
Abstract
Objective
To study the relationship between the static foot disorders (SFDs) and chronic venous disease (CVD).
Material and methods
A retrospective study of 824 feet in unselected 412 patients seen by one phlebologist using a standardized record form. A complete clinical, aetiological, anatomical and pathological elements (CEAP) classification was determined. Alleged venous symptoms were recorded using a 10-point visual analogue scale and scored using a customized questionnaire. A standardized measurement of the Djian-Annonier angle was used to quantify and identify the presence of any static disorder of the foot.
Results
There were 156 men (37.8%) and 256 women (62.2%) who were included in this study. A majority of patients (59.3%) had a CEAP classification of C3 or greater. Static disorders of the feet were found to be very common in the study population: 137 feet were hollow feet (16.6%) and 120 flat feet (14.5%). Thus, 31% of all of the feet had some form of SFD. A significant correlation was found between the incidence of SFD and body mass index (P < 0.01), the presence of symptoms (P<0.001) and prolonged standing during the day (>5 hours, P < 0.05). The severity of the CVD, represented by the CEAP clinical classes, was also found to be very significantly related to the SFD (P < 0.001). This correlation was found to be independent of age.
Conclusion
Static disorders of the foot can be considered as an important risk factor that negatively affects CVD. In daily practice, it is often underestimated. This emphasizes the crucial importance of the detection of SFD during the clinical exam of all CVD patients. Correction of static disorders of the feet will improve symptoms due to the SFD, as well as those related to venous stasis. These results can easily be explained by improvement of foot pump efficacy during walking.
Introduction
Static foot disorders (SFDs) are commonly found in the general adult population. Their prevalence varies with age: 23%, according to Harris and Beath; 1 8–15%, according to Walker and Fan; 2 and as much as 26.5%, according to Otsuka et al. 3 in 340 Japanese subjects in their seventh decade.
When walking with a SFD, the foot makes contact with the ground in a abnormal fashion; one's posture is also affected, as well. Static disorders of the foot can easily be detected by the clinical exam, but it is necessary to quantify them with a footprint and/or radiographic examination. A prospective study conducted by Maes et al. 4 on 79 subjects showed a good correlation between eight podometric and three radiologic parameters of the plantar arch. The footprint parameters included the arch angle; Chippaux-Smirak's index; Quamra's contact indices 2, 3 and 4; Schwartz's footprint angle; Staheli's arch index; and the arch length index. The three radiological parameters were as follows: the Djian-Annonier angle, Méary's angle and the calcaneus inclination. The footprint parameters were found to correlate best with Djian's angle and the calcaneus inclination. 4 In our study, Djian's angle was used to assess and quantify the SFD.
The aim of this study is to establish the possible relationship between the foot static disorder (FSD) and chronic venous disease (CVD).
The anatomical studies of the foot pump suggest that the pedal venous reservoir is located in the lateral plantar veins. 5–7 When the sole of the foot presses on the ground, the lateral plantar veins are emptied and blood is forced up into the posterior tibial veins. Hence, the presence of an SFD could be a good explanation for the impairment of venous return during ambulation.
The role of the foot venous pump could be crucial in CVD patients since venous return starts with the foot when one walks.
Material and methods
Unselected patients, aged 18 or more, seeking medical care for CVD of the lower limbs were included in this study.
A customized computer programme was used, the Computer Venous Registry, 8 to provide an automated clinical, aetiological, anatomical and pathological elements (CEAP) classification and scoring of the symptoms for each limb. Data entered for each patient included the examination date, birth date, sex and body mass index (BMI). All patients were assessed by a Duplex colour examination of the superficial and deep system. Complete CEAP clinical classification 9 was documented, using the definitions proposed by the expert panel at the 2001 world meeting of the International Union of Phlebology (UIP) in Rome. 10 Venous symptoms were also carefully documented using a 10-point visual analogue scale. Symptoms assessed included pain, heaviness, swollen feeling, pruritus, cramping and burning. Additionally, leg symptoms and their occurrence were assessed with a customized questionnaire that allowed for scoring of the symptoms. 11
The computerized programme used for this study facilitated complete record taking by asking for missing items. It also provided illustrations of clinical items when requested by the user. Beyond that, the programme asked for additional clinical items, when necessary. Ankle stiffness was evaluated by physical examination and was assessed in three severity grades (0 = absence, 1 = reducible ankylosis or ankle stiffness, 2 = non-reducible ankylosis).
