
Abstract
Introduction
Active venous ulcers are present in 0–0.5% of the adult Western population; 0.6–1.4% have healed ulcers. 1 The socioeconomic importance of chronic venous insufficiency (CVI) is due to the large number of patients concerned to the cost of investigations and management and to the deterioration of the quality of life (QoL) and loss of working days. 2 The magnitude of these costs depends on the severity of the venous disease. As the prevalence of CVI increases with age, societal costs also increase with age of the involved population. In clinical stages C4–C6, direct costs include treatment of skin changes, prevention of ulcer development and recurrence as well as ulcer treatment. 2
Direct costs include medical and nursing manpower, cost of investigations and of treatment. These costs can appear in hospitals or in outpatient care. There are also indirect costs related to loss of working days. Reimbursement of costs for venous diseases differs widely in different countries and is affected by government policies. 3
Overall costs for CVI
Older estimations of the overall annual costs of CVI vary from 600 to 900 million € to 2.5 billion € in Western European countries and the USA.2,4–7 This is representing 1–2% of the total health-care budget in these countries. In all, 22% of district nurses’ time is spent treating ulcers of the legs. 8 Figures for France in 1991 showed a total expenditure for CVI of 2.24 billion €, of which 41% was for drugs, 34% for hospital care and 13% for medical fees; there was a total of 200,000 hospitalizations for CVI during that year, of which 50% was for varicose veins, which was the eighth most common cause for hospitalization. These costs represented 2.6% of the total health budget for that year. 9 In Belgium, medical care costs in 1995 for chronic venous diseases amounted to 250 million €, which is 2–2.25% of the total health-care budget. 10
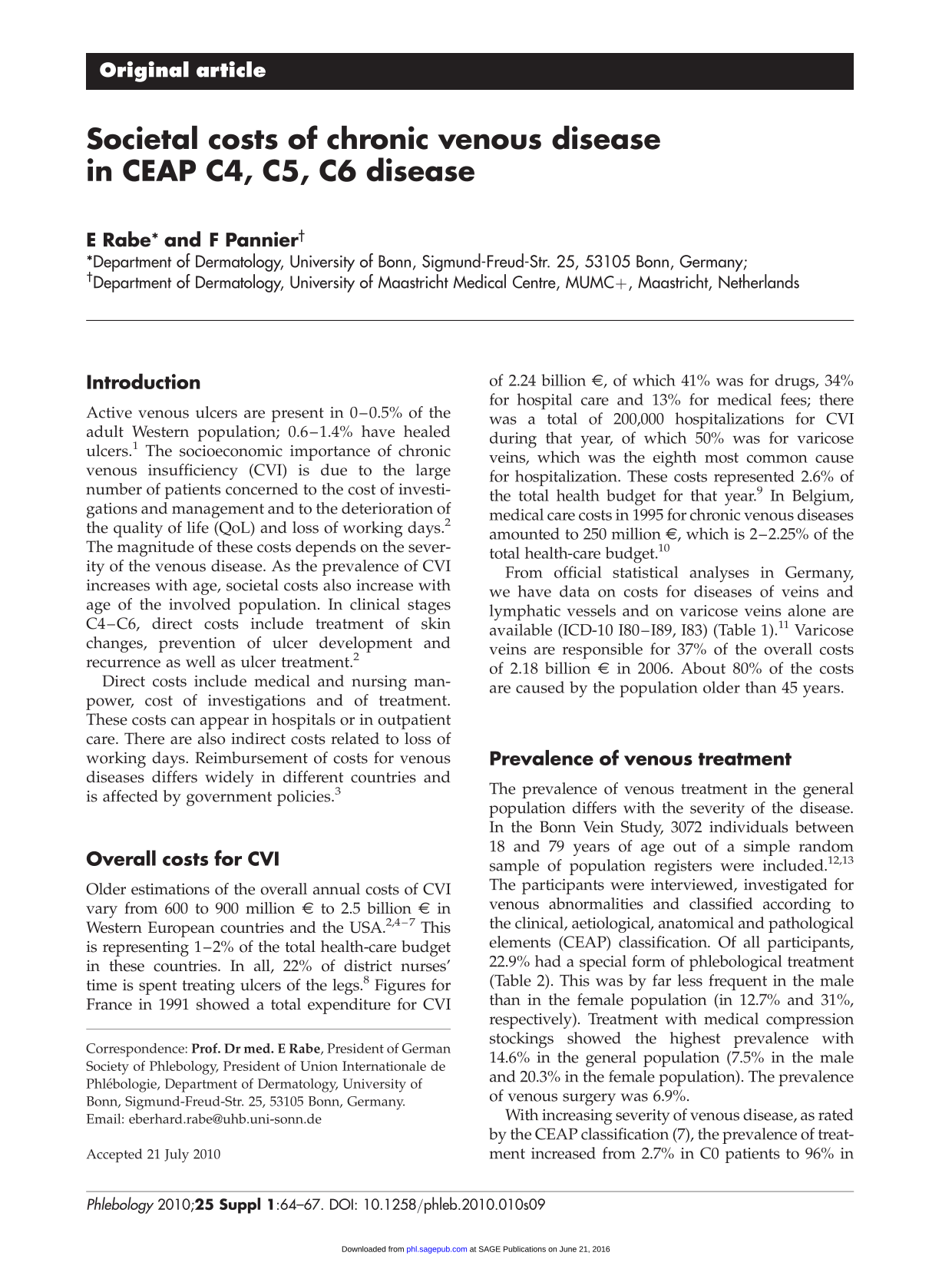
From official statistical analyses in Germany, we have data on costs for diseases of veins and lymphatic vessels and on varicose veins alone are available (ICD-10 180–189,183) (Table 1). 11 Varicose veins are responsible for 37% of the overall costs of 2.18 billion € in 2006. About 80% of the costs are caused by the population older than 45 years.
