
Abstract
The correct and precise nomenclature of the veins of the lower extremity is a necessary tool for communication. Three important changes have been done over the last 13 years. Terminologia Anatomica, the latest version of the Latin anatomical nomenclature, was published in 1998, extended in the area of the lower extremity veins with two consensus documents, in 2001, during the 14th World Congress of the International Union of Phlebology and in 2004 during the 21st World Congress of the International Union of Angiology. This article is a free continuation of two previous articles, reviewing the detailed anatomy and correct nomenclature of the superficial veins of the lower extremities and veins of pelvis. Now, it is concentrated on the deep venous system, in which 15 new terms have been added in both Latin and English languages.
Introduction
This article is a continuation of two previous articles by the same collection of authors who have written on the anatomy of superficial veins of the lower extremities and veins of pelvis, emphasizing their new nomenclature. 1,2 For more than 100 years the Latin anatomical terminology was standardized as a nomenclature 3–5 and its last revision was published 13 years ago in 1998, thanks to the effort of the Federative Committee on Anatomical Terminology (FCAT). This proposal was approved by the International Federation of Associations of Anatomists (IFAA) as the only valid and mandatory Latin anatomical nomenclature denominated as the Terminologia Anatomica (TA), subtitled the International Anatomical Terminology. 6 The official Latin terms, according to the TA, which are used in this article, are written in italics; on the contrary, the obsolete and unofficial terms are stated in normal case within quotation marks; finally, the English synonyms are stated within parentheses. All synonyms (in both languages) are separated with semicolons, following the manner of the TA. The English terms used are only equivalents, applied in English-speaking countries; there is no official version of the English anatomical nomenclature at all. 4,5
The development of new diagnostic and therapeutic methods, together with the introduction and spread of the clinical, aetiological, anatomical and pathological elements (CEAP) classification are a mighty impulse to extend the anatomical knowledge and terminology. 7 In 2001, the International Union of Phlebology, IFAA and Federative International Committee on Anatomical Terminology (FICAT) created the International Interdisciplinary Committee (IIC) and issued a document published as ‘Nomenclature of the veins of the lower extremities: an international interdisciplinary consensus statement’. 8 Three years later, the IIC issued the second document, aimed at the veins of pelvis and terms used in the everyday clinical practice. This document was published as ‘Nomenclature of the veins of the lower extremity: extensions, refinements and clinical application’. 9 Both documents (after the IFAA approval) changed, extended and completed the current pool of TA terms and will be incorporated in to TA in its next planned edition. 8–11 The new terms have not yet received the unique identification number of TA.