Measurement of the Djian-Annonier angle 12 allowed for quantification of any SFDs that were found. The Djian-Annonier angle is defined as an angle that is created by three specific points when the patient is standing. The first point is the lower point of the calcaneus; the second is the lower point of the talo-navicular joint; and the third is the impact point of the medial sesamoid bone (Figure 1). A standardized measurement protocol was used by the same radiologist, not aware of the CEAP class of the patient (Figure 2). The data from 824 limbs (412 patients) were analysed to evaluate the relationship between the SFD, BMI, CEAP clinical class, and the other clinical parameters of chronic venous insufficiency (CVI).
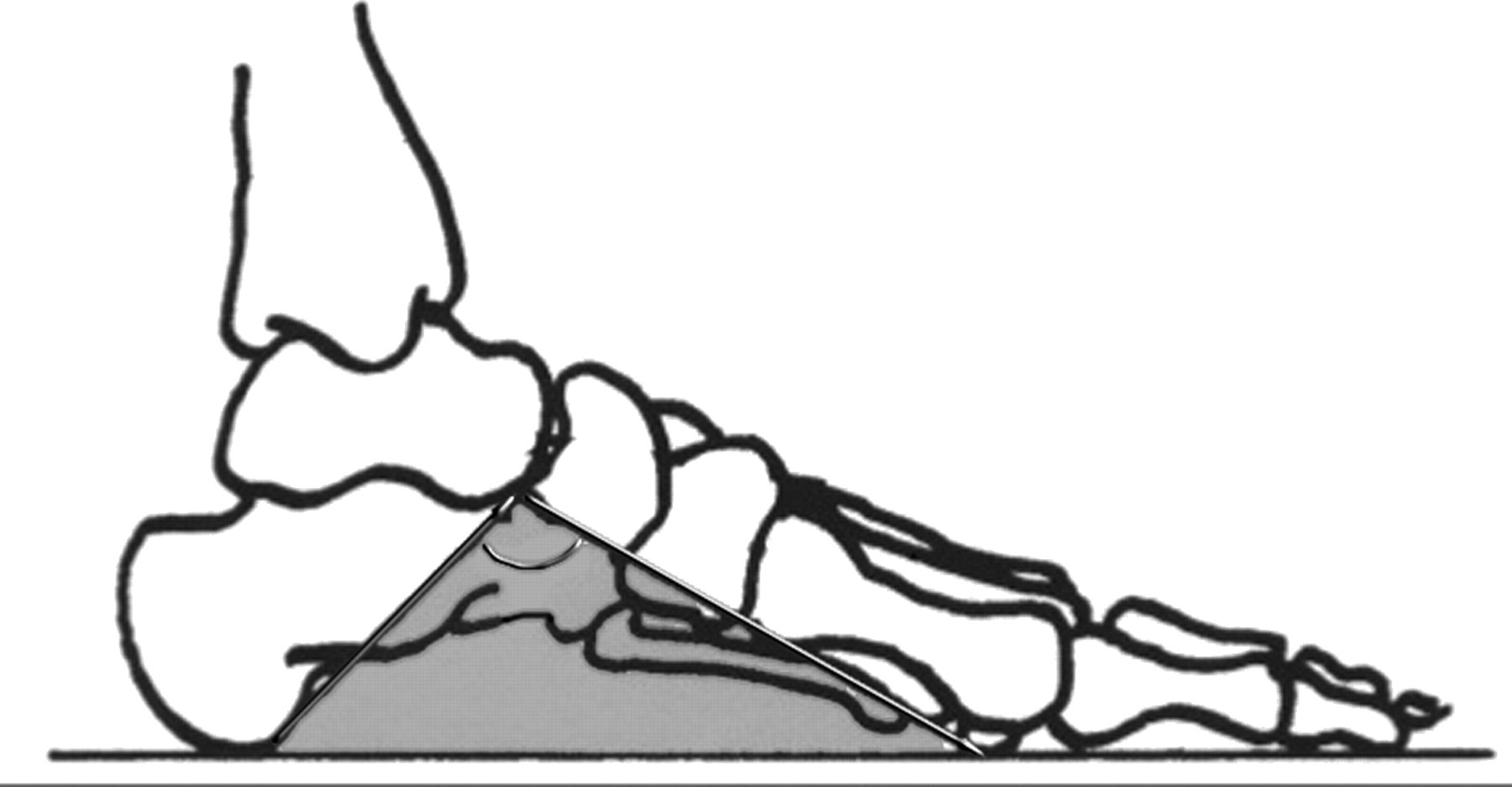
The Djian-Annonier angle is defined as the angle that is formed by three specific points in the standing patient: the lower point of the calcaneus, the lower point of the talus-navicular joint and the impact point of the medial sesamoid bone
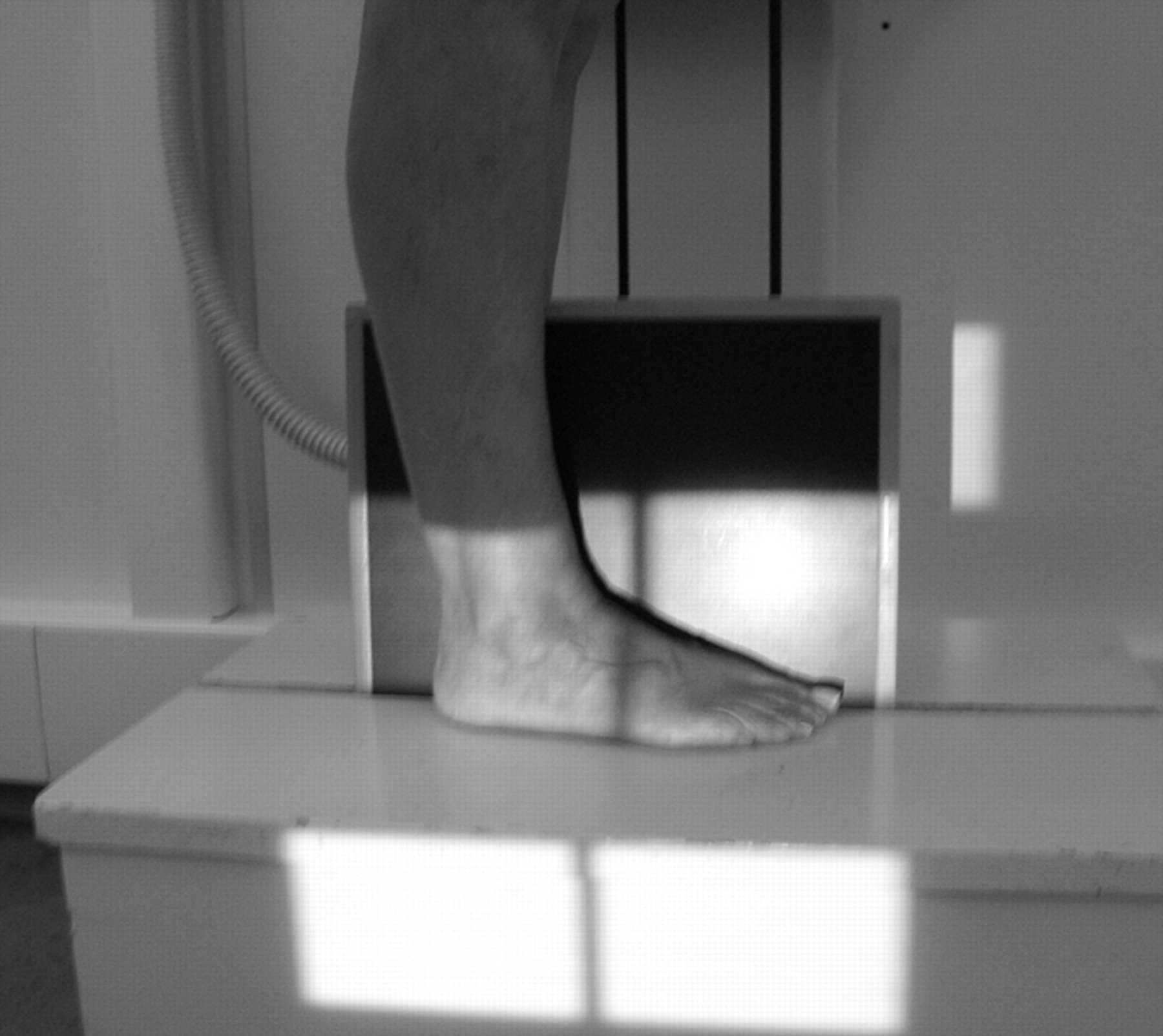
Radiological protocol for measuring the Djian-Annonier angle in the standing position
