
Abstract
A clinical model to examine the hypothesis that venous hypertension of the lower leg per se can cause lower leg stasis dermatitis is described. To prove this concept, we retrospectively studied a consecutive series of 38 patients with lower leg dermatitis who underwent phlebological examination at our consultation over a period of four years. Among those patients who had an insufficiency of the superficial veins only, without insufficiency of the deep veins, 22 had undergone patch testing to common allergens in phlebology. We found 10 patients with a stasis dermatitis of the lower leg and an incompetent great saphenous vein, six of whom had no detectable contact sensitization at all and another four exclusively to phlebologically irrelevant substances, e.g. nickel, cobalt, chromate or epoxid resin. All these 10 patients showed long saphenous vein incompetence from the groin to the medial aspect of the leg. All were operated by classical flush ligation and saphenectomy. Lower leg dermatitis healed in all 10 patients within 8–12 weeks and no recurrence was observed (1 year follow-up). These results support clinical experience that venous hypertension alone indeed can cause lower leg dermatitis.
Keywords
Introduction
Most phlebologists would agree that lower leg dermatitis is a common condition among patients with chronic venous insufficiency (CVI). In the population-based cross-sectional Bonn Study, 3.7% of participating persons complained of eczema of the lower leg and 2.9% of examined persons showed lower leg skin changes in the context of CVI (stage C4, clinical, aetiological, anatomical and pathophysiological elements [CEAP] classification 1 ) including lower leg dermatitis. 2
However, the existence of a pure form of stasis dermatitis with venous stasis as the exclusive cause of lower leg dermatitis might be challenged. Lower leg dermatitis can be caused by several factors, such as CVI (‘stasis dermatitis’, corresponding to CEAP classification stage C4a), 1 but also by contact sensitizations (‘allergic contact dermatitis’), ‘xerosis cutis’ (dry skin) corresponding to cumulative-toxic contact dermatitis in sebostatic skin, ‘atopic dermatitis’ and in many cases by combinations of several factors.
Patients with clinical stage C4–C6 (CEAP classification) 1 of CVI seem to carry a higher risk of contact sensitization, ranging from 37% to 85%. 3 Three pathophysiological factors are likely to enhance sensitization rates in CVI patients: high penetration of allergens through the deteriorated epidermal barrier, particularly long and repetitive contact of potential allergens with the skin and application of particularly potent allergens in local therapy of dermatitis and chronic wounds. 3 Venous ulcer patients (C5, C6) tend to have even higher sensitization rates, around 66%, a prevalence that remained unchanged over the last decades. 4,5 The following four groups of allergens – identified by using standardized patch tests – are believed to be particularly typical for CVI patients: (1) lanolins and derivatives; (2) Peru balsam-colophony-fragrances; (3) neomycin and related antibiotics; and (4) preservatives. 4 In using a patch test series based on the European standard series, antimicrobial and medicament series and a variety of commonly used topical leg ulcer treatments as well as any additional topical treatments the examined (ulcer) patient was using, similar results were shown, but additionally rubber and topical corticosteroids, as well as some wound dressing components were detected as common contact allergens. 5
Stasis dermatitis can also be found outside of the classical location on the lower leg, for example: distally to arterio-venous fistulas in haemodialysis patients, all trophical skin changes attributed to CVI, including stasis dermatitis, can occur. 6
Patients and methods
We suggest three criteria to be fulfilled in order to support the existence of stasis
dermatitis as independent entity: Dermatitis at the lower leg in venous hypertension, when concurrent pathologies
are excluded; Healing of leg dermatitis on elimination of venous hypertension; Plausible pathophysiological explanation for the stasis dermatitis.
Patient series
We retrospectively studied a consecutive series of 38 patients who were referred to our phlebology consultation for treatment of lower leg dermatitis in the absence of venous ulceration or other kinds of chronic wounds (period January 2004–December 2007). Every patient at this consultation received a thorough vascular examination with duplex ultrasound scanning of the superficial and deep venous system. We then extracted those 22/38 patients who were found to have had an incompetent great or short saphenous vein (GSV/SSV), and who also had patch tests performed to the common allergens most relevant in phlebology. Patch testing included standard series, desinfectants and preservatives, ointment vehicles and emulsifiers, pharmaceuticals/antibiotics/antiseptics/antimycotic agents, topical steroids, cosmetics, fragrances, rubber, as well as specific ointments used by each patient (own samples) (Figure 1). Patients were allowed to use emollients and topical class 2-glucocorticosteroids until the time of surgery (requirement of the Ethics Committee). The conduction of this retrospective study was approved by the local Ethics Committee.
