
Abstract
Background
Venous valves have been classified into parietal (PVs) and ostial valves (OVs). PVs are located within the lumen of veins, whereas the OVs are located directly at the confluence of two veins. In the common femoral vein (CFV), the most prominent PVs are the suprasaphenic and infrasaphenic valve. The terminal valve (often designated as ‘valvule ostiale’ in the relevant literature in French) defined as that lying between the orifice of the great saphenous vein (GSV) and the most proximal of the major superficial tributary veins and the preterminal valve represent the most important PVs in the GSV. While PVs are well studied, there is not much literature on the OVs of the superficial venous system, especially of the GSV.
Objective
In order to investigate the presence of OVs (defined strictly as valves located at the entrance of a tributary vein) in the GSV, we carried out studies on specimens obtained from bodies bequested to the Division of Clinical and Functional Anatomy of Innsbruck Medical University.
Methods
Ninety-eight specimens consisting of the CFV and the attached tributary veins including the GSV were investigated.
Results
In five of these (5.1%), a single-cusped OV, in six (6.1%) a two-cusped OV and in 10 (10.2%) remnants of an OV were identified. Thus, OVs do not seem to be primarily present in all GSVs.
Conclusion
The distinction between PVs and OVs is not always clear in literature, and as a consequence misinterpretations may occur. Very often the terminal valve of the GSV, which is in fact a PV, is designated as an ‘ostial valve’. In view of its widespread use, we suggest that the term ‘ostial valve’ together with its clear description be included in the consensus documents of the ‘Union Internationale de Phlébologie’.
Introduction
Knowledge about venous valves has evolved over centuries, beginning in the 16th century when Fabricius ab Aquapendente gave a detailed description of these membranous entities in the veins. Other illustrious names in this field dating back to the 16th century are Charles Estienne, Giovanni Battista Canano and Ludovicius Vassaeus. 1–8
Venous valves have been classified into parietal (PVs) and ostial valves (OVs). 9,10 According to Franklin, 10 the OVs, which are located at the point of entry of tributary veins, have been variously designated as ‘platismata’ or ‘platismatia’, ‘soupapes’, ‘valvules en toupie’ or ‘Astklappen’. A literature search using the keywords ‘platismata’, ‘platismatia’, ‘soupapes’ or ‘valvules en toupie’ did not lead to articles on venous valves besides some biological and technical papers; use of the keyword ‘Astklappen’ yielded some relevant references. 11–17 Fish are reported to be completely lacking in PVs, but richly endowed with OVs. 18 In humans, OVs occur less frequently and usually consist of a single cusp, sometimes of two cusps. 10 In the case of a single-cusp OV, the free margin typically looks towards the heart and the distal margin forms the attached agger, the thickened attachment of the valve's framework to the venous wall. 10 The concave area faces obliquely towards the cavity of the tributary and the convex in the opposite direction. 9 OVs are located at the entrance of a tributary vein, but they are attached to the wall of the major vein into which the tributary vein drains. Citing Sappey, 19 Franklin 10 wrote, ‘A valve which is not inserted into the circumference of the actual entry is not an ostial, but a parietal valve, no matter how near it is to the entry.’ The function of venous valves, primarily discovered by Harvey, 20 is characteristically viewed as a mechanism to guide direction of the blood flow and to prevent reflux by undergoing four phases (opening phase, equilibrium phase, closing phase and closed phase). 9,21,22
OVs direct the blood stream from the tributary into the main vein. The arrangement of the valvular apparatus of a single-cusp OV is such that when the blood within the common femoral vein (CFV) flows backwards upon the concave surface of the valve, it presses the cusp more or less across the cross-section, that is, the lumen of the CFV, and away from the orifice of the great saphenous vein (GSV [Figure 1a]). A single-cusped OV offers the GSV no protection from reflux. The main function of such a single-cusped OV appears to be to prevent blood pumped from the GSV into the CFV from passing into that portion of the CFV which is distal to the orifice of the GSV. The valve therefore directs the blood from GSV into the onward track of the CFV and prevents reflux of blood within the CFV. 9 Furthermore, a single-cusped valve divides the blood streams in the proximal portion of the CFV. As the velocity of the two streams is not necessarily the same, this would allow for two independent laminar flows running at different paces without too much turbulence. As has been shown previously, the motion of valvular cusps is driven mainly by the hydrodynamic pressure created by the flowing blood 21,22 ; this would mean that a high velocity inside the CFV would be able to drag open such an OV.
The function is quite different when an OV consists of two cusps, one at the proximal and another at the distal margin of the orifice. In these cases, the two cusps mutually assist each other, preventing blood from passing behind either. The result is a complete obstruction to all retrograde circulation into the smaller vessel (Figure 1c). 9
The anatomic–clinical concept of the saphenofemoral junction includes the valves proximal and distal to the orifice of the GSV, the suprasaphenic and the infrasaphenic valves of the CFV, as well as the proximal segment of the GSV with its terminal and preterminal valve. 23–28 All these mentioned valves are in fact PVs according to the description of Franklin, 10 and while these PVs are well studied, there is almost no literature on OVs of the GSV. 26,29–31 It was therefore the aim of our study to investigate whether there are OVs, defined strictly as valves located at the entrance of a tributary vein, but attached to the wall of the major vein into which the tributary vein drains, at the orifice of the GSV, and if they are detected, to distinguish them clearly from the terminal valve of the GSV.