Statistical analysis
Quantitative variables and percentages are described using numerical means plus or minus (±) the standard deviation, and χ2 testing was performed on the quantitative variables that were used in characterizing SFD according to right or left leg, CEAP clinical class and age. Due to the relationship between CEAP clinical class and age, the relationship between SFD and CEAP clinical class was studied with χ2 testing for different age classes and logistic regression. This allowed the odd ratio of CVD to be identified when a patient has a hollow foot or a flat foot. The threshold of <119° and >128° for Djian's angle was chosen on the basis of the first and ninth deciles of the population distribution. In other words, 80% of the population had a Djian's angle that is between 119° and 128° and could be called ‘normal’ in the statistical point of view, while 10% have an angle that is below 119°, and 10% have an angle that is above 128°. These thresholds are exactly the same as those used in the study of Maes et al. 4
The statistical analysis was performed using SAS software, version 9.2. The level of significance of α is 5%.
Results
The series consisted of 412 patients with recorded clinical data and standardized measurement of Djian's angle. There were 268 women (82.4 %) and 156 men (17.6%). Their mean BMI was 26.4 and 25.9 with a standard error of 0.1 and 0.15, respectively.
Distribution of CEAP clinical (C) classes
Figure 3 shows that a majority (59.3%) of patients had CVI classified as C3 or greater. This could be related to the fact that a high percentage of patients were retired and, therefore, had an older average age. The comparison of the CEAP clinical (C) classes on both legs showed significantly more advanced CVD (P < 0.01) on the right side than the left (Table 1). Limbs without CVD (C0: 1.5%) or with little CVD (C1: 18.8%) were also included in this series since a systematic bilateral examination was performed even when a patient presented with unilateral telangiectases (C1). This group of normal patients together with the controlateral limbs C0–C1 of unilateral CVD patients (C2 or more) acted as the normal control group and was compared with the group of true CVD limbs (C2–C6) in studying the relationship between CVD and SFD.
