
Abstract
A 31 year-old female patient, an opera singer, came for a consultation, mainly for aesthetic problems of the lower limbs. An asymptomatic bilateral P-point pelvic shunt was demonstrated by the EchoDoppler, while no nutcracker syndrome was detected. The examination demonstrated a medial circumflex femoral vein (MCFV), going into the common femoral vein and then into the great saphenous vein (GSV). The Valsalva manoeuvre showed the GSV terminal valve incompetence. A dilated MCFV vein at the level of the saphenofemoral junction was the source of the reflux through the GSV, while the external iliac vein was competent. GSV reflux with Valsalva was present only in the lying position. Flow in the MCFV was directed toward the CFV during and after the Valsalva. The examination shows clearly that a GSV reflux can sometimes occur in absence of iliac reflux. Circumflex femoral veins (medial and lateral) are anatomical variations, but common findings during ordinary EchoColourDoppler investigations of the venous system of the lower limbs.
Introduction
It is a common belief that an escape point from the saphenofemoral junction (SFJ) must always be fed by the external iliac vein (EIV), through an incompetent or absent ilio-femoral valve (IFV) 1 (Figure 1).
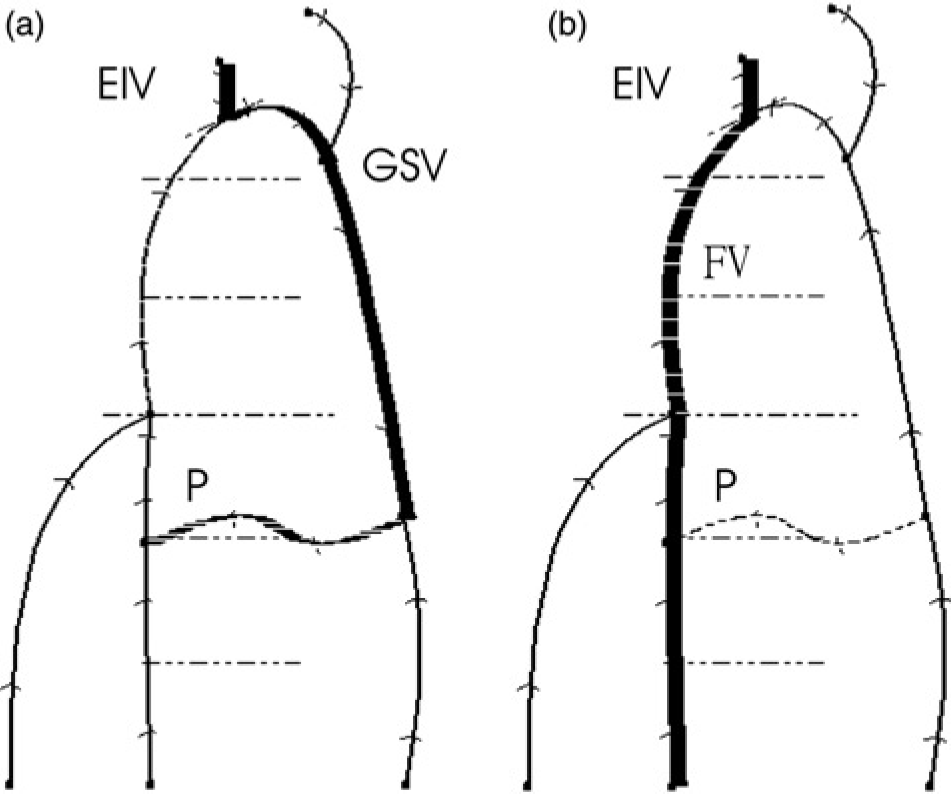
EIV feeding of SFJ. SFJ incompetence fed by a refluxing EIV: (a) during the Valsalva; and (b) after the Valsalva. Arrows indicate the versus of flow. EIV, external iliac vein; FV, femoral vein; GSV, great saphenous vein, P, perforator
This point of view systematically underestimates the physiopathological meaning of the confluence of other vessels into the common femoral vein (CFV), so that the ultrasound examination generally omits their observation, unless they have an evident compensating role in an ilio-femoral thrombosis.