Materials and methods
Between December 2008 and February 2009, 98 specimens consisting of the CFV and the attached tributary veins including the GSV were investigated for the presence of OVs at the orifice of the GSV. The specimens had previously been used for investigating the exact position of valves at the saphenofemoral junction. 28,32 All specimens were derived from bodies donated after premortal informed consent by the donors themselves to the Division of Clinical and Functional Anatomy of Innsbruck Medical University. 33 The adjacent parts of the CFV and the GSV were opened longitudinally towards the conjunction of both trunks so as to expose the entrance of the GSV to the CFV. The lumina of the veins were cleaned with diluted formaldehyde, and thrombi, when present, were removed carefully. In our study, we used the definition of Franklin and Salter that a valve which is not inserted into the circumference of the actual entry is not an OV, but a PV. 9,10 Each specimen was documented photographically with a Nikon D100 (Nikon Corporation, Tokyo, Japan) using a distinct protocol.
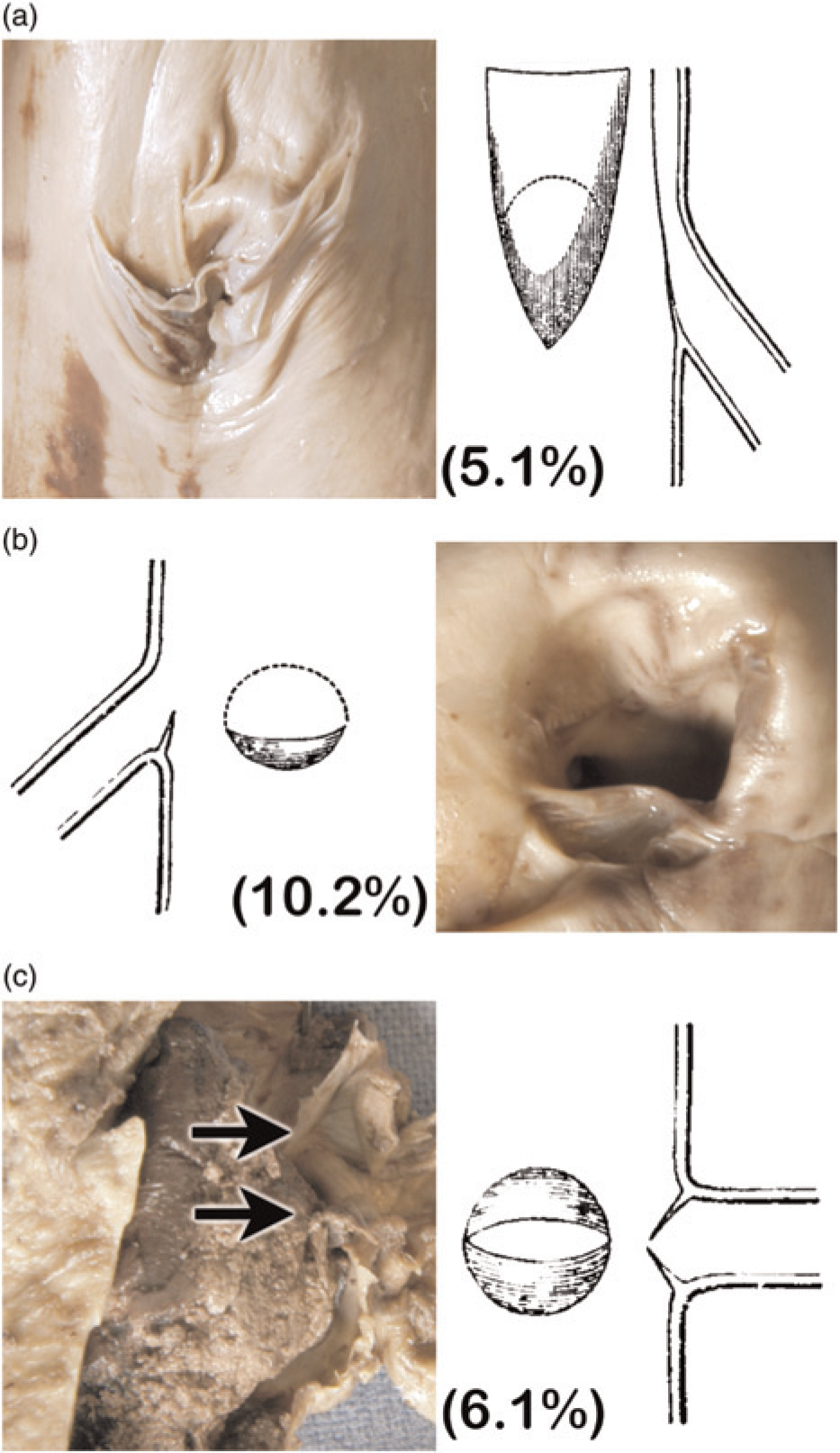
Sample specimens and schematic representation of different forms of ostial valves (OVs): (a) a single-cusped OV, (b) incomplete single-cusped OV and (c) a double-cusped OV (the arrows point to the two cusps). The schematic drawings were taken from Salter, Figure 683 9
Results
An OV consisting of a single cusp (5.1%) (Figure 1a) was present in five of the 98 investigated specimens, an OV with two cusps was present in six of the specimens (6.1%) (Figure 1c) and 10 specimens showed remnants of an OV (10.2%) (Figure 1b). In all single-cusped OVs, the distal margin was attached to the wall of the CFV at the margin of the GSV's orifice and the cusp with its proximal free border covered the entry of the GSV. The concave area of the valvular apparatus constantly faced towards the saphenous trunk. We only considered those valves as OVs in which the attached agger was strictly inserted into the circumference of the entry of the GSV exactly where the trunks join with cusps flattening over the orifice of the GSV. All other detected valves, no matter how near they were to the entry, were excluded and were considered as PVs.