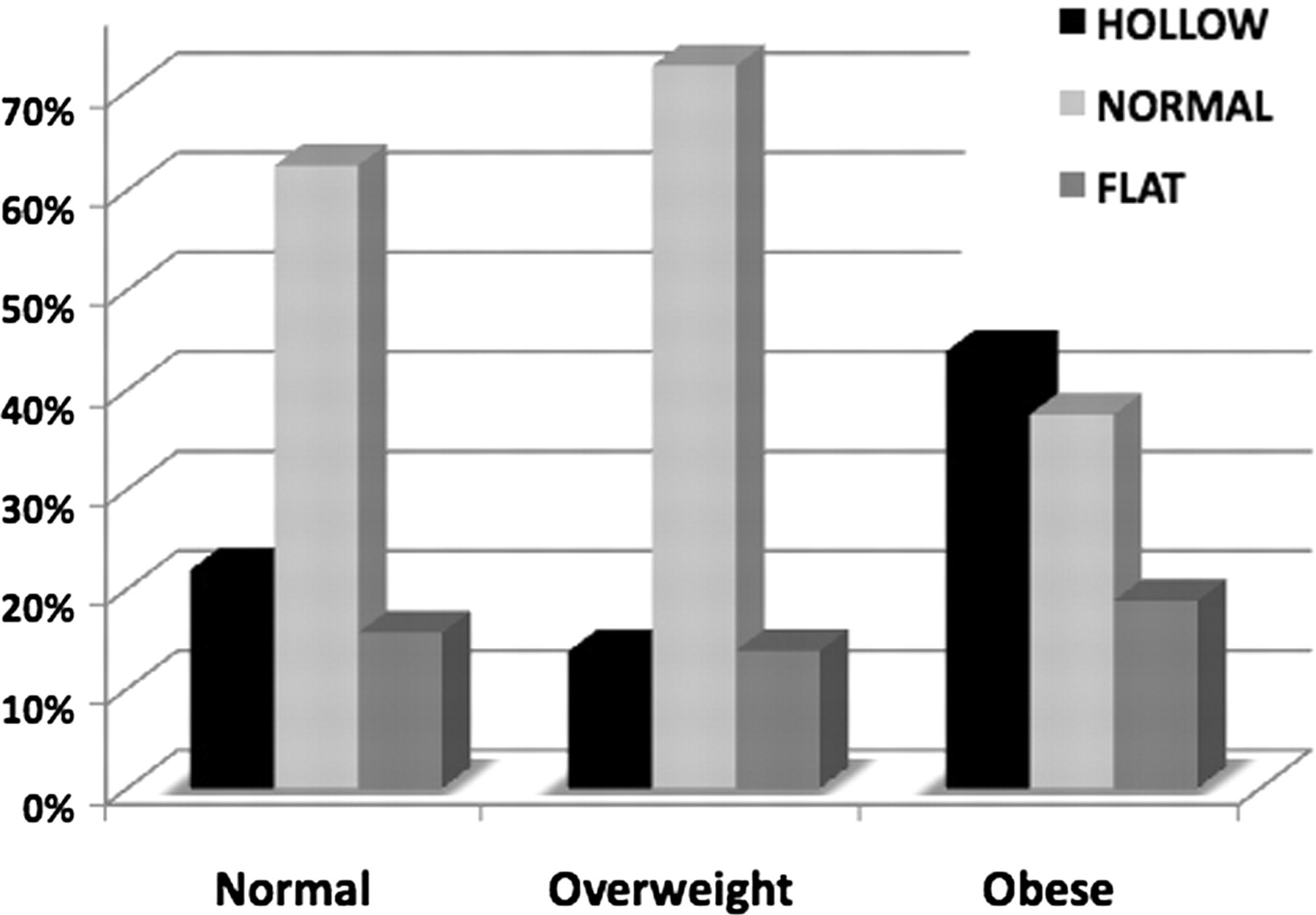
Prevalence of static foot disorder according to patient body mass index (BMI), divided into three subclasses. Normal = BMI < 25; overweight = 25 < BMI < 30; obese* = BMI > 30 (*P < 0.0001) (χ2)
Division of CEAP clinical (C) classes of both legs
CEAP, clinical, aetiological, anatomical and pathological elements.
More advanced C classes are found on the right side (P < 0.01)
We found no ankle stiffness, even in the group of 10 patients with an active ulcer.
Distribution of SFDs
Static disorders of the foot were found in 31% (257/824) of limbs. This included 16.6% with hollow feet, or pes cavus, and 14.5% with flat feet, or pes planus. The comparison of both limbs (Table 2) showed an asymmetry of SFD, with the right foot being affected more than the left (P < 0.001). This could be related to the fact that CEAP clinical class severity was also found to be more frequent on the right side. The comparison of each type of SFD, with regard to side (Table 3), showed both feet to be normal in 50% of the patients, with unilateral disorders in 38% and bilateral in 12%. The overall prevalence of SFD in this study was 31%; however, if consideration were only given to those patients who were C2 or more, the prevalence of SFD would have been 38%.