Their thorough examination instead allows the evaluation of cases of incompetence at their very onset, so giving the opportunity to observe the sequence of the physiopathological phenomena of varicogenesis.
Circumflex femoral veins (CXFVs) are generally not routinely studied and even the recent changes in the anatomical nomenclature 2 confirmed only the pre-existing data and names.
The reported clinical case gives hints for going deeply into these topics.
Case report
A 31 year-old young female patient, an opera singer, came for a consultation, mainly for aesthetic problems of the lower limbs. She was not pregnant, nor had other comorbidities, and her family history was negative for venous and vascular diseases. Clinical, aetiological, anatomical and pathophysiological elements (CEAP) score was C1,SEp AS1,2,5,D10,P18 Pr. and only teleangectasiae were clinically evident.
An asymptomatic bilateral P-point pelvic shunt 3 was demonstrated by the EchoColourDoppler (ECD), while no nutcracker syndrome was detected.
A haemodynamic venous map of the left lower limb was performed to detail the features of the venous network 4 (Figure 2).
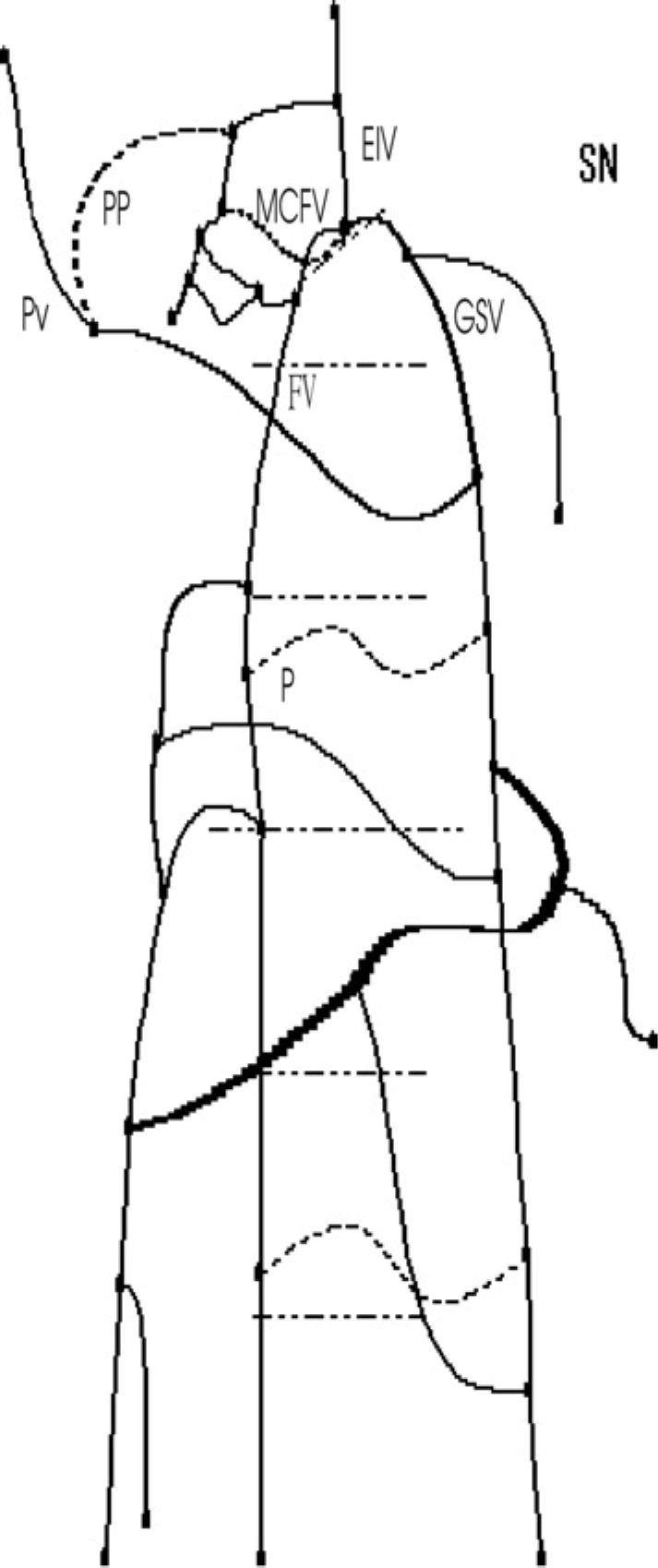
The haemodynamic venous map of the patient. EIV, external iliac vein; FV, femoral vein; GSV, great saphenous vein, P, perforator; PP, the P pelvic escape point; Pv, perineal vein; MCFV, medial circumflex femoral vein
The examination demonstrated a medial circumflex femoral vein (MCFV), going into the CFV and then into the great saphenous vein (GSV) (Figure 3a).