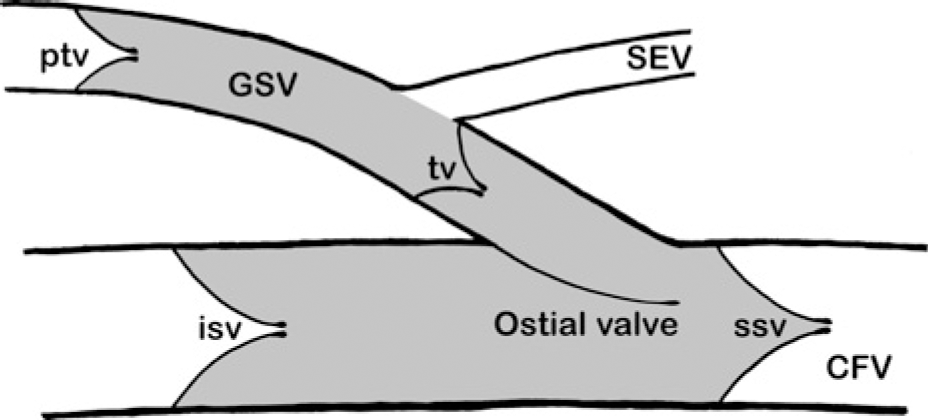
Scheme of the saphenofemoral junction with a single-cusped ostial valve (sagittal plane). CFV, common femoral vein; GSV, great saphenous vein; SEV, superficial epigastric vein; tv, terminal valve; ptv, preterminal valve; ssv, suprasaphenic valve; isv, infrasaphenic valve
Discussion
OVs are described at various positions: the Thebesian valve at the orifice of the coronary sinus, 34 the Eustachian valve as the OV of the inferior vena cava, 10 the valve of Vieussens at the orifice of the great cardiac vein at its junction with the oblique cardiac vein, 34,35 valves over the entrance of tributary veins into the mesenteric veins, 36 those guarding the renal entry in the inferior vena cava, 37 OVs at the orifices of spermatic and ovarian veins, 38 valves over the entrance of the vertebral, inferior thyroid and superior phrenic veins, 10 OVs at the orifice of an intercostal vein joining the azygos vein, 9 a valve at the orifice of a hepatic vein where it joins the vena cava 9 and valves at the junction of the vena azygos with the vena cava 2 as well as OVs in the deep veins of the lower limb. 39 This listing shows clearly that OVs are found repeatedly; nevertheless, all of them have been described within the deep venous system, whereas there is no description in the literature found of OVs in the superficial venous system. In particular, the OV of the GSV may have clinical significance in retrograde blood flow in the lower limb (Figure 2). 24 Thus, a competent OV, especially if double-cusped, can offer protection from pathological vein reflux from the CFV. Hence, it is important to identify OVs in the GSV and differentiate saphenous from non-saphenous trunk pathology before surgical interventions are carried out with the aim of preserving the main GSV for its potential use in coronary bypass grafting and other vascular procedures.
However, the distinction between PVs and OVs is not always clearly drawn in literature. The terminal valve of the GSV, in particular, which is in fact a PV, is often designated as ‘ostial valve’ or ‘valvule ostiale’, mainly in French studies. 29–31 Furthermore, OVs can also be identified in sonography, sometimes mimicking a terminal valve situated immediately at the orifice (compare for instance Figure 7.7a in Mendoza's 40 book, which according to us depicts an OV, and not a terminal valve). This may result in misapprehension of an author's meaning as well as misinterpretation of sonographic findings. We would like to emphasize that anatomic terms should be clearly defined and strictly adhered to for the sake of clarity in theory and clinical practice. Thus, according to the strict definitions used in this study, the terminal valve can never be an OV; it is clearly a PV, irrespective of how close it is to the saphenofemoral junction. We suggest that the term ‘ostial valve’ together with its proper description be included in the consensus documents of the ‘Union Internationale de Phlébologie’, with the additional comment that it can never stand for the terminal valve of the great saphenous vein. 26,41
Footnotes
Acknowledgements
We thank Rajam Csordas-Iyer for critical reading and editorial assistance.