator and inferior epigastric arteries (rami pubici arteriae obturatoriae et arteriae epigastricae inferioris) or the so-called aberrant or aberrant accessory obturator artery (arteria obturatoria aberrans or arteria obturatoria aberrans accessoria), emptying into the trunk of the external iliac vein. Percentage data concerning the venous and arterial communications differ in various studies but, generally, the venous one is present in almost every patient and the arterial one is much rarer. Their clinical importance resides in the possible danger of the fatal bleeding in surgical procedures of the femoral hernias, anterior approach to the acetabulum, fractures of the superior pubic ramus or complicated deliveries. 15–17
3B – The second group of internal iliac vein tributaries comprises the parietal veins of the walls of the lesser pelvis:
3Ba –
These veins accompany the corresponding arteries and convey blood from the sacral venous plexus into proximal segment of the internal iliac vein.
3Bb –
A venous plexus located in the loose connective tissue behind the rectum and in front of the sacral bone is embedded into the parietal layer of the pelvic fascia. It collects blood from:
3Bb1 – Spinal veins (venae spinales) that originate from the cauda equina of the spinal cord and traverse the anterior sacral foramina (foramina sacralia anteriora). They receive blood from the anterior surface of the sacral bone, anterior branches of spinal nerves (forming the sacral plexus) and from the interfascial spaces between the posterior aspect of the rectum and anterior aspect of the sacral bone.
Drainage from the sacral venous plexus is assured in three directions:
By means of the median sacral vein into the left common iliac vein; Via the iliolumbar vein into the common iliac vein; Mainly through the lateral sacral vein into the internal iliac vein.
The spatial arrangement of the plexus is hexagonal in the upper half (in 83%) and ladder-like in the lower one (in 90%), being drained prevailingly into the sacral lateral veins.
Communications: ventrally into the organ (visceral) plexuses, principally around the rectum and dorsally via the anterior sacral foramens into the vertebral venous plexuses (plexus venosi vertebrales; plexus of Batson), being valveless, which can serve either as a possible route of the cavo-caval anastomosis or as a channel for spreading of the metastatic cells and inflammation. 12,18
For an anterolateral view of main parietal pelvic veins (Figure 3).

Drawing of the parietal veins of pelvis (anterolateral view). VCI, vena cava inferior; VCIP, vena circumflexa ilium profunda; VEI, vena epigastrica inferior; VFC, vena femoralis communis; VGI, vena glutea inferior; VGS, vena glutea superior; VI, vena iliolumbalis; VICdx., vena iliaca communis dextra; VICsin., vena iliaca communis sinistra; VIEdx., vena iliaca externa dextra; VIIdx., vena iliaca interna dextra; VIIsin., vena iliaca interna sinistra; VL4, vena lumbalis quarta; VO, vena obturatoria; VPI, vena pudenda interna; VvSL, venae sacrales laterales; VScM, vena sacralis mediana
3C – The third (last) group of tributaries originates from the venous plexuses of the pelvic organs (they are considered visceral tributaries). The pelvic venous plexuses are extensive mutually connected systems and the classification into visceral and parietal is purely arbitrary. They are listed in the dorsoventral direction as present in the female pelvis, completed with the relevant male venous structures:
3Ca –
The rectum is equipped with a huge venous plexus situated in two layers of the organ – the first one is embedded within the adventitia (plexus venosus rectalis externus), the other one is located in the submucosa (plexus venosus rectalis internus), which is denominated as the haemorrhoidal plexus (plexus haemorrhoidalis) as well. The internal plexus is formed in the area of the anal canal (canalis analis) in longitudinal extensions, presents a series of dilated pouches that are arranged in a circle around the tube, immediately above the anus and are interconnected by transverse circles, situated directly above the anal valves (valvulae anales). The most prominent ones are observed during the rectoscopic examination at numbers 3, 7, 11. The function of the rectal venous plexuses is irreplaceable for the faeces continence.