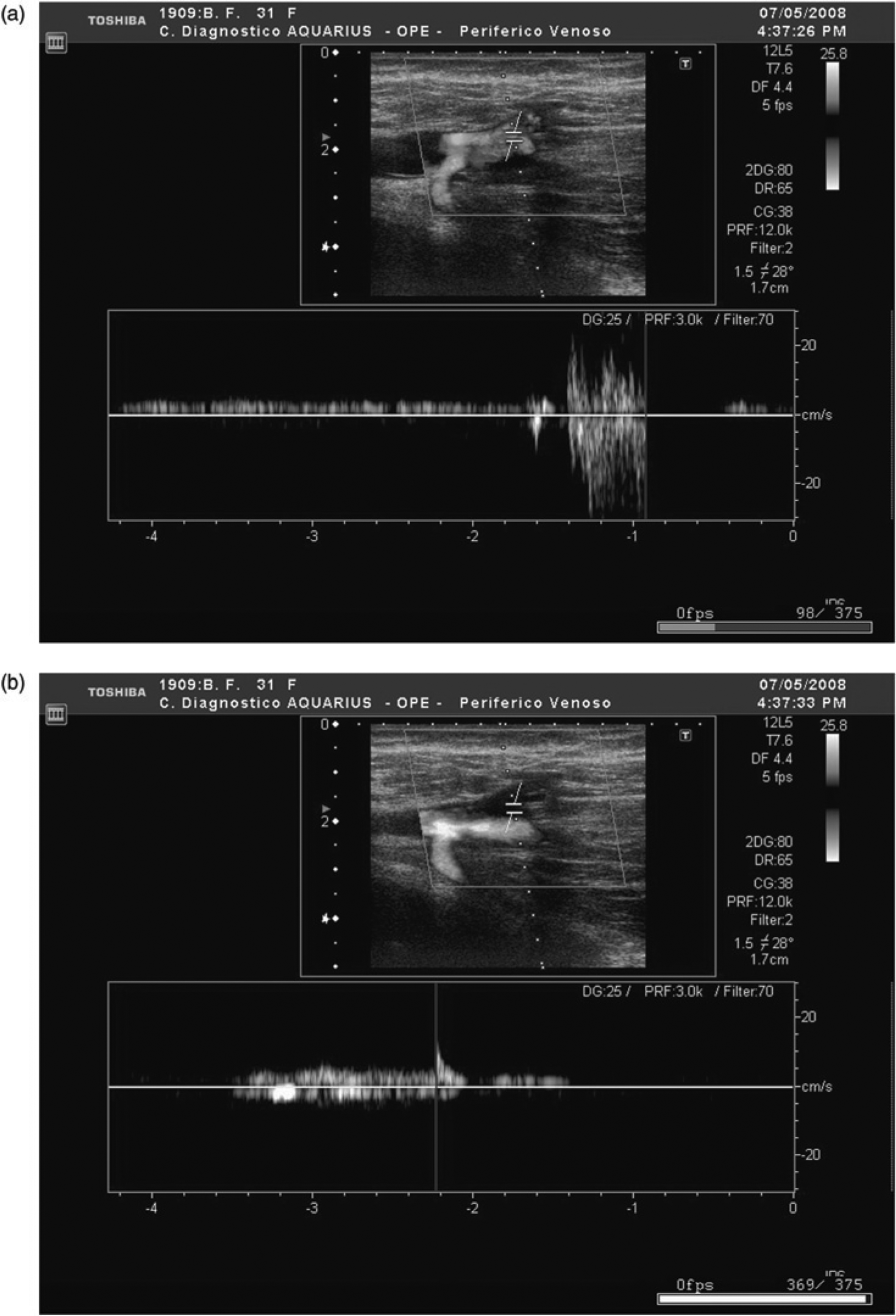
ECD of the SFJ. The sample volume is set in the CFV at the SFJ, with an angle correction normal to the TV plane, to detect the GSV TV incompetence. Images are taken in two consecutive phases of a Valsalva manoeuvre. In both phases the MCFV is anterograde. (a) During the Valsalva (time 0 s): a blood jet traverses the CFV. The jet enters an incompetent SFJ, eccentrically and cranial to the position of the sample volume, where instead turbulence is present causing an unreliable Doppler signal; (b) After the Valsalva (time 7 s): the GSV reflux stops (0 flow) and the CFV flow becomes again anterograde, far from the place where the sample volume is positioned
A longitudinal section of the SFJ showed the following valves: ilio-femoral, epigastric, SFJ terminal and pre-terminal ones. The Valsalva manoeuvre caused the GSV terminal valve (TV) incompetence. A dilated MCFV at the level of the SFJ was the source of the reflux (longer than 1 second) through the GSV, while the EIV and the IFV were competent (Figure 3a). GSV reflux during Valsalva was present only in the laying position, while it disappeared in the standing position. Two external pudendal veins directly joining the CFV had no participation in the mechanism of the SFJ incompetence.