The veins of the lower extremities can be classified into three independent and yet interconnected systems, which finally gather and drain the blood into the vena iliaca externa and later into the vena cava inferior. They are the superficial venous system; 1 deep venous system; and their mutual connections, called the perforating veins or perforators. These systems are situated within separated space, called compartimentum (compartment). The TA listed only terms of individual compartments containing muscles groups (Table 1). The deep compartment, delineated by muscle fasciae, contains the deep venous system, which accompanies arteries. The deep veins of the lower extremity are regularly doubled as high as the level of the vena poplitea. 12
Compartments of the lower extremity
Compartments of the lower extremity
Table 2 summarizes the terminology of the deep venous system of lower extremity according to TA 1998 (terms with the identification number) and the revision of the IIC 2004.
Nomenclature of the deep veins of the lower extremity according to the TA 1998 (terms with the identification number) and according to the revision of the IIC 2001 and 2004
Terms pointed out with asterisk (*) are former TA terms changed by the IIC
Venae profundae membri inferioris (deep veins of lower extremity)
The deep veins of the lower extremity accompany the corresponding arteries and their branches. They contain a large number of valves (valvulae in Latin) within their course (Figure 1).
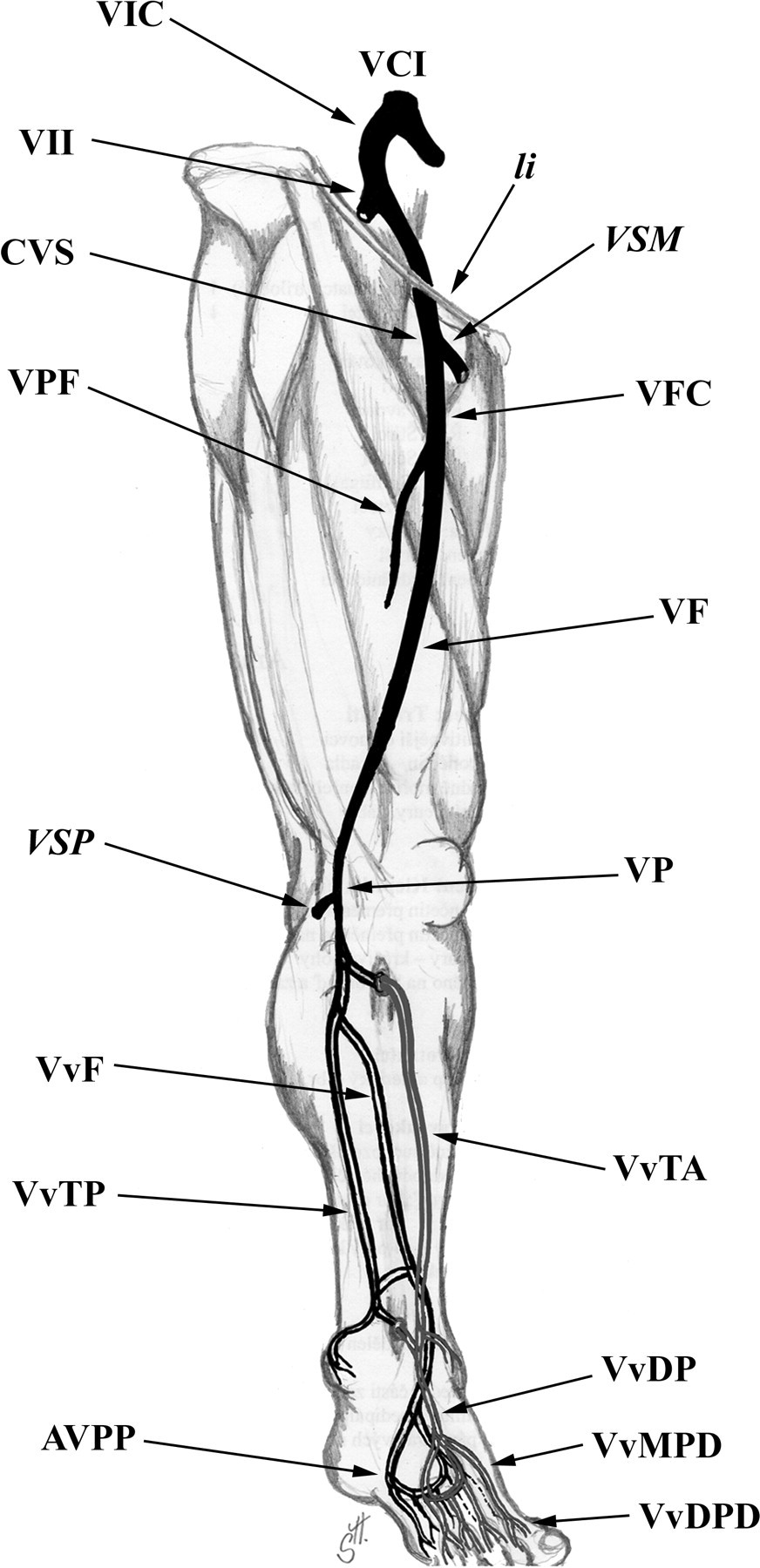
The scheme of the deep system of the lower extremity. AVPP, arcus venosus plantaris profundus; CVS, confluens venosus subinguinalis; li, ligamentum inguinale; VCI, vena cava inferior; VF, vena femoralis; VFC, vena femoralis communis; VIC, vena iliaca communis; VIE, vena iliaca externa; VII, vena iliaca interna; VP, vena poplitea; VPF, vena profunda femoris; VSM, vena saphena magna; VSP, vena saphena parva; VvDP, venae dorsales pedis; VvDPD, venae diigtales profundae dorsales; VvF, venae fibulares; VvMPD, venae metatarsales profundae dorsales; VvTA, venae tibiales anteriores; VvTP, venae tibiales posteriores
Venae digitales profundae plantares (plantar deep digital veins) drain the plexuses on the plantar side of the toes, communicate with the venae digitales profundae dorsales and join to form four venae metatarsales profundae plantares (plantar deep metatarsal veins). These run inside the intermetatarsal space and communicate with corresponding veins on the foot dorsum (venae metatarsales profundae dorsales (dorsal deep metatarsal veins). They are often incorrectly called the ‘venae perforantes’, although these veins are situated within the deep compartment and hence do not pierce any fascia (which is the principal identification mark of the real perforantes). 13 The venae metatarsales profundae plantares continue proximally and form the arcus venosus plantaris profundus (deep plantar venous arch), which accompany the arterial arcus plantaris. The venae plantares laterales et mediales (lateral and medial plantar veins) leave this arcade proximally and follow the corresponding arteries. Afterwards, they send off communications to the vena saphena magna et parva (great and small saphenous vein), enter the canalis malleolaris (malleolar canal; tarsal tunnel) together with the nervus tibialis (tibial nerve), situated dorsally to the malleolus medialis (medial malleolus). The medial and lateral veins merge within the malleolar canal and form the venae tibiales posteriores.