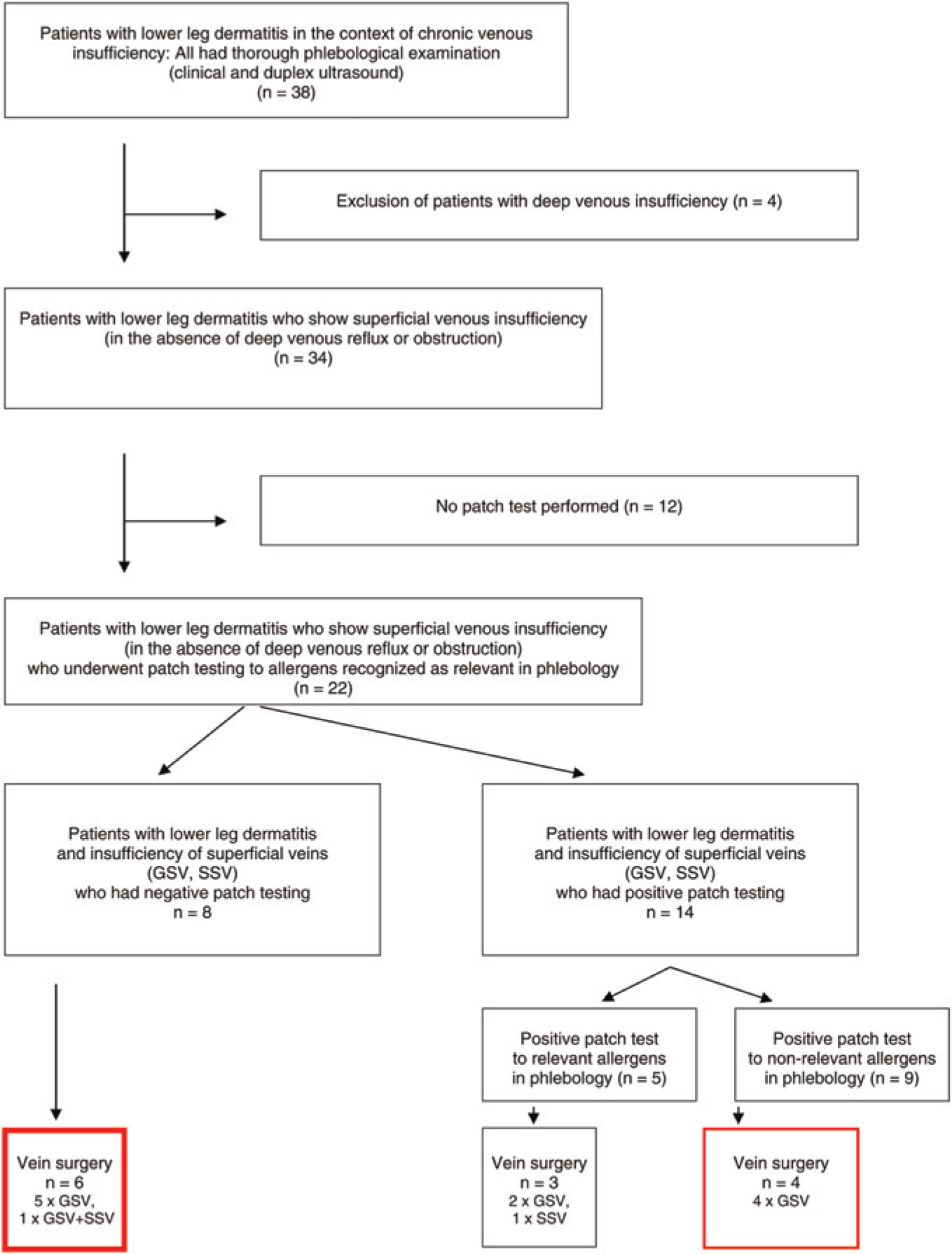
Flowchart of the study. GSV, great saphenous vein; SSV, short saphenous vein
Among the 22 selected patients, 8/22 had a completely negative patch test. Six patients in this group (6/8) underwent classical vein surgery for their superficial venous reflux, including ligation of proximal point of reflux (commonly a flush ligation at the groin) and saphenectomy of incompetent superficial vein segments. In all six patients, the lower leg dermatitis healed rapidly, completely and without recurrence during an observation period of one year (Figures 2a and b).