Drainage for the rectal plexuses is assured in three directions:
Most of the blood from the internal plexus flows cranially via the superior rectal veins (venae rectales superiores) to the inferior mesenteric vein (vena mesenteria inferior) and further to the portal vein (vena portae); The blood from the anal canal is emptied through the middle rectal veins (venae rectales mediae) and mainly through the inferior ones (venae rectales inferiores), by means of the internal pudendal vein, internal iliac vein, common iliac vein and finally inferior vena cava. The communication between the network of the portal vein and inferior vena cava can serve as a porto-caval anastomosis in pathological states, e.g. portal hypertension.
Communications: The external rectal plexus encompassing the rectum is connected ventrally with the vesical ♂/uterine and vaginal ♀ venous plexus (plexus venosus vesicalis ♂/uterinus et vaginalis ♀).
6
3Ca1 –
The term haemorrhoidal is reserved for the internal rectal plexus only according to its physiologically dilated arrangement (see Table 1).
This term designates the veins usually not originating directly from the external rectal plexus, but draining the blood from the surrounding organs (urinary bladder, prostate, seminal glands, uterus, vagina, pelvic floor); however, they feature multiple anastomoses with the rectal venous plexuses.
3Cb –
This plexus is located on the lateral sides of the vagina (within the so-called ‘mesokolpium’, which is rather hard tissue composed of the connective tissue, smooth muscle cells, vessels, nerves and lymph nodes).
3Ca1 – Paired
Communications: The vaginal plexus has multiple connections ventrally to the vesical plexus and dorsally to the rectal plexus and is continuous cranially with the uterine one – both plexuses (plexus venosus uterinus et plexus venosus vaginalis) serve as huge collateral for drainage of the blood from the lower extremity. They feature rich anastomoses with pubic, obturator, suprapubic, inferior epigastric and deep circumflex iliac veins.
3Cc –
Uterine plexus is situated laterally within the broad ligament of the uterus (ligamentum latum uteri). It concentrates the venous blood from the uterus, the broad ligament, the medial part of uterine tube (tuba uterina) and ovary, and it is drained mainly by the uterine veins.
Communications: Cranially along the ligament of ovary (ligamentum ovarii proprium), broad ligament of the uterus and mesovarium with ovarian veins; caudally with the related vaginal plexus (plexus venosus vaginalis). There are minor communications ventrally to the vesical plexus (along the vesicouterine ligaments – ligamenta vesicouterina) and dorsally to the external rectal plexus (along the rectouterine ligaments – ligamenta rectouterina).
3Cc1 – Paired
3Cc2 –
3Cc3 –
3Cd –
Larger venous plexus surrounding the lower part of the urinary bladder and in men the base of prostate, too. The blood is emptied by several vesical veins (venae vesicales), which usually unite into one common trunk (vena vesicalis) terminating into the internal iliac vein.
Communications: It anastomoses with the prostatic ♂/vaginal ♀ plexus (plexus prostaticus ♂/vaginalis ♀).
3Ce –
This term denominates the venous plexus situated behind the inferior pubic ligament and lower part of the pubic symphysis and in front of the urinary bladder and prostate, on its anterior and inferolateral surfaces, i.e. within the retropubic space (spatium retropubicum, space of Retzius, obsoletely spatium prevesicale), which is filled with the loose connective tissue only.
The main tributary of the pudendal plexus is the deep dorsal vein of clitoris ♀/penis ♂ (vena dorsalis profunda clitoridis ♀/penis ♂).
Drainage and communications: Dorsally, there are connections to the vesical and prostatic ♂ venous plexus, and caudally, with the internal pudendal vein.
The only eponym recommended for general use is that of the plexus pudendus – plexus of Santorini – see Table 2.
Eponyms recommended for general usage by IIC
TA, Terminologia Anatomica; IIC, International Interdisciplinary Committee
3Ce1 –
An unpaired vein, incorporated within the connective tissue sheath of the penis, just deep to the fascia of penis (fascia of Buck), receives blood from the glans penis and cavernous bodies, runs dorsally in the midline between the paired corresponding arteries (exceptional situation in the human body) and close to the suspensory ligament of penis (ligamentum suspensorium penis) it passes through a foramen between the inferior pubic ligament and anterior border of the perineal membrane (membrana perinei). There, it bifurcates into the right and left branch and empties into the pudendal plexus and/or into the internal pudendal vein. 6,19 There are no relevant and precise statistical data about the anatomical arrangement of this area.
