
Abstract
Background
Compression stockings are the cornerstone of the treatment of chronic venous disorders, but practical acceptability is an important limitation in the elderly.
Objective
To evaluate the practicability of compression stockings in elderly patients.
Methods
Twenty women aged 68–85 years without major disability were asked to put on, wear for three hours and take off Solegg® and Solegg® Fine compressive stockings (15–20 mmHg) in random order on different days, and to rate through questionnaires the difficulties and discomfort they experienced in comparison with their usual non-compressive stockings (controls).
Results
Foot and heel insertions of the compression stockings, as well as their removal, were found significantly more difficult, whereas comfort when they were on was higher. In the whole, the compression stockings were found to be more agreeable than the controls.
Conclusion
Difficulties regarding putting on and removal of the compression stockings remain significant but are counterbalanced by a better comfort when they are on.
Keywords
Introduction
As stated by most guidelines regarding venous disorders, 1,2 elastic compression stockings are the cornerstone of the treatment of chronic venous disorders. However, it is often difficult for the patient to deal with the practical aspects of this kind of treatment, and these difficulties lead to a poor compliance, which, indeed, is its most important limitation, since less than one out of three patients with chronic venous disorders regularly wears compression stockings. 3
As the disease is more prevalent in the elderly, when orthopaedic disorders of the spine and joints of the lower limbs result in additional limitations, the practical problems of putting on and taking off of stockings become even more important. The aim of the study was to evaluate the acceptability and practicability of putting on and taking off two kinds of elastic compression stockings: Solegg® 2 and Solegg® Fine 2, as well as the level of comfort or discomfort felt by elderly subjects when wearing them.
Methods
Subjects were 20 elderly women, mean age 75.0 ± 5.2 years, on spa treatment for venous (15) or rheumatological (18) disorders in the resort of La Léchère (Savoie, France) in September/October 2007 and complaining of venous symptoms (14 of the subjects attended both venous and rheumatological treatments). The clinical, aetiological, anatomical and pathological elements (CEAP) ‘C’ classes of the subjects were as follows: C1 = 2, C2 = 8, C3 = 4, C4 = 5 and C5 = 1. Most subjects presented several symptoms corresponding to different CEAP scores, e.g. varicose veins over 3 mm (C2) and ankle oedema (C3), but only the highest CEAP score was kept for each patient. The demographical and anatomical data are summarized in Table 1.
Mean, minimum and maximum values of age, height, weight, BMI, heart rate and leg measurements with corresponding standard deviations

To be included, the subjects had to usually wear city socks or stockings but not elastic compression stockings on a daily basis. Other non-inclusion criteria included being engaged in another biomedical study at the time, ankle or calf circumferences outside of the Solegg size chart, open ulcer, acute dermatitis, any skin ulceration or eczema. Subjects unable to put on their usual (non-compressive) stockings by themselves whatever the reason or unable to understand or answer an auto-questionnaire were not included either. All subjects had to give written, informed consent and the study protocol conformed to the ethical guidelines of the current revision of the 1975 declaration of Helsinki. The study protocol was approved by the institutional review board Comité de Protection des Personnes (CPP) of Grenoble (France) on 1 August 2007, as well as by the AFSSAPS (Agence Française de Sécurité Sanitaire des Produits de Santé).
Each subject had to put on, wear for three hours and remove two investigated stockings and their own usual non-compressive stockings. The tests were performed at about the same time for the three days of the test (mean observed difference between the three sessions 3.75 minutes, maximum 10 minutes). The subjects were asked to keep their activities during the three hours as comparable as possible for the three days of the test. This activity usually consisted in a three-hour walk, as prescribed by their appointed physician during the spa treatment. The two investigated stockings were Solegg 2 and Solegg Fine 2, two elastic compression orthesis, French compression class II (15–20 mmHg at ankle level) manufactured by the Laboratoires Innothera, Arcueil (France), made of cotton, polyamides and elasthanne-lycra® at different ratios with double-covered yarns, as dictated by the French technical system of reference (Asqual 4 ). These stockings are closed-toes, knee high, with a pressure level of 15–20 mmHg at ankle level which is the norm in France for Class II elastic compression products and usually prescribed for venous symptoms. They are specifically targeted at women and the size chart is fitted to women measurements. The stockings were provided for each subject according to personal sizing (ankle and calf circumferences, knee height). These measurements are summarized in Table 1.