Distribution of static foot disorders found in the 412 patients
There is more static foot disorder (both flat and hollow) on the right side (P < 0.001)
Distribution of static foot disorders according to type and side
Relationship between CEAP classes and SFD
The incidence of SFD in those with or without CVD (Table 4) was higher in the CVD group (P < 0.0001, χ2). In order to eliminate the age factor, we studied the incidence of FSD in four age groups (Table 5): we found a significantly higher incidence of SFD in the three older age groups (P < 0.001). The exception to this finding was the youngest age group (<30 year old, NS). Logistic regression with age adjustment more precisely quantified the relationship between the different static disorders of the foot and CVD (Table 6): patients with hollow foot had an odd ratio of 4.2 for CVD (regardless of age) and patients with a flat foot had an odd ratio of 3.1 for CVD (regardless of age).
Relationship between SFD and CVD
SFD was significatively more common in the CVD group when compared with the group with limbs C0–C1 (P < 0.0001, χ2)
SFD, static foot disorder; CVD, chronic venous disease
Comparison of SFD according to CVD disease, using χ2 testing for different subgroups by age
NS, non-significant; SFD, static foot disorder; CVD, chronic venous disorder; CEAP, clinical, aetiological, anatomical and pathological elements
Logistic regression analysis of the influence of FSD on CVI severity adjusted on age
FSD, foot static disorder; CVI, chronic venous insufficiency
Influence of the other factors on SFD
Sex, age, personal history and symptom specificity scoring were not significantly related to SFD. To study the relationship between Djian's angle and BMI, patients were divided into three groups: normal (BMI<25), overweight (25<BMI<30) and obese (BMI>30). The results (Figure 3) showed a higher incidence of hollow foot in the obese group (P < 0.0001, χ2). The incidence of the SFD, based on occupation and long-standing position (Figure 4), showed a higher incidence of hollow foot in the standing group (P < 0.001, χ2).
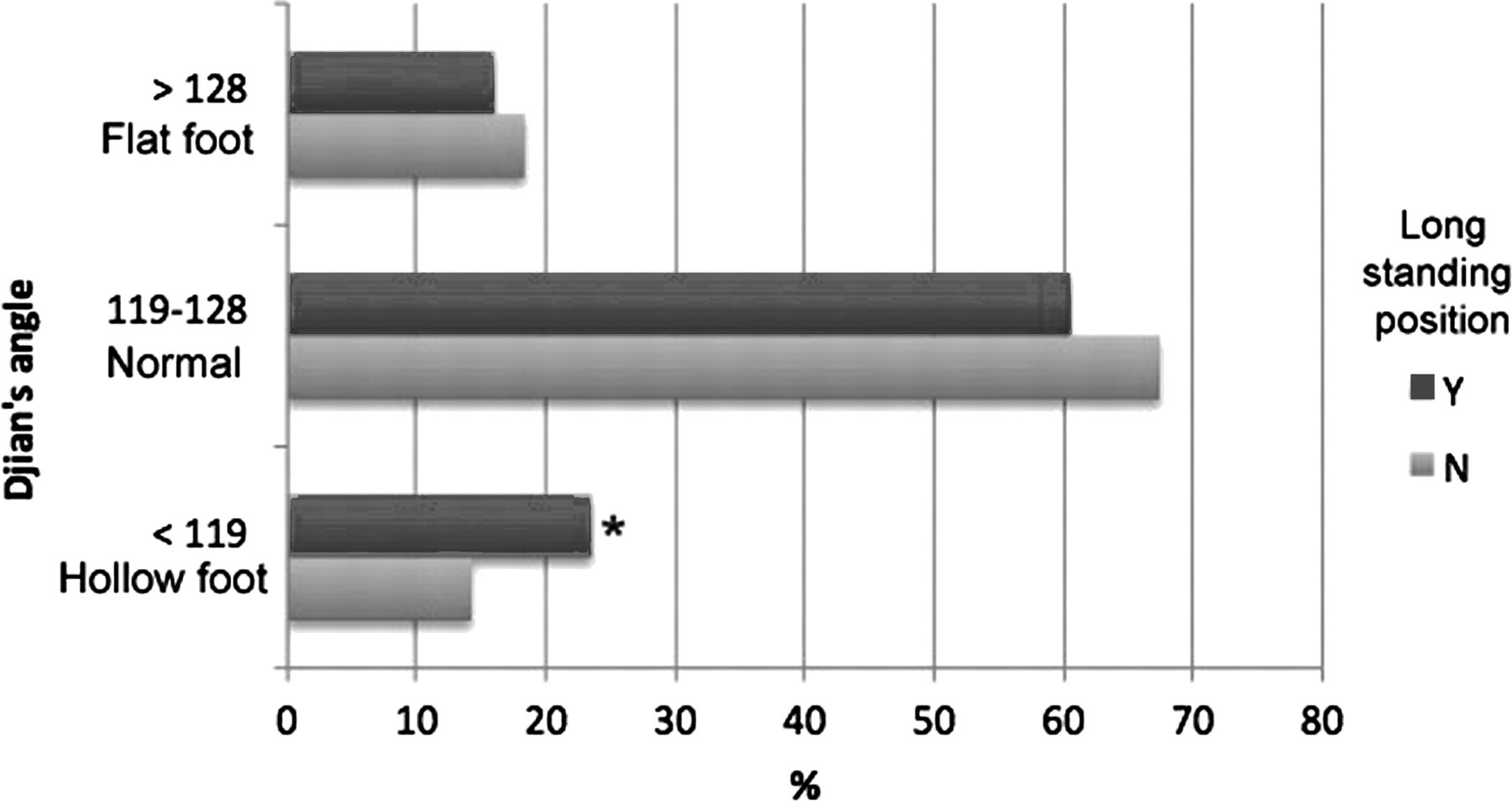
Prevalence of Djian's angle according to occupation and longstanding position. Flat foot and normal are NS. *Hollow foot, P < 0.001 (χ2). NS, non-significant
Discussion
Validity of the results: interpretation of a bias in our data
There are significantly more FSD on the right side. This higher rate of SFD in the right foot could be explained by the higher prevalence of severe CVD seen in the right limb.