No surgical indication was set, so that the patient underwent only an aesthetic sclerotherapy, not involving the GSV trunk. The patient was actually lost at follow-up.
Discussion
Flow in the MCFV was directed towards the CFV during and after the Valsalva. In the first phase, flow deviated from the anterograde direction into the iliac vein (Figure 3b) towards a retrograde flow (reflux) into the GSV (Figure 3a).
A detailed but schematic representation of the dynamics of flow in the involved veins is given as a sequence of static images 5 (Figure 4 and Table 1).
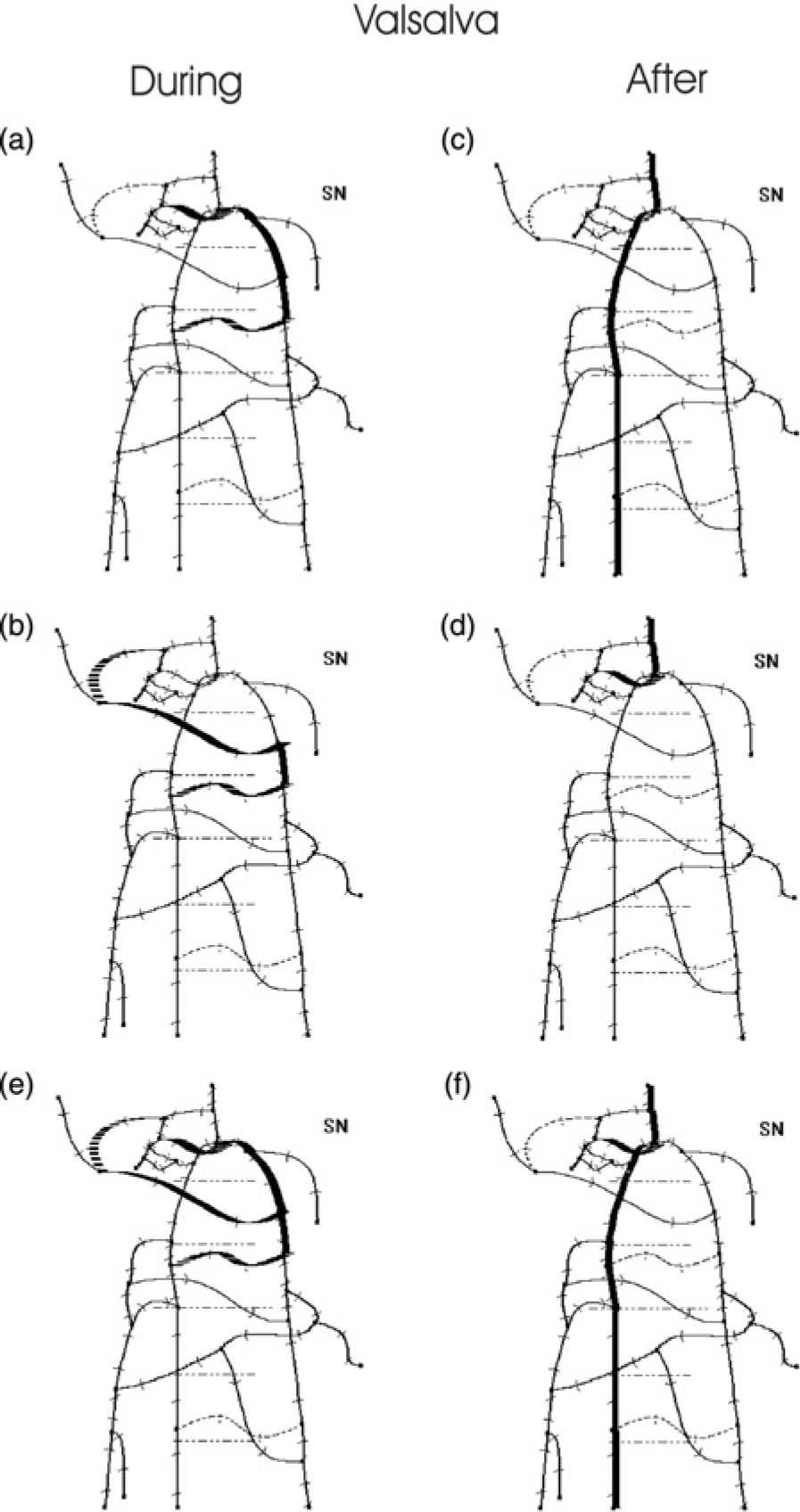
MCFV feeding of SFJ. When a Valsalva is performed, several paths (a, b, c and d) become active, depending on the phase of the manoeuvre and on the body position, giving an overall flow pattern representation (e, f), according to the synthetic scheme in Table 1; (a, b and e) Retrograde flow during Valsalva; (c, d, f) anterograde flow after Valsalva
Body position and overall flow patterns
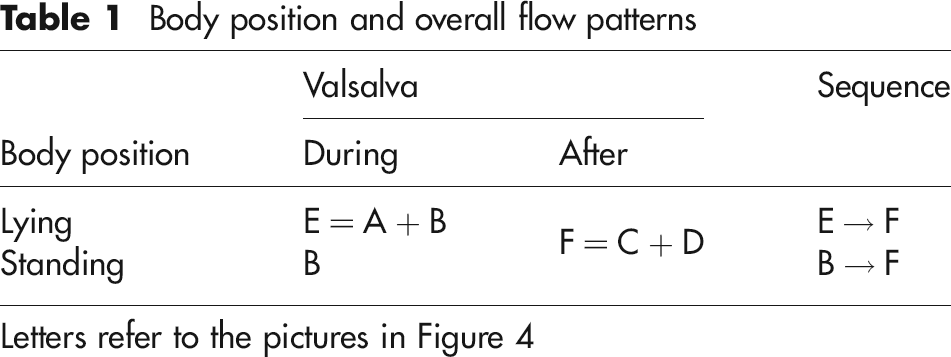
Letters refer to the pictures in Figure 4
During the Valsalva the SFJ reflux disappears in the standing position. This observation shows the need for additional studies to get a better comprehension of the physiopathology of the SFJ incompetence.
The examination shows clearly that a GSV reflux can sometimes occur in absence of an iliac reflux.
The CXFVs (medial and lateral) are tributaries of the deep femoral vein. When they join the CFV, they are anatomical variations, but also common findings during ordinary ECD investigations of the venous system of the lower limbs.
Conclusions
The CXFVs are factors of a different physiopathology of the SFJ incompetence, which can be detected instrumentally even if the IFV is competent.
In addition, in this clinical case the SFJ incompetence is at its very onset, present only in the lying position and in absence of GSV dilation (incompetent GSV TV and normal trunk). The current case report is:
In line with recently reported data on the order of appearance of the reflux in the saphenous trunks, which support a descending varicogenesis (the reflux first, the dilation secondarily);
6
Not in line with some evidences available in literature, which support an ascending varicogenesis, starting from the tributary veins towards the saphenous trunks.
7