The control stockings were always worn on the second day and the two compression stockings were tested on the first and the third days, the allocation order being randomized using a balanced complete block of four treatments. The subjects were kept blind about the kinds of stockings they wore on days 1 and 3, although they were able to recognize the control stocking since it was their own. The subjects put on their stockings – compressive or not – following the same step-by-step method, which was explained to them and was visible on a poster throughout the putting on phase. This was done to avoid the discrepancies that would have occurred if each subject had chosen by herself how to put on her stockings. Difficulties and discomfort when putting on, wearing and removing the stockings were rated by the subjects through auto-questionnaires after each test, using ordinal three or four categories scales as well as 10 cm visual analogue scale (VAS). The questions were as follows:
Q1: Do you think that, as a whole, these stockings are easy or difficult to put on? (VAS range: impossible–no difficulty); Q2: During the putting on, do you think passing the foot into the stocking was easy or difficult? (VAS range: impossible–no difficulty); Q3: During the putting on, do you think passing the heel into the stocking was easy or difficult? (VAS range: impossible–no difficulty); Q4: If a difficulty arose while putting on the stockings, please explain where it came from (Difficulty to seize the stocking with your hands/Difficulty to bend to put on the stocking/Difficulty at knee or ankle level/Other reason: explain; Q5: A few minutes after putting on the stockings, which impression do they give you as a whole? (VAS range: very agreeable–very disagreeable); Q6: A few minutes after putting on the stockings, which impression on the skin do they give you? (VAS range: very agreeable–very disagreeable); Q7: A few minutes after putting on the stockings, which impression on the leg do they give you? (VAS range: very agreeable–very disagreeable); Q8: Would you say that these stockings were comfortable to wear for three hours on the whole? (VAS range: perfectly comfortable–unbearable); Q9: At the end of the three hours, what did you feel at skin level? (VAS range: very agreeable–very disagreeable); Q10: At the end of the three hours, what did you feel at leg level? (VAS range: very agreeable–very disagreeable); Q11: After three hours, would you say that these stockings were easy or difficult to remove? (VAS range: impossible–no difficulty); Q12: If a difficulty arose while removing the stockings, please explain where it came from (Difficulty to seize the stocking with your hands/Difficulty to pass the heel out of the stocking/Difficulty to put the foot out of the stocking/Other reason: explain); Q13: What is your global feeling about the use of these stockings for three hours (including putting on and removal)? (VAS range: very positive–very negative).
The subjects were asked to answer the questionnaire independently for the left and right leg. Statistical analyses were performed with SPSS software (version 14.0 for Windows), using Wilcoxon paired tests with a 0.05 P value as the significance threshold, with the exceptions of questions Q4 and Q12 which were not statistically analysed. Comparisons addressed the difference between each elastic stocking and the ordinary, non-elastic stocking usually worn by the subject. Variables are described as median and interquartile ranges.
Results
A preliminary statistical analysis comparing the results of each question between the right and left leg returned no significant difference between the two legs. In the following part, the authors chose to present the results for the right leg of the subjects only, except when noted otherwise. Thus, the statistical analyses were performed on 20 right legs and not on all 40 legs, which would have led to an artificial underestimation of the calculated P values.
As a whole (Q1), putting on the stockings was not considered significantly more difficult by the subjects for either elastic compression stocking, compared with the controls (Figure 1). However, in the detailed analysis of the different steps when putting on (Q2, Q3), a significant difference was found for the insertion of the foot (P = 0.0050 for both stockings) and of the heel (P = 0.0029 for Solegg Fine 2, and P = 0.0065 for Solegg 2, respectively) (Figure 1). The two main explanations given by the subjects for their difficulties at this stage (Q4) were joint problems for bending the back, hip, knees or heels (Figure 2).