At the dorsum of foot, the veins commence in the same manner as the plantar ones. The venae digitales profundae dorsales (dorsal deep plantar veins) gather the venous blood from minute venous plexuses and communicate with the corresponding deep plantar veins. Afterwards, they merge into four venae metatarsales profundae dorsales (dorsal deep metatarsal veins), which successively join and form the venae dorsales pedis (pedal veins), which run on both sides of the arteria dorsalis pedis (dorsalis pedis artery) together with the nervus fibularis profundus (deep fibular nerve; deep peroneal nerve). In case of the arteria arcuata (arcuate artery) existence, it is accompanied by veins; however, this arterial variation is present in 5% of cases only. 14 The valvules of the foot veins are oriented to enable the blood flow from the depth to the surface, unlike the leg and thigh ones, which valvules are oriented conversely, enabling the blood flow from the surface deep into the deep venous system. 15 There are more valvules within the deep system in comparison to the superficial one and they are situated just at the estuary into the larger collecting vein. 16,17
Venae tibiales posteriores (posterior tibial veins)
They accompany the corresponding artery, receive tributaries from the posterior group of the calf muscles (musculus triceps surae, musculus tibialis posterior, musculus flexor digitorum longus et musculus flexor hallucis longus), especially communications from the venous plexus inside the musculus soleus (venae soleales), from the venae perforantes and in the proximal quarter of the calf from the venae fibulares (Figures 2 and 3). Afterwards, the venae tibilaes posteriores pass underneath the arcus tendineus musculi solei (tendinous arch of soleus) together with the nervus tibialis. The veins contain 8–19 valves. 18
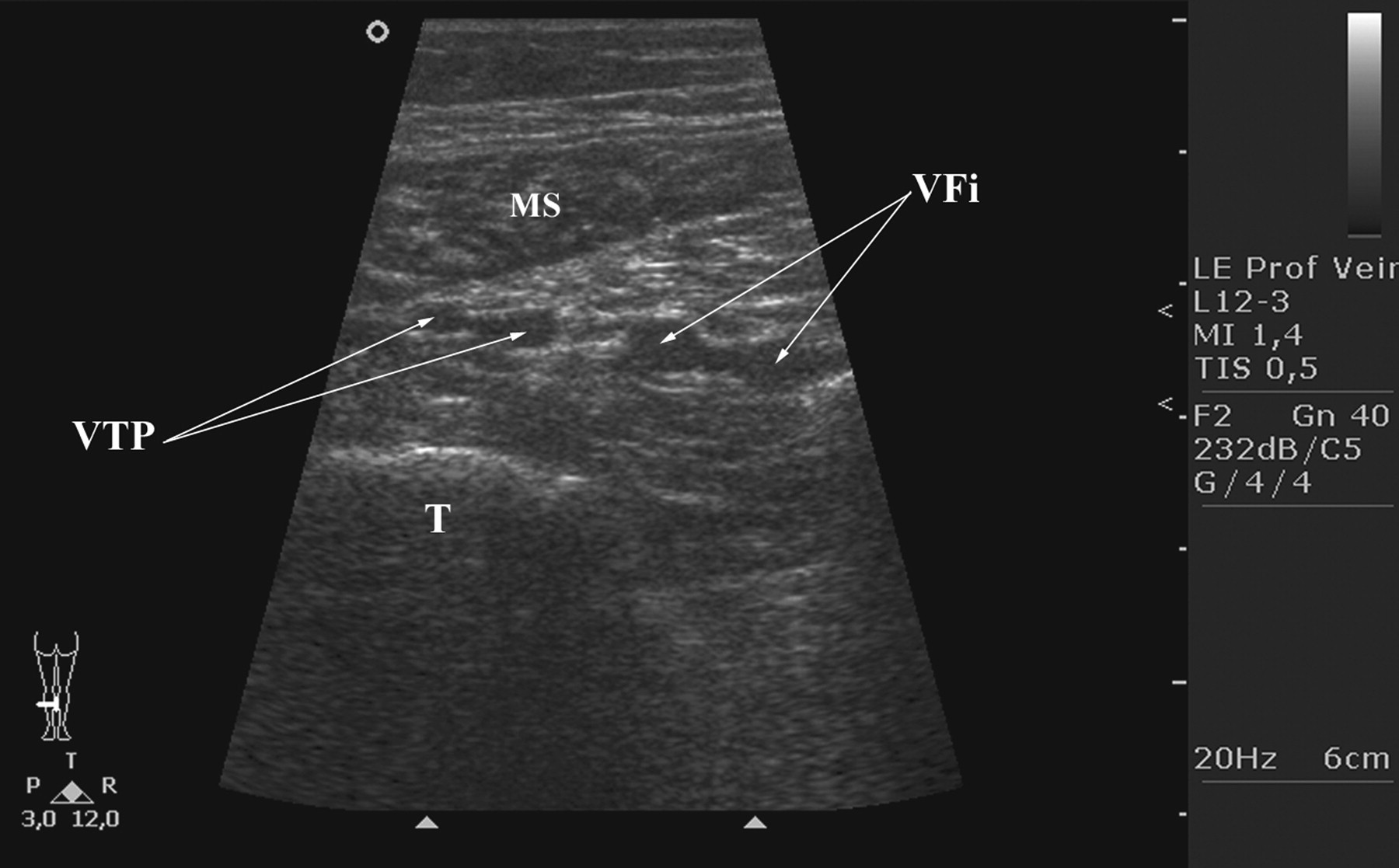
The ultrasound image of the deep veins of distal calf. MS, musculus soleus; T, tibia; VFi, vena fibularis ; VTP, vena tibialis posterior

The ultrasound image of the deep veins of distal calf. AFi, arteria fibularis; ATP, arteria tibialis posterior; MS, musculus soleus; T tibia; VFi, vena fibularis; VTP, vena tibialis posterior
Venae fibulares; venae peroneae (fibular veins; peroneal veins)
The term ‘fibular’ is now preferred to as ‘peroneal’. 4,6 They ascend along the corresponding artery within the canalis musculofibularis (‘canalis musculoperoneus; canalis Hyrtli’) between the musculus flexor hallucis longus and fibula, and collect blood from the musculus soleus (as the venae soleales) and from the venae perforantes. Finally, they drain into the venae tibiales posteriores, in the proximal quarter of the calf below the level of the arcus tendineus musculi solei (Figures 2 and 3). The veins contain 8–11 valves. 18
Venae tibiales anteriores (anterior tibial veins)
These veins are the proximal continuation of the venae dorsales pedis after passing under (dorsally to) the retinaculum musculorum extensorum inferius (inferior extensor retinaculum). They then continue along the corresponding artery and nervus fibularis profundus (deep fibular nerve; deep peroneal nerve), first on the anterior surface of the tibia and later on the anterior surface of membrana interossea cruris (interosseous membrane of leg), fixed with connective tissue vincula and hidden under the foot extensors. At the proximal end of the membrana interossea cruris, i.e. at the collum fibulae, the vasa tibialia anteriora (without the nerve) pierce the membrane dorsally into the flexor compartment. Here, the venae tibiales anteriores merge with the venae tibiales posteriores and form the vena poplitea at the distal end of the musculus popliteus. The veins contain 8–11 valves. 18
Vena poplitea (popliteal vein)
It ascends through the whole fossa poplitea (popliteal fossa) as high as the hiatus adductorius (‘hiatus tendineus’, adductor hiatus; adductor foramen; tendinous hiatus) within the insertion of the musculus adductor magnus (passing the hiatus it changes its denomination into the vena femoralis). Distally, the vein is located medially to the artery, between both heads of the musculus gastrocnemius situated dorsally to the artery (i.e. superficially) and finally proximally, its position is posterolateral to the arteria poplitea (Figure 4). Within its course it receives several tributaries: vena saphena parva, plexus venosus genicularis and muscular veins (venae gastrocnemii). It usually contains 1–4 valves and its trunk can be doubled in 5–20% of cases.