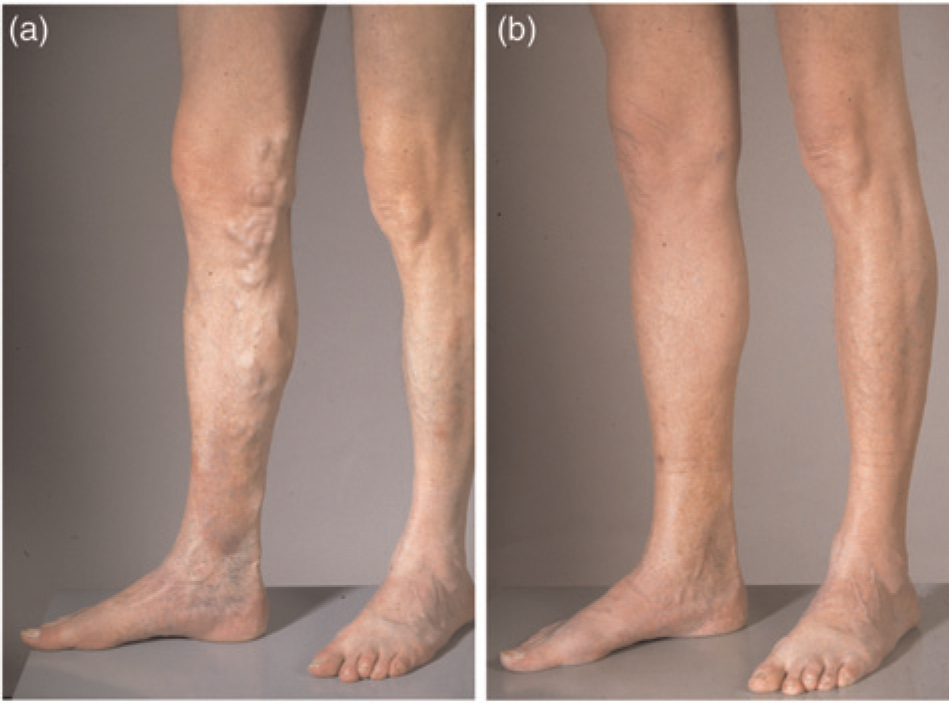
Patient V.K, a 64-year-old male patient; Stasis dermatitis with a negative patch test, before (a) and after treatment with flush ligation and saphenectomy (b)
The remaining 14/22 patients had positive reactions to patch tests (Table 1). Five (5/14) had sensitizations to allergens that are recognized to play a role in the context of phlebological pathologies (Table 1), and the other nine (9/14) were considered to have irrelevant sensitizations (cf Table 1, 2nd column).