Median scores for the putting on difficulty, with interquartile range. Stars mark statistically significant differences between Solegg Fine and Control (black) or between Solegg and Control (grey) at risk 0.05 (*) or 0.01 (**). VAS, visual analogue scale
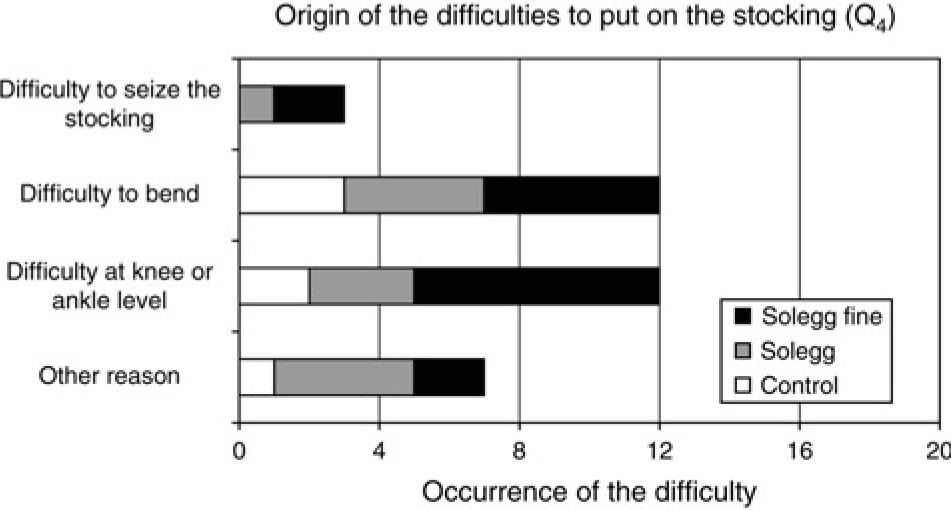
Occurrences of the reasons invoked in case of difficulty to put on the stockings (both legs are accounted for)
During the time they wore the stockings, comfort was found significantly better with both elastic compression stockings than with the controls, when asking the question after a few minutes (P = 0.0011 for Solegg Fine 2, and P = 0.0057 for Solegg 2, respectively) as well as at the end of the three hours (P = 0.0032 for Solegg Fine 2 and P = 0.0006 for Solegg 2, respectively). This was true for the global comfort (Q5, Q8), as well as for the feeling at the skin level, and for the whole leg (Q6, Q7, Q9 and Q10) (Figures 3 and 4).

Median scores for immediate comfort, with interquartile range. Stars mark statistically significant differences between Solegg Fine and Control (black) or between Solegg and Control (grey) at risk 0.05 (*) or 0.01 (**). VAS, visual analogue scale
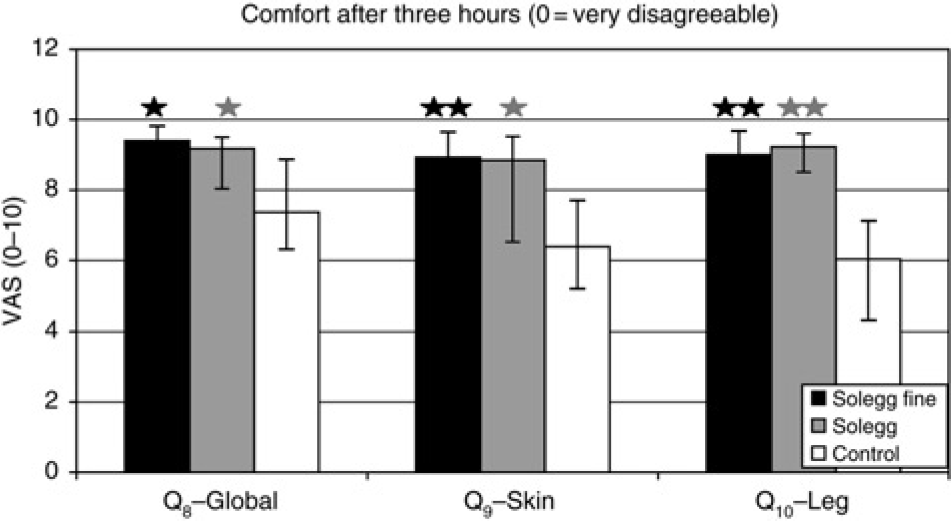
Median scores for comfort after three hours, with interquartile range. Stars mark statistically significant differences between Solegg Fine and Control (black) or between Solegg and Control (grey) at risk 0.05 (*) or 0.01 (**). VAS, visual analogue scale
Removing the stockings (Q11) was considered significantly more difficult with the elastic compression stockings (P = 0.0486 for Solegg Fine 2, and 0.0111 for Solegg 2, respectively) (Figure 5). On the whole (Q13), even when including the putting on and removal steps, the subjects found the use of the stockings more agreeable with the stockings than with the control (P = 0.0139 for Solegg 2 and close to the significance threshold level at P = 0.0526 for Solegg Fine 2) (Figure 6). The reasons invoked in case of difficulties (Q12) were mostly explained by a difficulty to pass the heel (Figure 7). No significant difference was found between the two compressive stockings (P > 0.05 for every item). Results are summarized in Table 2 and calculated P values are given in Table 3.