18,19
The term venae surales (sural veins) is not sufficient to describe the complexity of the venous arrangement in the calf region and is reserved for description of the these veins as a whole system. The new classification includes the following groups of veins:
Venae soleales (soleal veins)
Vena(e) solealis/es drain(s) the flat head of the musculus triceps surae – musculus soleus – and empties/y either into the venae tibiales posteriores or into the venae fibulares;
Venae gastrocnemii (gastrocnemius veins)
Venae gastrocnemii often merge into one trunk emptying into the vena poplitea close before the estuary (termination) of the vena saphena parva, either into their confluens or separately into their bifurcation;
vena medialis gastrocnemii (medial gastrocnemius vein) – larger caliber;
vena lateralis gastrocnemii (lateral gastrocnemius vein) – smaller caliber;
vena intergemellaris (intergemellar vein) – ascending between medial and lateral head of the musculus gastrocnemius directly deep to the vena saphena parva (Figures 5 and 6).

The ultrasound image of the deep veins of the fossa poplitea. AP, arteria poplitea; f, fascia; NT, nervus tibialis; VP, vena poplitea
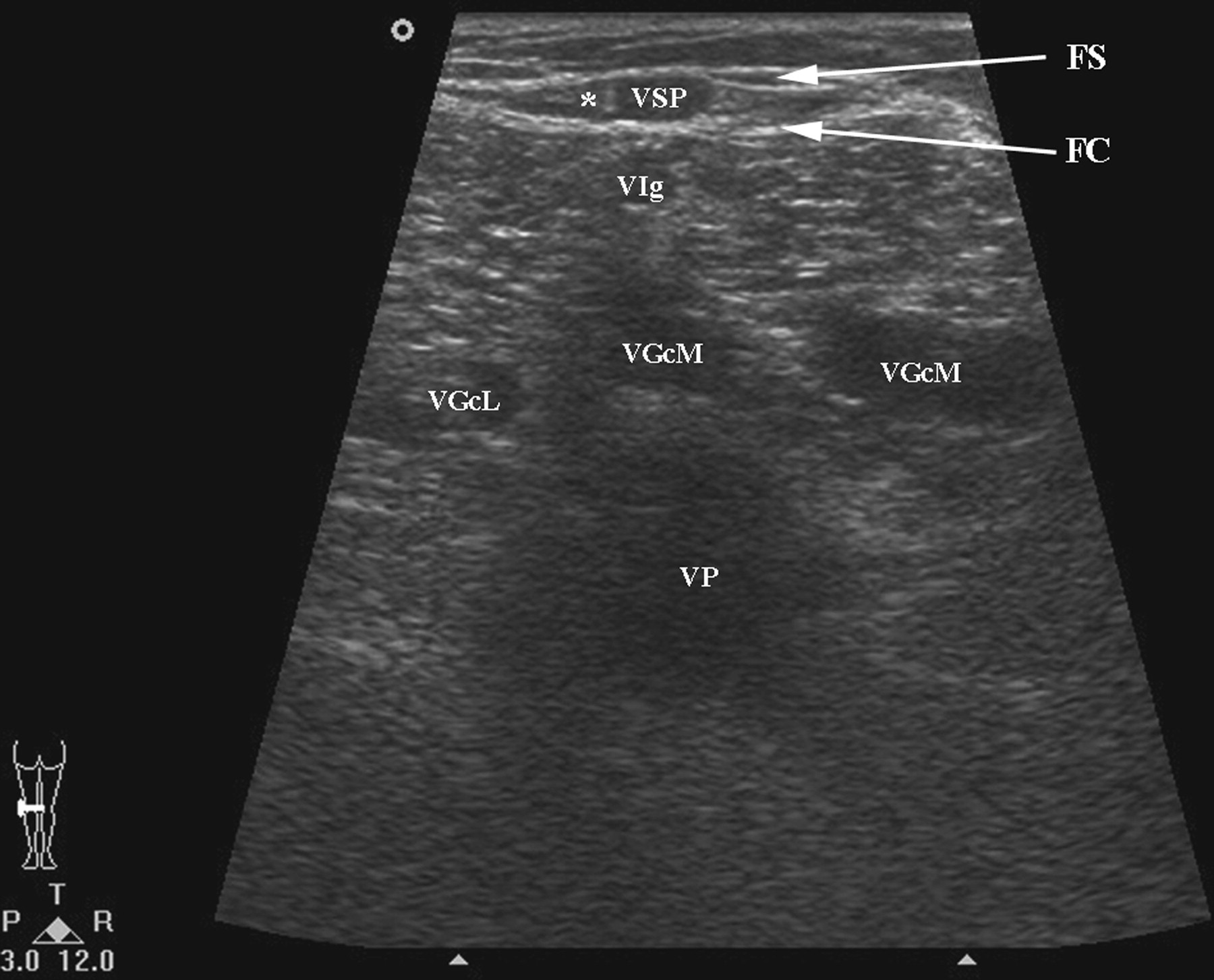
The ultrasound image of the deep veins of the proximal calf. FS, fascia saphena; FC, fascia cruris; VIg, vena intergemellaris; VGcM, vena gastrocnemia medialis; VGcL, vena gastrocnemia lateralis; VP, vena poplitea; VSP, vena saphena parva; *compartimentum saphenum