3Ce2 –
This vein or these veins is/are unpaired and collect(s) the venous blood from the preputium and skin of the penis. They run dorsally in the subcutaneous tissue and divert either to the left or to the right to terminate into one of the external pudendal veins (usually the superficial one – vena pudenda externa superficialis) and via the great saphenous vein (vena saphena magna) they empty into the common femoral vein (vena femoralis communis). 20
3Cef –
This venous plexus is placed dorsally to the inferior pubic ligament (ligamentum pubicum inferius; obsoletely arcuate ligament) and lower part of the pubic symphysis, ventrally to the urinary bladder and prostate, within the lateral fascial sheath of the gland.
Its main tributary is the deep dorsal vein of the penis ♂ (vena dorsalis profunda penis ♂) and it receives other tributaries from the anterior part of the urinary bladder and prostate as well. Drainage: the plexus terminates into the vesical veins (venae vesicales) and internal iliac vein.
Communications: It anastomoses with the pudendal plexus vesical venous plexus (plexus venosus vesicalis) and internal pudendal vein.
For a detailled schema of visceral plexuses and their anastomoses (Figure 4).

Schema of the veins of pelvis, their draining directions and communications (anterior view). ci, canalis inguinalis; CMH, corona mortis Hesselbachi; cpa, canalis pudendalis Alcocki; ffsa, foramina sacralia anteriora; fim, foramen ischiadicum minus; fi, foramen infrapiriforme; fs, foramen suprapiriforme; PRE, plexus rectalis externus; PRI, plexus rectalis internus; PVVE, plexus venosus vertebralis externus; PVVI, plexus venosus vertebralis internus (anterior et posterior); VBV, vena bulbi vestibuli; VCAP1, vena comitans arteriae perforantis primae; VCFM, vena circumflexa femoris medialis; VCI, vena cava inferior; VCIP, vena circumflexa ilium profunda; VCIS, vena circumflexa ilium superficialis; VDPC, vena dorsalis profunda clitoridis; VEI, vena epigastrica inferior; VES, vena epigastrica superficialis; VF, vena femoralis; VFC, vena femoralis communis; VGI, vena glutea inferior; VGS, vena glutea superior; VI, vena iliolumbalis; VICdx, vena iliaca communis dextra; VICsin, vena iliaca communis; VIE, vena iliaca externa; VII, vena iliaca interna; VIs, vena ischiadica; VLA, venae labiales anteriores; VLAdx, vena lumbalis ascendens dextra; VLAsin, vena lumbalis ascendens sinistra; VLP, venae labiales posteriores; VvLTU, venae ligamenti teretis uteri; VMI, vena mesenterica inferior; VO, vena obturatoria; VOv, vena ovarica; VP, vena pubica; VvPC, venae profundae clitoridis; VPEP, vena pudenda externa profunda; VPES, vena pudenda externa superficialis; VPF, vena profunda femoris; VPI, vena pudenda interna; VPt, vena portae; VRI, vena rectalis inferior; VRM, vena rectalis media; VRS, vena rectalis superior; VSM, vena saphena magna; VScM, vena sacralis mediana; VU, vena uterina; VV- vena vesicalis; VV♀g, vena vaginalis; VvPP, venae perineales profundae; VvPS, venae perineales superficiales; VvS in FSA, venae spinales in foramina sacralia anteriora; VvSp, venae suprapubicae; VvSL, venae sacrales laterals; *, venae ligamenti lati uteri
Perineal veins (venae perineales)
They represent an individual group of the pelvic veins. This clinical term includes all veins of the perineum that can be classified as deep and superficial.
4A –
4B –
Gonadal veins drainage areas
These veins of the genital glands are evolutionary independent of the pelvic venous circulation. Nevertheless, they have close relations and communications with their venous network; finally, they terminate in the inferior vena cava at the level of the second lumbar vertebra, either directly or by means of the left renal vein.