The ‘control group’ selected in this study cannot really be considered as ‘normal’ patients. However, about half of the patients of this group were free of venous disease in either limb (<C2). For this reason we think the control group could be considered as representative of all individuals' limbs without CVD.
Possible origin of the symptoms
Several authors have reported that flat feet (pes planus) and hollow feet (pes cavus) are associated with pain. 13–16 However, there is a need for further study to investigate the role played by any associated venous impairment in causing pain. Our study demonstrated the relationship between SFD and CVD; however, the question of which symptoms might be related to foot disorders and which might result from venous disease remains to be answered. The best way to answer the question would be to treat the patient's SFD and/or their CVD and evaluate the clinical result. A new French randomized controlled trial that hopes to address this issue is in progress.
Anatomical explanation of SFD as a risk factor of CVD
The role of the foot venous pump is crucial in CVD patients since venous return starts with the foot when one walks. 14 The anatomy of the foot pump suggests that the pedal venous reservoir is located in the lateral plantar veins. 15 When the sole of the foot presses on the ground, the lateral plantar veins are emptied and blood is forced up into the posterior tibial veins. Hence, the presence of a SFD could be a good explanation for the impairment of venous return during ambulation.
Conclusion
The prevalence of FSDs is underestimated in our patients consulting for CVD.
The relationship between FSD and the severity of CVD is significant. In other words, the presence of FSD could be considered as an important factor contributing to worsening the CVD.
The hollow foot, or pes cavus, seems to be more frequently related to CVD and obesity than flat foot or pes planus.
Due to their high prevalence, about 38% in this study, the SFD should be checked in any CVD patient, especially in case of obesity.
Awareness of the association between SFD and CVD is of crucial importance in daily practice. This is especially true for flat foot which is easily corrected: correction of the SFD by orthotics will improve the symptoms related to CVD. This could easily be explained by improvement of the foot pump function while walking.
Footnotes
Acknowledgements
We thank Ted King MD for his advice and re-reading this paper and this French Society of Phlebology for supporting this study.