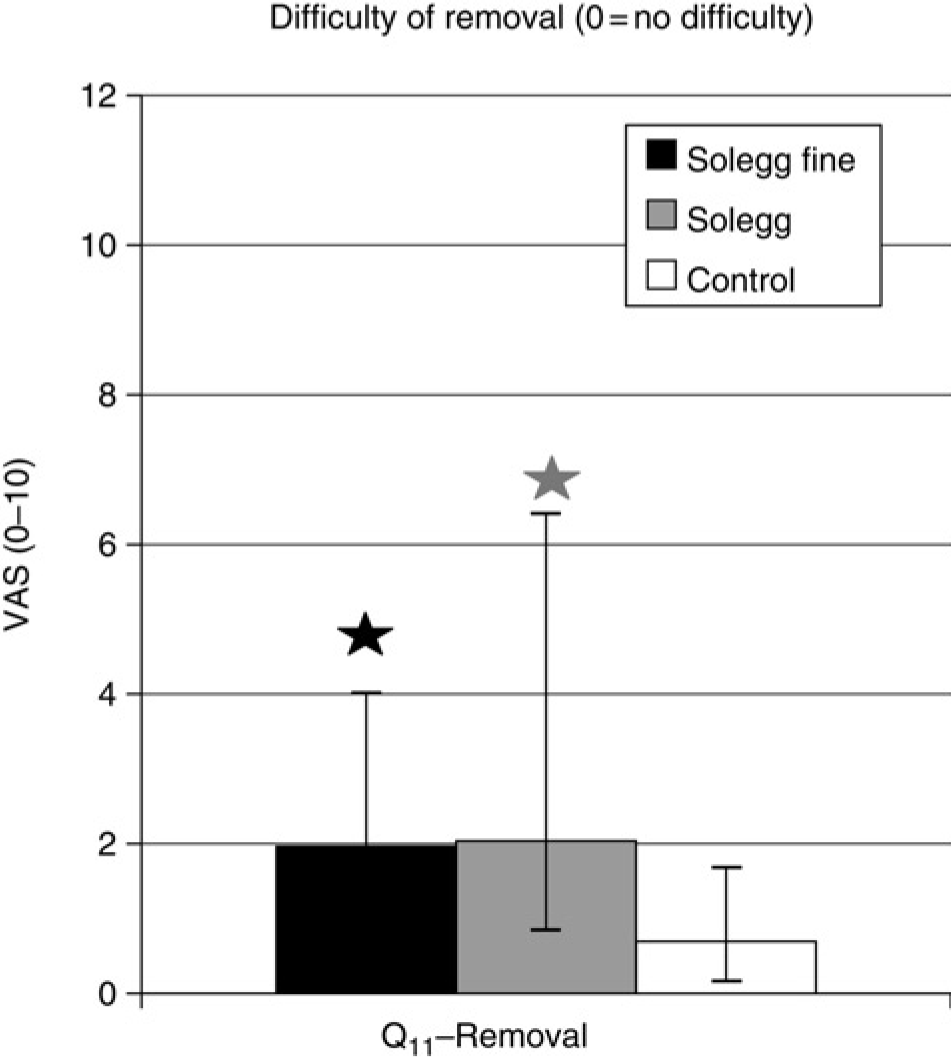
Median scores for difficulty of removal, with interquartile range. Stars mark statistically significant differences between Solegg Fine and Control (black) or between Solegg and Control (grey) at risk 0.05 (*) or 0.01 (**). VAS, visual analogue scale
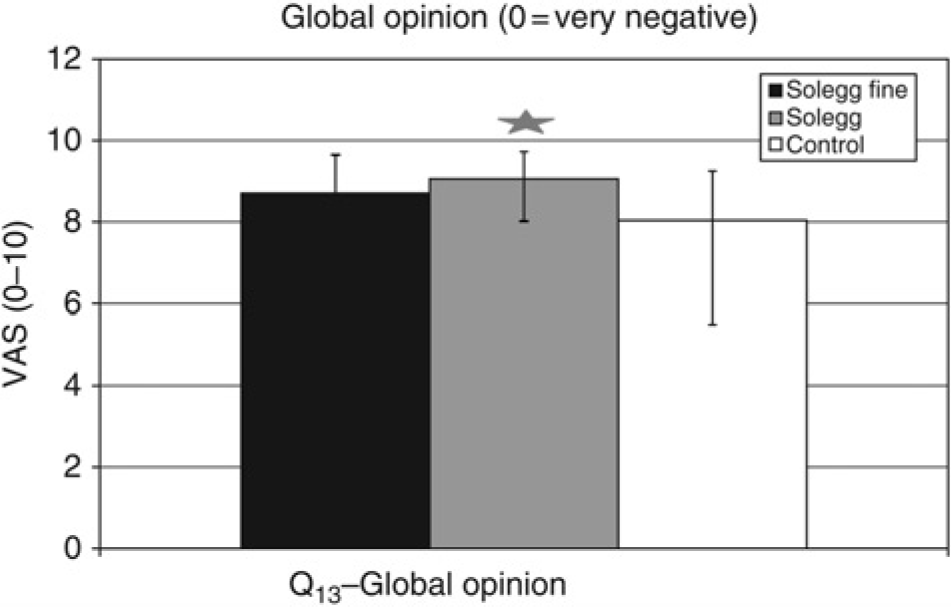
Median scores for global opinion, with interquartile range. Stars mark statistically significant differences between Solegg Fine and Control (black) or between Solegg and Control (grey) at risk 0.05 (*) or 0.01 (**). VAS, visual analogue scale
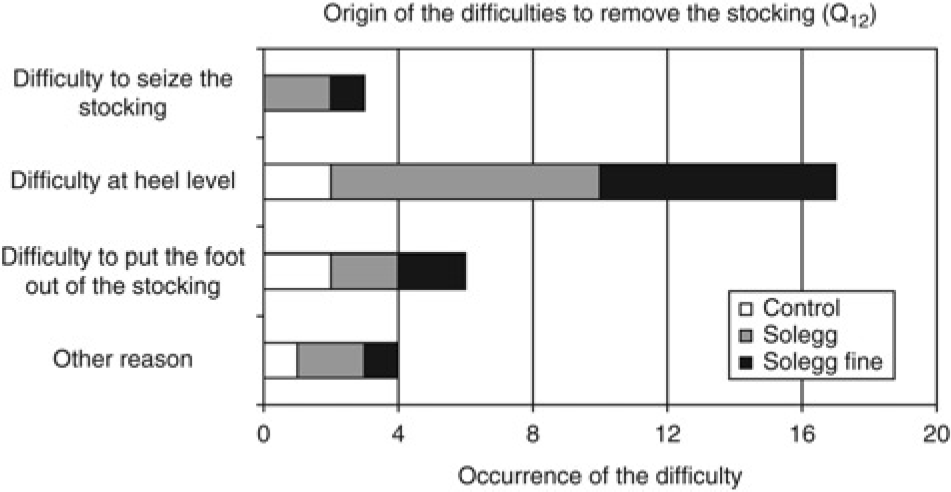
Occurrences of the reasons given in case of difficulty of removing the stockings (both legs are accounted for)
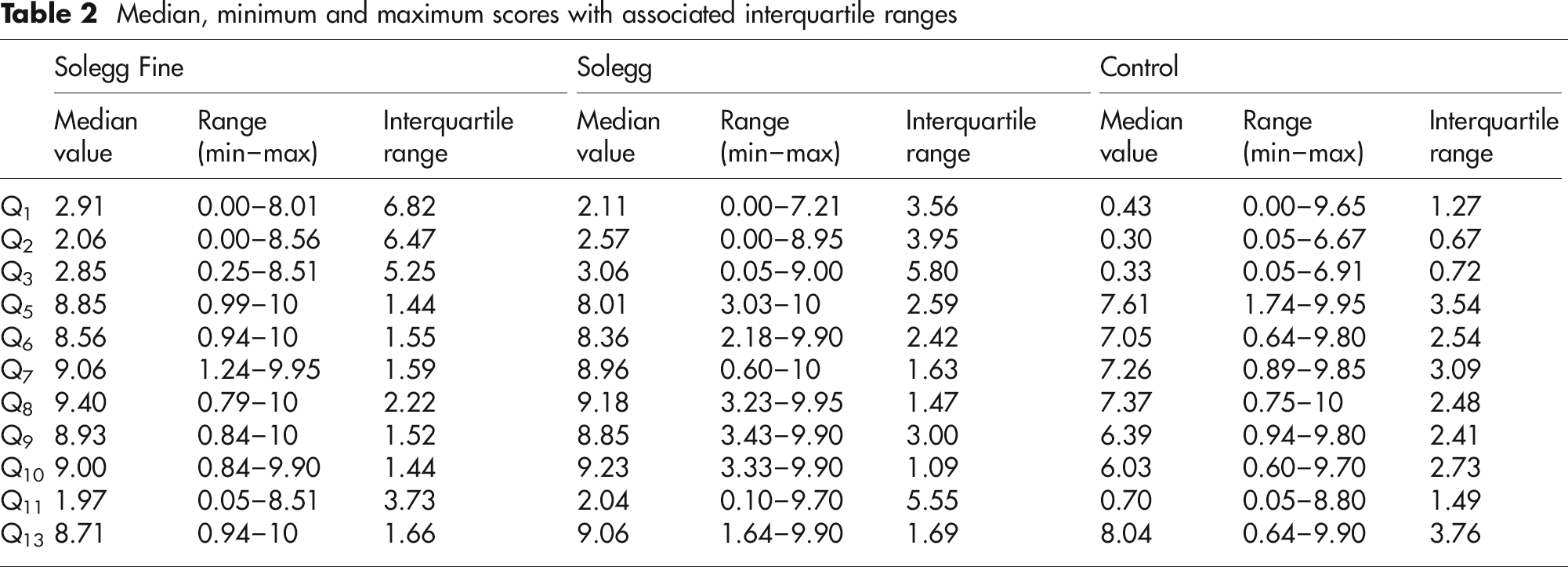
Median, minimum and maximum scores with associated interquartile ranges
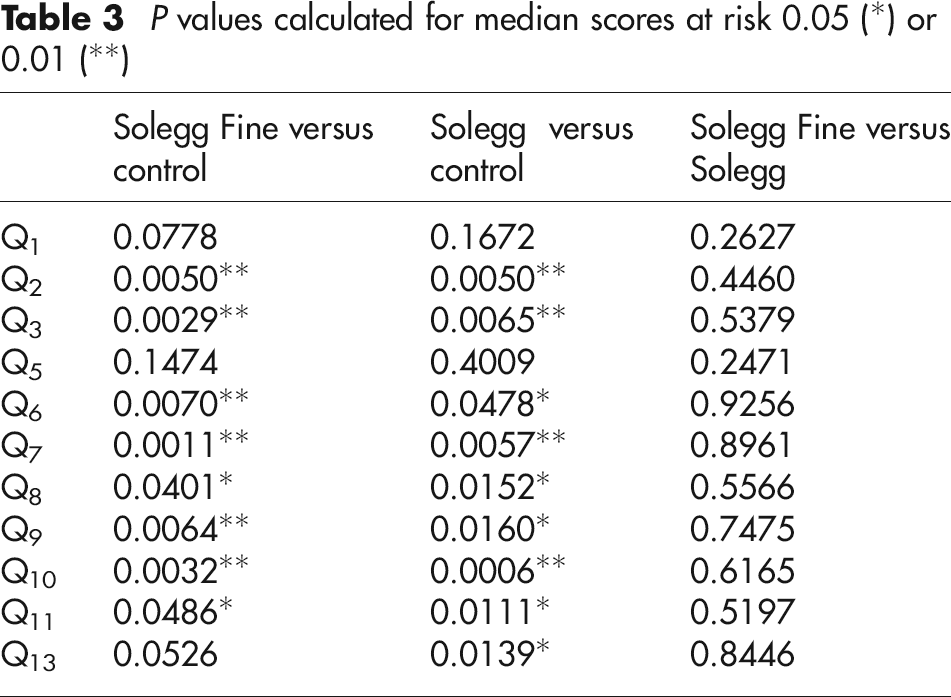
P values calculated for median scores at risk 0.05 (*) or 0.01 (**)
Discussion
In this study testing two kinds of French class II (15–20 mmHg at ankle level) elastic compression stockings, most difficulties met by the patient were linked to orthopaedic problems mainly impeding the putting on. Although of relatively low magnitude, these difficulties are significantly more important with the elastic compression stockings than with the usual non-compressive ones. A