1 –
They emerge from the posterior aspect of the testis, collecting blood from the epididymis, and fuse together to form the pampiniform plexus (plexus pampiniformis). This plexus twines the testicular artery, ascends along the anterior surface of the ductus deferens and is comprised within the spermatic cord. Distally to the superficial inguinal ring (anulus inguinalis superficialis), the plexus unites in 3–4 veins that pass through the inguinal canal (canalis inguinalis) and enter the abdominal cavity via the deep inguinal ring (anulus inguinalis profundus). There they again unite to form two veins ascending on both sides of the corresponding artery, dorsally to the peritoneum and ventrally to the ureter and psoas major muscle. The left-sided vein runs dorsally to the lower part of the descending colon and lower border of the pancreas and it is crossed ventrally with the left colic vessels (vasa colica sinistra). The right-sided one is located dorsally to the terminal ileum and lower part of the duodenum and it is crossed ventrally by the root of mesentery and ileocolic and right colic vessels (vasa ileocolica et colica dextra).
Gonadal veins contain valves in 62% of cases on the left side and in only 48% on the right. 21 The most frequently present one is situated at the termination of the vein (‘ostial valve; terminal valve’), representing 77% of the left-sided and 84% of the right-sided veins. 21
There is a significant difference in the anatomical arrangement of their terminations on the left and right side. In relation to the position of the vena cava inferior on the right side (a consequence of the development during which the inferior vena cava has arisen from different right-sided veins), the right-sided testicular vein terminates directly into the vena cava inferior unlike the left-sided one, which empties into the left renal vein (vena renalis sinistra), which has to traverse the abdominal aorta (aorta abdominalis) ventrally. The pathological result of this anatomical arrangement can be the presence of varicocoele on the left side in the majority of cases, probably due to the right-angle-junction of the left testicular and left renal vein. The termination of the gonadal veins has a classical textbook pattern in 79% of cases on the left and 78% on the right side. In the remaining 20% of cases there can be up to six different trunks, especially in the lower third. As the vein proceeds upwards, the confluence of veins reduces number of trunks, but even in the upper thirds a doubled or tripled trunk can be found in 19% and 1%, respectively. (For details, see reference 21.) The duplicated veins can often drain independently and do not unite into one trunk. Then, the first one follows the normal anatomical termination arrangement and the other usually enters the inferior vena cava distally to the level of the second lumbar vertebra. 13,20
2 –
Evolutionary they correspond to the male testicular veins. They commence in the plexus within the upper part of the broad ligament of the uterus (mesovarium, mesosalpinx), through which they communicate with the uterine venous plexus. They have the same arrangement, course in the abdominal cavity and termination sites as the testicular veins. Valves are present in the ovarian veins. They significantly dilate during pregnancy to accommodate the increased blood volume. Following childbirth, a period of venostasis occurs and the incompetence of those veins contributes to pelvic congestion syndrome. 13,20
The synonym ‘gonadal veins’ is appropriate only in general statements and ‘spermatic veins’ is considered obsolete.