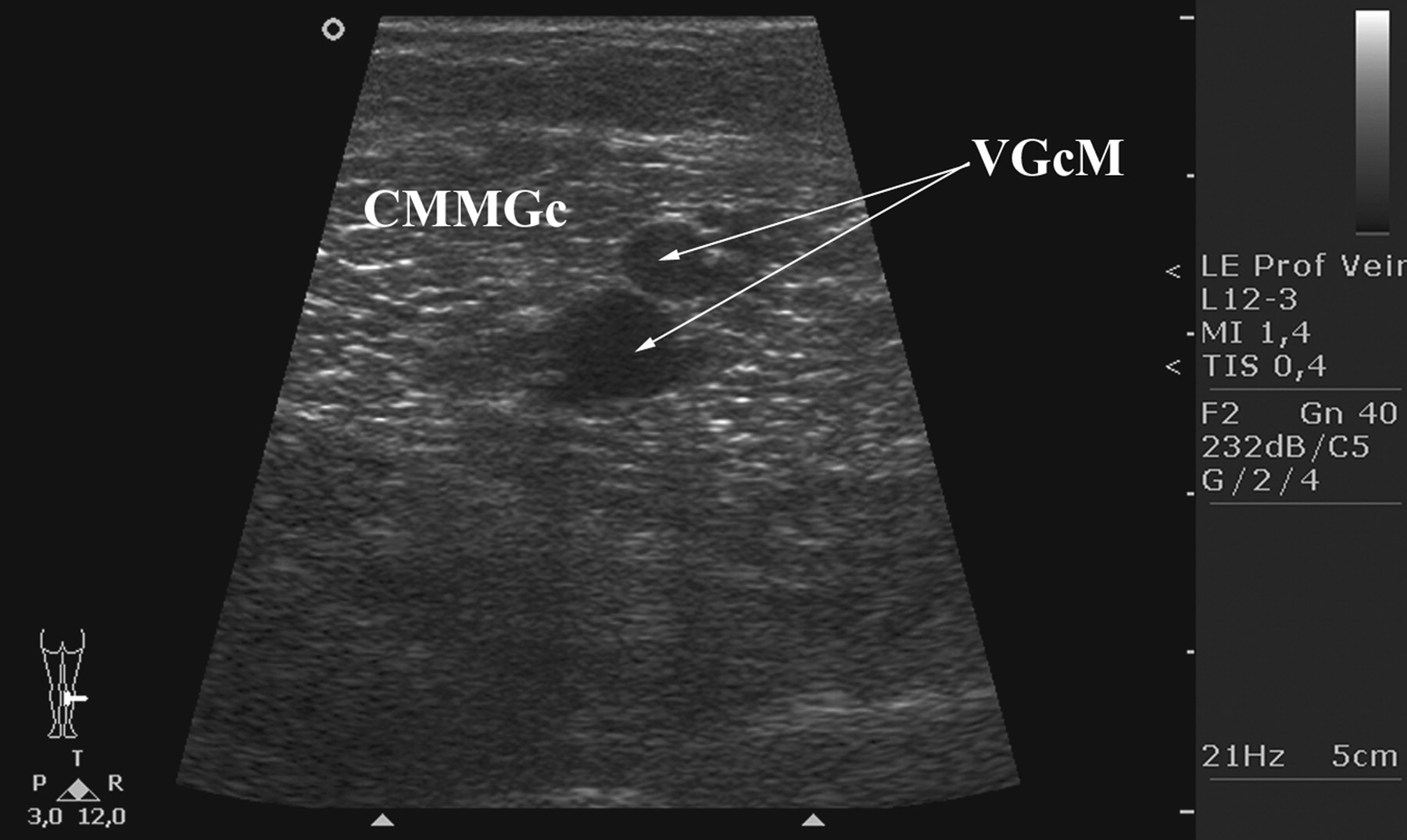
The ultrasound image of the veins of the gastrocnemius. CMMGc, caput mediale musculi gastrocnemii (musculi tricipitis surae); VGcM, vena gastrocnemia medialis
The musculus triceps surae contains within its muscular mass a system of large veins, frequently incorrectly denominated as the ‘muscular venous sinuses’, which serve as a principal source of the calf muscular pump. It is composed of 1–18 veins within the musculus soleus and a less important counterpart inside the musculus gastrocnemius. 20 From 25 years of age, the venous wall of this system slowly and successively degenerates and gets the sinuous or even varicose appearance. 21
Junctio saphenopoplitea (saphenopopliteal junction)
The estuary of the vena saphena parva into the vena poplitea is situated under the fascia poplitea, in the depth of the popliteal fossa, and the authors recommend that it should be referred to as the ostium saphenum (saphenous opening). The valvula terminalis is located 1–2 mm distally to the estuary. Another valve is usually found 3–5 cm distally to the vein estuary and is termed the valvula preterminalis (preterminal valve). 1 These two valves demarcate the segment of the vena saphena parva which forms, together with the adjacent segment of the vena poplitea, the junctio saphenopoplitea.