more detailed analysis showed that these difficulties were comparable for both legs when putting on the stockings (16 on the right versus 18 on the left), but were more pronounced for the right leg (28 on the right versus 2 on the left) when removing them. This can probably be explained by the fact that the subjects used both hands to put on the stockings (hence the symmetry), but removed the stocking on one leg with the opposite hand. Since significantly more subjects were right handed, more difficulties logically appeared when using the left hand, i.e. on the right leg.
Twelve out of the 20 recruited subjects were moderately suffering from upper limb osteoarthritis (5 at the shoulder level and 7 at the hand). Nine out of the 20 recruited subjects were moderately suffering from lower limb osteoarthritis (6 at the knee level and 3 at the hip). This may account for some of the difficulties felt by the subjects when putting on or removing their stockings. In any case, the presence of osteoarthritis was not severe enough to prevent the subjects from putting on or removing even the compressive stockings, which would have been a non-inclusion criterion.
One should note that four out of the 20 subjects experienced significant difficulty in putting on even their usual non-compressive stockings (answers to Q1 ≥ 5). These subjects were included in the main analysis, but we thought it interesting to also look at their specific results independently. Due to their small number, no specific statistical analysis was performed for these four subjects, but they found both compressive stockings globally easier to put on than their control stockings (median scores for Q1 was 6.52 for the control versus 2.84 and 4.83 for Solegg 2 and Solegg Fine 2, respectively). Their global opinion (Q13) was also in favour of the compressive stockings (median scores for Q13 was 7.78 for the control versus 9.08 and 8.76 for Solegg 2 and Solegg Fine 2, respectively). No correlation was found with the presence or absence of recorded arthropathy since two of these four subjects did not have arthropathy of either upper or lower limb, and one had arthropathy on both hand and hip. It is then doubtful that arthropathy would be the main source of difficulty even for these four specific subjects.
It should be noted that none of the 20 subjects was unable to either put on or remove the stockings, and the global judgement of the subjects was positive, with a better comfort when wearing the compressive stockings overbalancing the difficulties. In any case, if possible, any improvement in the field of practicability of the use of elastic compression stockings is worth implementing because once the putting on phase is passed, the subjects' judgement on the comfort of the stockings is positive.
Conclusion
This study shows that it is possible to test the acceptability and practicability of elastic compression stockings in the elderly, and we think that this approach is important for the compliance and therefore the efficiency of compression therapy in real life.
Footnotes
Acknowledgements
The authors express their deep appreciation to Corine Trolliet for the excellent practical organization of the trial, as well as to the patients who kindly agreed to take part in this study. The Laboratoires Innothera provided the stockings for each subject. The work load for this study was compensated by funding from our research centre that allowed for the corresponding salary of the investigators. Patrick Carpentier received an honorarium for the methodology and data analysis, and for the presentation of the study at a national congress. François Becker received fees as Medical Scientific Consultant at the Biophysics Department of the Laboratoires Innothera. Grégory Thiney is employed full time by the Laboratoires Innothera as Project Leader and participated in the design of the protocol and Case Report Form, as well as in providing the tested stockings in accordance with each subject's measurements.
Method for putting on the stockings