Costs of diseases of veins and lymphatic vessels (ICD-10 180–183) and of varicose veins alone (ICD-10 183) from official statistical calculations in Germany in 2002 and 2006 (in million €)
Prevalence of venous treatment
The prevalence of venous treatment in the general population differs with the severity of the disease. In the Bonn Vein Study, 3072 individuals between 18 and 79 years of age out of a simple random sample of population registers were included.12,13 The participants were interviewed, investigated for venous abnormalities and classified according to the clinical, aetiological, anatomical and pathological elements (CEAP) classification. Of all participants, 22.9% had a special form of phlebological treatment (Table 2). This was by far less frequent in the male than in the female population (in 12.7% and 31%, respectively). Treatment with medical compression stockings showed the highest prevalence with 14.6% in the general population (7.5% in the male and 20.3% in the female population). The prevalence of venous surgery was 6.9%.
Details on the therapeutic measures taken in the 3072 participants of the Bonn Vein Study

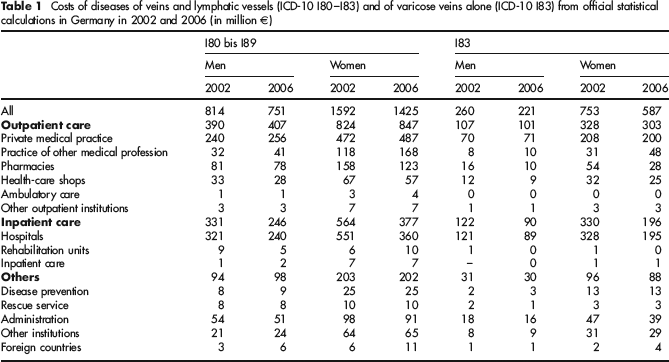
With increasing severity of venous disease, as rated by the CEAP classification (7), the prevalence of treatment increased from 2.7% in CO patients to 96% in C5/C6 patients (Table 3). More than 30% of patients with severe chronic venous insufficiency (C4–C6) had undergone a vein operation. The application of sclerotherapy and antithrombotic medication is also significantly increased in this group.
Prevalence of venous treatment in the different clinical stages (multiple entries possible; n = 3069)
CEAP, clinical, aetiological, anatomical and pathological elements
CEAP classification details lacking for three probands
Costs for ulcer treatment
A prospective study from France has broken down the cost of treating venous ulceration: of the total cost 48% was for care, 33% for medication, 16% for hospitalization and 3% for loss of work. 14 In Sweden, in 2002 the average weekly cost of a venous leg ulcer was €101 with an estimated annual cost of 73 million € for all venous ulcers. These costs were slightly less than that in previous years and were attributed to a more structured management. 15
In Germany in 2008 a prospective cost-of-illness study was performed in 23 specialized wound centres throughout Germany. 16 Direct, medical, non-medical and indirect costs to the patient, statutory health insurers and society were documented. Health-related QoL was recorded as intangible costs using the Freiburg QoL assessment for wounds. A total of 218 patients (62.1% female) were recruited consecutively. Mean age was 69.8 + 12.0 years. The mean total cost of the ulcer per year and patient was €9569 (€8658.10 [92%] direct and €911.20 [8%] indirect costs). Of the direct costs, €7630.70 was accounted for by the statutory health insurance and €1027.40 by the patient. Major cost factors were inpatient costs, outpatient care and non-drug treatments. QoL was strikingly reduced in most patients.
Loss of work days
In the USA, venous ulcers caused the loss of 2 million work days per year in 2002. 7 In France, 6.4 million days of work were lost in 1991. 9 Another study in France found that about 7% of the working population is off work because of venous disease (CEAP: C1–C6) with an overall ‘estimation’ of 4 million working days lost in a year, at an estimated cost of 320 million € to the economy.17,18 These costs were higher than the amount spent for the treatment of arterial disease.
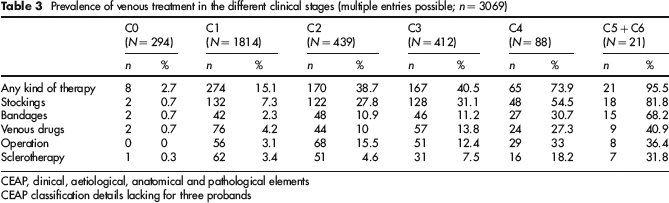
In Germany, in 2006 0.3 of 1000 female and 0.5 of 1000 male members of the biggest health insurance company (AOK) were out of work at any time due to leg ulcers. 11 The mean number of lost working days was seven in the female and 12 in the male population (Table 4).
Cases and days of work incapacity (WI) in 1000 AOK members in 2000 and 2006
Summary
Chronic venous diseases have a high impact on socioeconomic costs. Direct and indirect costs rise with the severity of the disease. As main risk factors for CVI are higher age and obesity, and the prevalence of both will be rising in the next years, the socioeconomic burden of CVI will also rise in the future. As a consequence, there is a need for early and qualified disease management. Deeper-going cost-of-illness-studies and cost-benefit analyses are necessary if management of venous ulcers is to be improved.