Plexus venosus genicularis (genicular venous plexus)
This term has replaced the denomination ‘venae geniculares’ (genicular veins), because the veins within the fossa poplitea collecting the venous blood from the knee region and knee joint do not correspond to the arteries which are six – unpaired arteria genus descendens (descending genicular artery) and arteria genus media (middle genicular artery) and paired arteriae genus superiores et inferiores (superior and inferior medial and lateral genicular artery) – but intermingle into a system of mutually interconnected vessels.
Vena femoralis (femoral vein)
This vein originates as the continuation of the vena poplitea at the hiatus adductorius, situated at the proximal end of the fossa poplitea between the insertions of the musculus adductor magnus and ascends through the canalis adductorius (adductor canal; ‘canalis vastoadductorius; canalis subsartorialis; canalis Hunteri; vastoadductor canal; subsartorial canal’) and enters the trigonum femorale (‘fossa Scarpae major’; femoral triangle) (Figure 7). The prevailingly used clinical term ‘vena femoralis superficialis’ (superficial femoral vein) should be omitted due to the fact that this vein belongs to the deep system of the lower extremity veins and this term is not included in the TA.
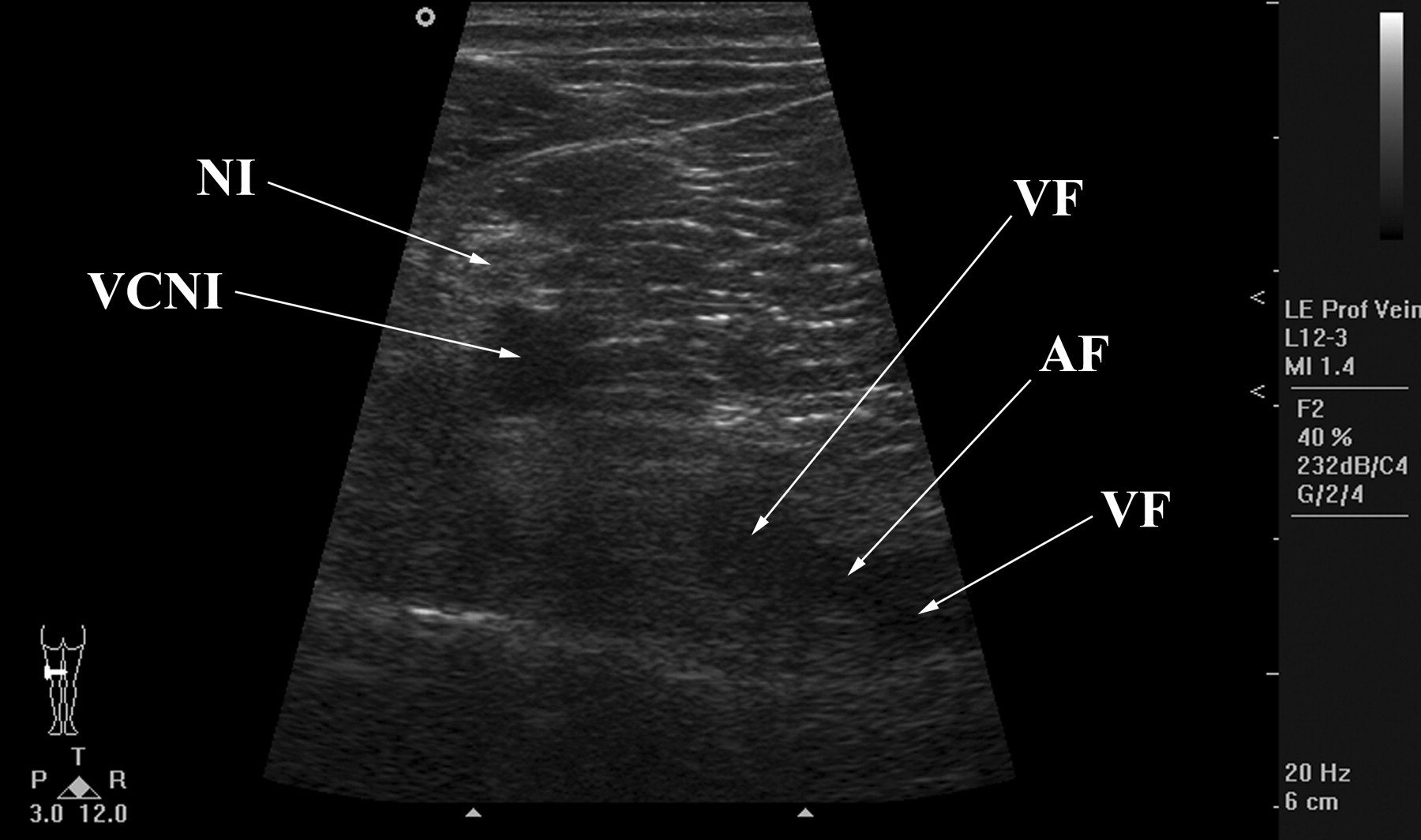
The transverse ultrasound image of the vena ischiadica. AF, arteria femoralis; NI, nervus ischiadicus; VCNI, vena comitans nervi ischiadici; VF, vena femoralis
The vena femoralis can be doubled in 6–46% of cases, rarely even tripled. The duplication can be isolated to the vena femoralis or combined with vena poplitea duplications. 18,19,22,23 The duplicated segment can be seen either superficial to the vena femoralis or adjacent to the arteria femoralis and superficial to the vein. 22
The anatomical variations of vena femoralis (as well as other large veins) can be considered venous malformations (designated as ‘minor truncular form’) in the new classification of congenital vascular malformations, as formulated by Lee. 24 For details of truncular variations and their embryological background see Uhl et al. 23
The vena femoralis usually contains 3–5 valves. The ‘valvula infrasaphenica’, located distally to the junctio saphenofemoralis and to the junction with the vena profunda femoris, is present in 100% of cases! 21
Confluens venosus subinguinalis (confluence of superficial inguinal veins)
This term is applied to a segment of the vena saphena magna close to the estuary of the vena saphena magna into the vena femoralis communis, including the centripetal segments of the venous tributaries (listed below), draining the thigh, the groin, the anterior and lateral abdominal wall and the external genital organs, as far as their terminal valves, including the venous plexus of the adjacent inguinal lymph node(s). 1
The confluence is situated at the level of the inguinal flexion line and receives the following tributaries:
Vena epigastrica superficialis (superficial epigastric vein);
Vena circumflexa ilium superficialis (superficial circumflex iliac vein);
Vena pudenda externa superficialis (superficial external pudendal vein);
Vena saphena magna accessoria anterior et posterior (anterior and posterior accessory great saphenous vein);
Vena circumflexa femoris anterior (anterior femoral circumflex vein).
These veins drain into the terminal arch of the vena saphena magna in 75% of cases; in the remaining cases they either join a common trunk or empty separately into the vena femoralis communis, confluens venosus subinguinalis or into the vena saphena magna accessoria.