LePage analysed the anatomical findings of the internal iliac venous system and stated that there were ‘anastomotic plexuses among the different visceral components of the pelvis and the relative scarcity of valves in the pelvic venous system, which have contributed to the understanding or the pathophysiology of reflux of the pelvic veins into the gluteal, vulvar, and lower extremity venous systems (pelvic dumping syndrome). However, it poses the following important question: if 90% of the individuals do not have valves in the internal iliac system, why do we not see more women with vulvar varices and symptoms of pelvic venous insufficiency? Twenty percent of pregnant women will develop varicose veins, but only one out of three will have vulvar varices’. 14 There are other factors resulting in the varicose veins development, such as genetic predisposition and disturbances in the collagen structure of the venous wall, May-Thurner's syndrome, direct compression of the inferior vena cava and pelvic veins by the pregnant uterus against the vertebral column, increase of the blood flow in the pelvic veins and femoral vein that can lead to the valvular incompetence, etc. The internal iliac vein and its complex system of the visceral and parietal tributaries serve as huge collateral in case of obstruction in the iliac and inferior vena cava system. 11
Both internal iliac veins communicate between each other by means of the various above-stated plexuses and form a unique, incontinent and constitutionally refluent system in the majority of cases, 22 but then the superficial veins of the pelvis (perineal veins, labial/scrotal veins), which possess valves, do not allow the reflux from the pelvis into the superficial venous system. But, especially in pregnancy, these valves get incompetent and serve as sources for varices in the vulva, perineum and lower extremities. Two main points of the ‘leakage’ have been described (‘P’ and ‘I’), followed with another two minor ones. 21