Summary of positive patch test results
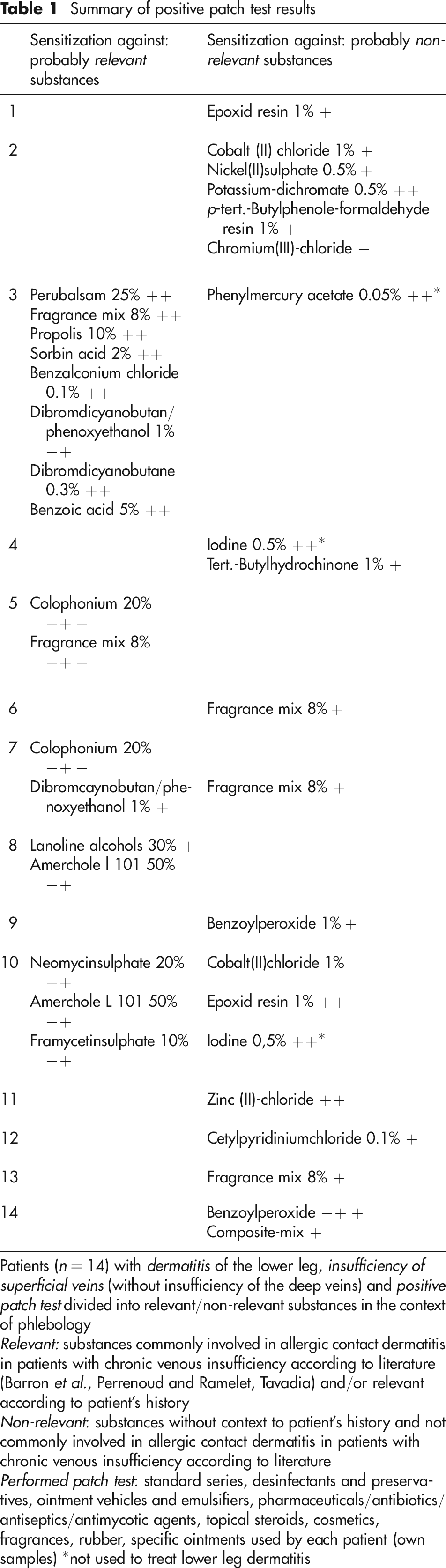
Patients (n = 14) with dermatitis of the lower leg, insufficiency of superficial veins (without insufficiency of the deep veins) and positive patch test divided into relevant/non-relevant substances in the context of phlebology
Relevant: substances commonly involved in allergic contact dermatitis in patients with chronic venous insufficiency according to literature (Barron et al., Perrenoud and Ramelet, Tavadia) and/or relevant according to patient's history
Non-relevant: substances without context to patient's history and not commonly involved in allergic contact dermatitis in patients with chronic venous insufficiency according to literature
Performed patch test: standard series, desinfectants and preservatives, ointment vehicles and emulsifiers, pharmaceuticals/antibiotics/antiseptics/antimycotic agents, topical steroids, cosmetics, fragrances, rubber, specific ointments used by each patient (own samples) *not used to treat lower leg dermatitis
Four of the nine patients (4/9) considered to have irrelevant sensitizations and in which GSV/SSV incompetence was, thus, judged the sole relevant cause of lower leg dermatitis, also underwent vein surgery. All of them experienced rapid and definite healing of their lower leg dermatitis (Figure 1).
Plausible pathophysiological explanation
Clinically there is a close relation between the occurrence of lower leg dermatitis and CVI, and approximately half of the concerned patients who get patch tests do not demonstrate any contact sensitizations. The elective presentation of (stasis) dermatitis along varicose pathways or facing incompetent perforators is another strong argument in favour of stasis dermatitis as a clinical entity. CVI and stasis dermatitis can also occur at totally different sites with venous hypertension, such as distally to a dialysis shunt.
Laboratory work also supports the observation that chronic venous hypertension can cause stasis dermatitis. In the 1980s, Thomas et al. 7 observed leukocyte trapping in extremities with venous hypertension, experimentally also in the arms. Leukocyte trapping is not only observed in panniculitis, but also in earlier stages of CVI, particularly stasis dermatitis. Peschen et al. 8 investigated disturbed interaction of leukocytes with microvascular endothelial cells. They found that the endothelial expression of intercellular adhesion molecule (ICAM)-1/vascular cell adhesion molecule-1 and their ligands lymphocyte function-associated antigen-1/very late antigen-1 on leukocytes is upregulated already in early stages of CVI, particularly stasis dermatitis and remains elevated during later stages (dermatoliposclerosis and venous ulcers). Basal keratinocytes also expressed ICAM-1 in stasis dermatitis and higher stages of CVI. 8
Conclusion
Our clinical observation in a series of patients in whom no other plausible explanation could be found for their lower leg dermatitis than venous hypertension, and in all of whom elimination of venous hypertension as an only treatment led to complete and definite healing of dermatitis, strongly supports the common clinical experience that venous hypertension can cause stasis dermatitis. Stasis dermatitis, therefore, can be regarded as a meaningful and robust clinical entity.
Footnotes
Acknowledgement
This study has been supported by a grant of the Swiss Society of Phlebology.