1
Junctio saphenofemoralis (saphenofemoral junction)
There is an ambivalence in the application of this term. From the anatomical point of view, junctio saphenofemoralis is only the saphenous opening into the common femoral vein. But in 2005, the IIC suggested that the junctio saphenofemoralis should be reconsidered, from the anatomical-clinical point of view, as the complex of venous connections and valves in the vicinity of the saphenous opening. 9 It is applied to a segment of the vena saphena magna, which is delineated by two valves: proximally, close to the estuary of the vena saphena magna into the vena femoralis communis, there is the valvula terminalis (terminal valve, the last valve of the vena saphena magna); distally by the valvula preterminalis (preterminal valve), situated approximately 3–5 cm against the blood flow. Furthermore, this area is delineated by the valvula suprasaphenica (in the vena femoralis communis), located proximally to the ostium of the vena saphena magna, and the valvula infrasaphenica, located distally. 1
From the pathophysiological point of view, the valvulation of the confluens venosus subinguinalis and of the terminal arch of the vena saphena magna substantially influences the haemodynamics in both healthy and varicose limbs. As a consequence, in clinical anatomy, the two terms (confluens and junctio) are not to be considered as equipollent. 9 The authors recommend that the term ostium saphenum (saphenous opening) should be applied to the estuary of the vena saphena magna into the vena femoralis communis.
Vena profunda femoris (‘vena femoralis profunda’; profunda femoris vein; deep vein of thigh; ‘deep femoral vein’)
Thick short vein commences as a confluence of smaller muscular veins, collecting blood from posterior and medial group of thigh muscles and veins accompanying the arteriae perforantes (perforating arteries). Close before its estuary into the vena femoralis communis (common femoral vein) it contains a valve. Both the vein and its tributaries feature several valves. 25
The term ‘vena femoralis profunda’ (‘deep vein of thigh; deep femoral vein’), not listed in the TA, should be omitted due to the fact that it is a unspecific and misleading term, as recommended by FCAT. 6
Venae circumflexae femoris mediales et laterales (medial and lateral circumflex femoral veins)
The deep veins of the thigh collect blood from the thigh muscles and hip joint and empty into the vena femoralis or vena femoralis communis, rarely into the vena profunda femoris.
Venae comitantes arteriarum perforantium (‘venae perforantes’; deep femoral communicating veins; ‘perforating veins’)
(Caggiati stated the incorrect Latin term ‘venae comitantes arteriae perforantium’ in the consensus document). 9
These deep veins accompany the arteriae perforantes, which are branches from the arteria profunda femoris and pierce the adductor muscles to enter the posterior compartment of the thigh. The denomination ‘perforantes’ should be omitted because it is exclusively reserved in the field of the veins of extremities for the type of veins, connecting the superficial and deep venous systems (venae perforantes; perforators; perforating veins), while the aforementioned veins only accompany the corresponding arteries, i.e. they pierce the medial group of thigh muscle (adductors) dorso-ventrally but always keep the deep compartments and should be considered as a part of the deep venous system.