Pelvic leakage points (Figures 5 and 6):
Point ‘P’ – situated in the perineal membrane (membrana perinealis), which is traversed by the perineal veins, just after it receives the labial/scrotal tributaries. It connects the internal and external pudendal veins systems); Point ‘I’ – located at the superficial inguinal ring (anulus inguinalis superficialis), where the veins of the round ligament meet the superficial veins of the anterior abdominal wall and veins of the diverticulum of Nuck (a remnant of the embryonal vaginal process of peritoneum – processus vaginalis peritonei. It connects uterine and ovarian systems with those of external pudendal veins, superficial dorsal veins of clitoris/penis and anterior abdominal wall veins);
22
Point ‘O’ – found within the obturator canal (canalis obturatorius), connecting the deep veins of the proximal portion of the medial group of thigh muscles and the obturatory vein, emptying into the proximal segment of the internal iliac vein; Point ‘G’ – found in the gluteal region in which the variable sciatic vein (vena ischiadica), running on the posterior surface of the thigh from various level, joins the peripheral segment of the inferior gluteal vein (before the latter enters the infrapiriform foramen).
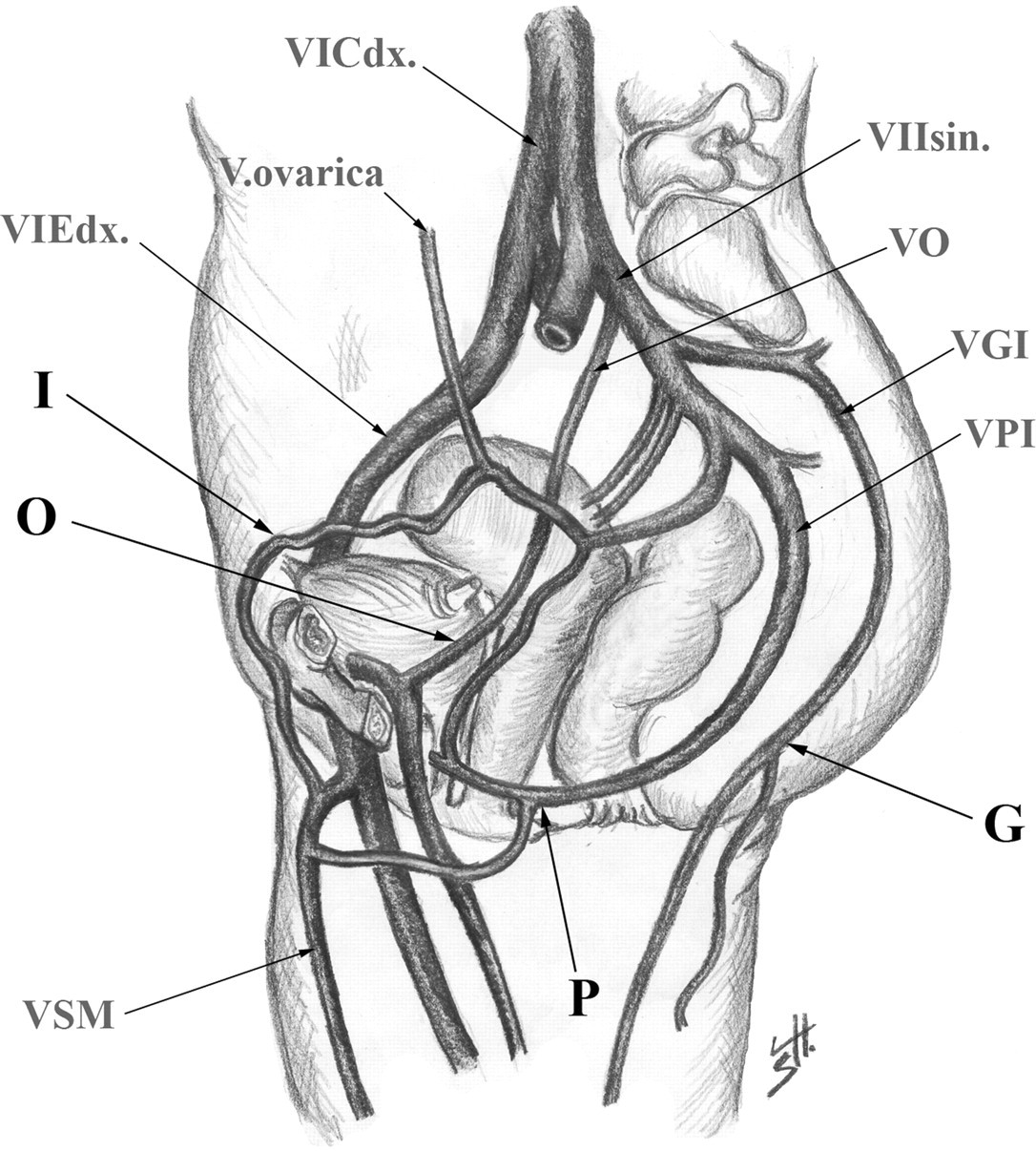
Scheme of pelvic leakage points, lateral view of pelvis section. G, ‘gluteal’ point; I, ‘inguinal’ point; O, ‘obturator’ point; P, ‘perineal’ point; VCI, vena cava inferior; VGI, vena glutea inferior; VIEdx., vena iliaca externa dextra; VIIsin., vena iliaca interna sinistra; VO, vena obturatioria; VPI, vena pudenda interna; VSM, vena saphena magna
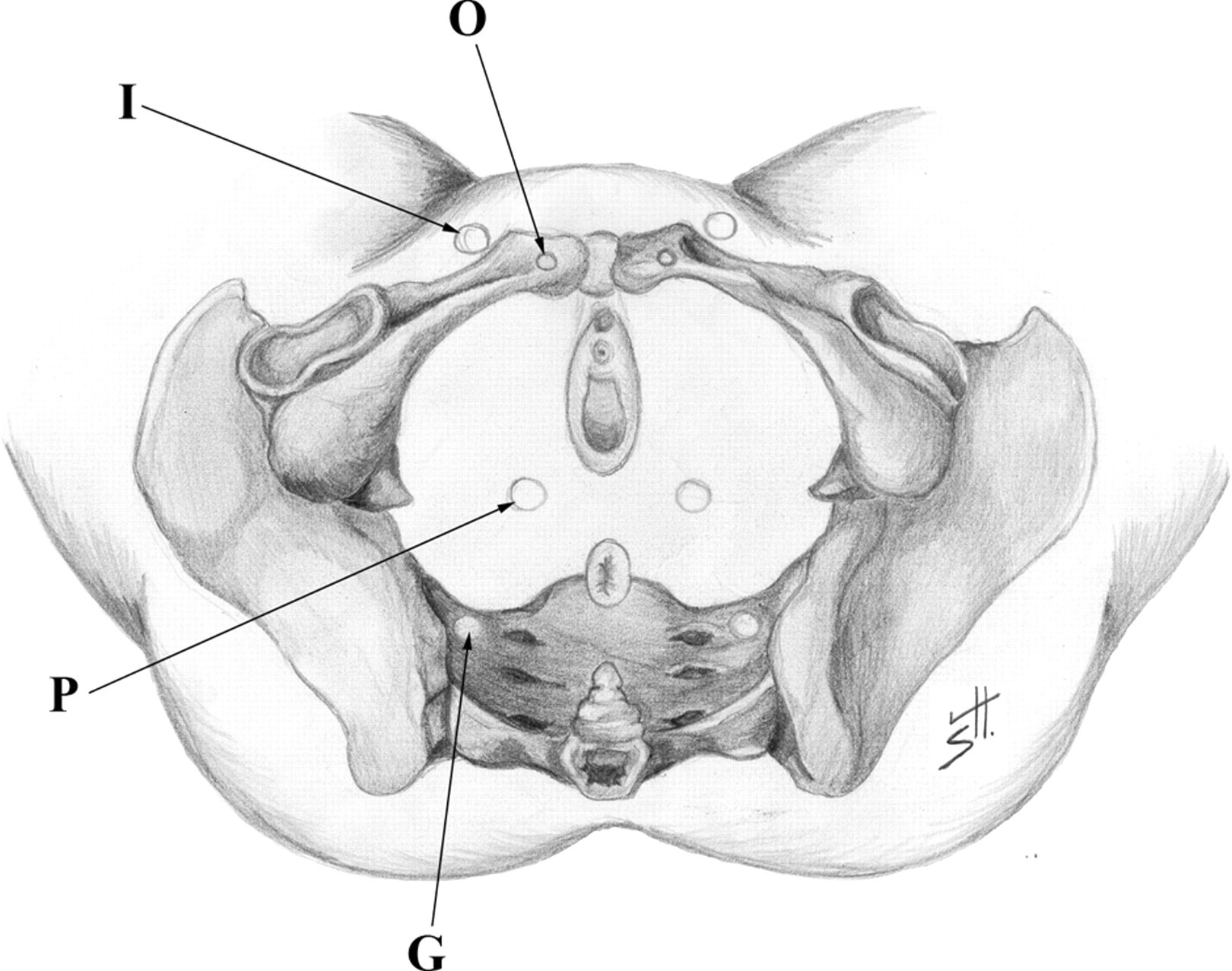
Scheme of pelvic leakage points, inferior view of the pelvis. G, ‘gluteal’ point; I, ‘inguinal’ point; O, ‘obturator’ point; P, ‘perineal’ point
These leakege points are the clinical anatomical structure, not having the corresponding terms within the anatomical terminology. Nevertheless, they are of a great importance for the evaluation of the reflux.
Eponyms
As a general rule, the use of eponyms is discouraged. Eponyms are not considered equal synonyms and the IFAA excluded them from the anatomical nomenclature as early as 1955 (Parisiensia Nomina Anatomica – PNA). 2,23 Unfortunately, this rule has only remained academic and the clinicians tend to use the eponymys for their shortness. A thorough survey of the recent literature demonstrated that some eponyms are correctly and frequently used in clinical journals with worldwide circulation – however, there is only one of them concerning the veins of pelvis – plexus of Santorini. 7 This article serves as a review and offers some other eponyms as well, for easy orientation of the clinicians (Table 2).
Conclusion
The consensus document added five new terms in both Latin and English languages in the chapter concerning the veins of the pelvis (indicated with the question-marks in the Table 1): pubic veins (venae pubicae), pudendal plexus (plexus pudendus), veins of broad ligament (venae ligamenti lati uteri), veins of round ligament of uterus (venae ligamenti teretis uteri), suprapubic veins (venae suprapubicae) and divided the term ‘rectal plexus’ into two terms: external rectal venous plexus (plexus venosus rectalis externus) and internal rectal venous plexus or haemorrhoidal plexus (plexus venosus rectalis internus; plexus haemorrhoidalis). Eponyms are not considered equal synonyms and the only eponym recommended for general use is that of the plexus pudendus – plexus of Santorini. The anatomical terminology is one of the basic communication tools and it is necessary to count with a clear and useful one. If such one exists and is extended, the overall and general usage is highly recommended to precede any misnomers and errors in future communication among specialists, scientists, teachers and students all over the world.
Footnotes
Acknowledgment
The authors thank Štěpán Hájek for the graphic part of the article and to Miroslava Plecitá for the librarian services.