Vena femoralis communis (common femoral vein)
This large and short vein commences as the confluens of the vena femoralis and vena profunda femoris in the proximal part of the trigonum femorale (‘fossa Scarpae major’), approximately 1–3 cm distally to the branching point of the arteria femoralis. This confluens is situated 4–12 cm distally to the ligamentum inguinale (inguinal ligament, ‘ligament of Poupart’). 26,27 The vein runs within the fossa iliopectinea (iliopectineal fossa; ‘fossa Scarpae minor’) and changes its denomination into the vena iliaca externa when passing through the lacuna vasorum (lacunar space) under the ligamentum inguinale to leave the lower extremity and enter the pelvis. Its only valve (‘valvula suprasaphenica’), present in at least 76–81% of cases, 19,28 is located proximally to the ostium saphenum (saphenous opening), which protects the superficial venous system of the lower extremity against the elevated intra-abdominal pressure. 29
Vena comitans nervi ischiadici (vena comitans of sciatic nerve; ‘vena ischiadica’; ‘sciatic vein’)
The term vena ischiadica was omitted in the Terminologica Embryologica issued on-line in 2009. The principal trunk of the embryonic venous system (vena axialis membri inferioris; axial vein of lower limb) is situated in the dorsal part of the lower extremity and follows the course of the nervus ischiadicus (sciatic nerve) (Figures 7 and 8). Although its role of the main collecting venous trunk of the lower extremity is replaced by ventrally located vena femoralis, it need not perish and can serve as its important collateral. The beginning of the vena glutea inferior (inferior gluteal vein) corresponds to the part of the original vena comitans nervi ischiadici. This communication between the lower extremity and pelvis system veins can be of clinical importance. Especially in pregnancy, the venous valves become incompetent and this vein serves as a minor way to develop varices in the vulva, perineum and lower extremities. This point (designated as ‘G’) is defined as a site in the gluteal region in which the inconstant vena comitans nervi ischiadici, running on the posterior surface of the thigh from various level, joins the peripheral segment of the vena glutea inferior (before the latter enters the infrapiriform foramen). These leakage points are the clinical anatomical structure, not having the corresponding terms within the anatomical terminology. Nevertheless, they are of a great importance for the evaluation of the reflux. 2,31

The longitudinal ultrasound image of the vena comitans nervi ischiadici. NI, nervus ischiadicus; VCNI, vena comitans nervi ischiadici
Persistent vena comitans nervi ischiadici is often coincident with the Klippel–Trenaunay–Weber syndrome (varicose veins, skin haemangiomas and hypertrophy of soft tissue and bones) – approximately in 50% of cases.
12,32
It is a rare variation, first described by Servell in 1978 and classified into three types by Cherry:
33,34
Vena comitans nervi ischiadici persistens (persistent sciatic vein) originates in the area of the vena poplitea, ascends along the whole posterior aspect of the thigh, enters the lesser pelvis via the foramen infrapiriforme (infrapiriform foramen), together with the nervus ischiadicus and terminates into the vena iliaca interna;
Vena comitans nervi ischiadici persistens femoris superior (superior femoral persistent sciatic vein) commences in the proximal posterior aspect of the thigh and continues into the lesser pelvis;
Vena comitans nervi ischiadici persistens femoris inferior (inferior femoral persistent sciatic vein) is present in the distal and middle part of the posterior aspect of the thigh and empties into the vena profunda femoris.
Vena obturatoria (obturator vein)
The parietal tributary of the vena iliaca interna (internal iliac vein) originates within the proximal portion of the medial group of thigh muscles, enters the lesser pelvis through the canalis obturatorius (obturator canal), together with the corresponding artery and nerve, and runs dorsocranially, along the lateral wall of the pelvis, covered by the artery. In some cases, it may be completed or even replaced with a widened vena pubica (pubic vein), which conveys blood into the vena iliaca externa. Then it is termed the vena obturatoria accessoria/aberrans (accessory/aberrant obturator vein). It has important communications in the proximal part of the thigh with the venae circumflexae femoris. 2
Abbreviations
The frequent long terms of the veins are replaced with abbreviations mainly in the communications among clinicians. Unfortunately, there is no unified system or rule for their usage either worldwide or nationally and the superfluous number of synonyms can give rise to communication errors and misunderstandings. That is why the derivation of abbreviations from the Latin nomenclature, which is the only official and worldwide-accepted one, seems to be the correct way. Nevertheless, the list of equivalent English abbreviations is stated as well (Table 3).
The most applied recommended abbreviations (derived from Latin)
*It is recommended not to use the term ‘deep femoral vein, deep vein of thigh’
†Due to the duplicity, it is recommended to omit the abbreviation VPe (PV), derived from the term vena peronea
Conclusion
Exact and clear anatomical nomenclature is necessary for easy and safe communication in angiology and phlebology. Internationally accepted norms are the easiest and most acceptable way for understanding among specialists speaking different languages.
Footnotes
Acknowledgement
Special thanks to Mirka Plecitá for the bibliographic support and to Štěpán Hájek for illustrations.