
Abstract
Isolated popliteal venous entrapment is unusual and often caused by variation or aberrant origins of the gastrocnemius muscle, thickened perivenous fascia or an abnormal vascular bundle. We report a unique case of a fit and well 35-year-old man with popliteal venous entrapment after presenting to the vascular unit with symptomatic varicose veins. The cause of the entrapment was found to be an aberrant medial sural artery on operative exploration. The artery was ligated, releasing the entrapped vein. The patient made an uneventful recovery with resolution of symptoms of venous insufficiency without evidence of muscle ischaemia.
Introduction
Popliteal venous entrapment is often associated with entrapment of the popliteal artery. Isolated popliteal venous entrapment is less common. Potential causes include variation in the origin of the medial or lateral head of the gastrocnemius muscle, 1 vascular anatomic course anomalies, 1,2 a fibrous band 2 or thickened perivenous fascia. 1 Popliteal venous entrapment is often asyptomatic but is a potential cause of chronic venous insufficiency in the affected limb. 1 We report a unique case of symptomatic popliteal venous entrapment caused by an aberrant medial sural artery.
Case report
A healthy 35-year-old man was referred from his primary care provider with symptomatic right lower limb varicosities in the long saphenous distribution with a palpable mass in the right popliteal fossa (Figure 1). There was no history of deep vein thrombosis, pulmonary embolism or long bone fracture. Duplex sonography of the affected limb demonstrated a popliteal venous aneurysm in addition to a dilated great saphenous vein secondary to incompetence at the saphenofemoral junction; the short saphenous system was competent. A magnetic resonance venogram suggested the aneurysm to be a poststenotic venous dilation of unclear cause (Figure 2); there was no evidence of muscular compression. Colour duplex sonography excluded a concomitant popliteal artery entrapment. Dorsal venous arch pressure measurement revealed maximal venous pressures on forced ankle dorsiflexion which exceeded systolic arterial pressures (240 mmHg).

Preoperative clinical images demonstrate significant varicosities in the great saphenous distribution of the right calf: (a) medial view, (b) anterior view
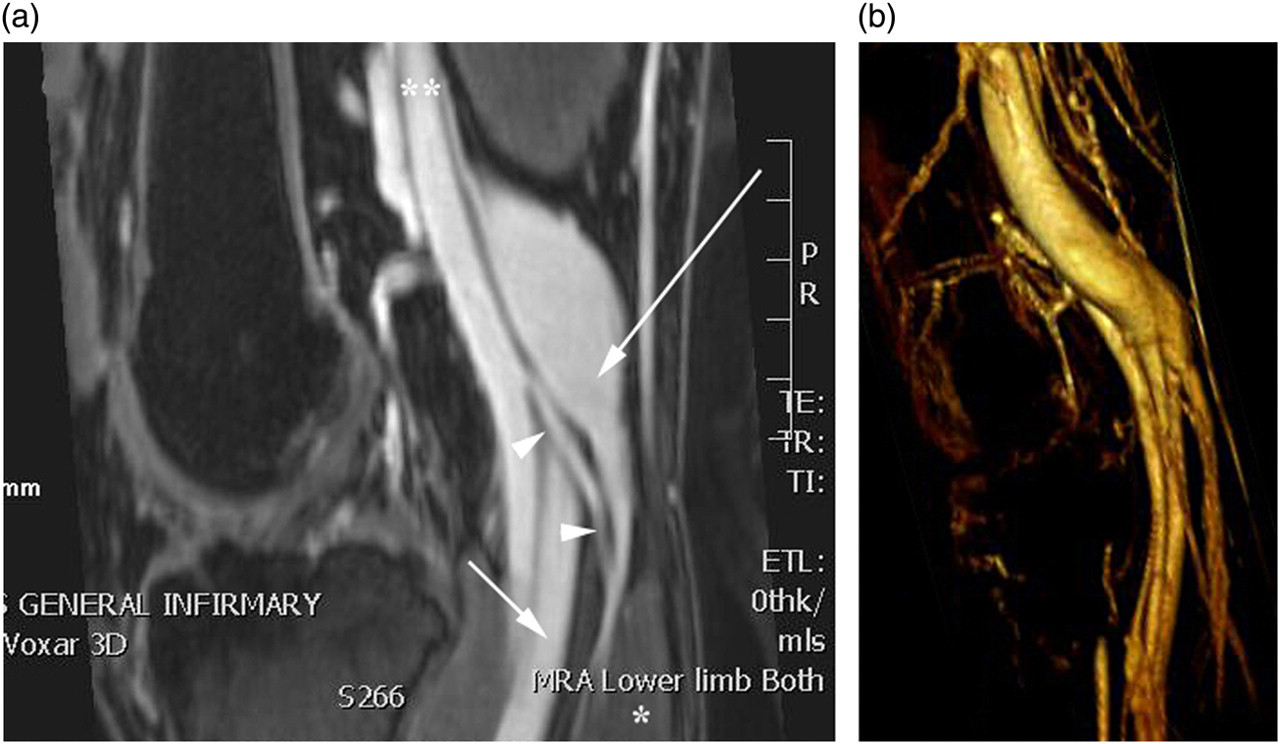
(a) Magnetic resonance venogram demonstrated a poststenotic dilation in the posterior tibial vein (long arrow) at the level of the tibio-peroneal trunk (short arrow) and abberantly placed medial sural artery (arrowheads) can be seen originating from the popliteal artery (**), coursing across the posterior tibial vein towards the medial head of gastrocnemius (*). (b) A three-dimensional reconstruction demonstrates the anatomy more clearly
Surgical exploration of the right popliteal fossa via a standard posterior approach revealed the source of venous entrapment to be a high branching medial sural artery. The small 2 mm diameter artery arose directly from the popliteal artery and emerged between the convergence of the posterior tibial vein and tibio-peroneal trunk before coursing around the neck of the posterior tibial vein to supply the medial head of gastrocnemius (Figure 3) which was itself in the standard position. The obliquely coursing medial sural artery was splinted between the posterior tibial vein and the tibio-peroneal trunk causing entrapment of posterior tibial vein which was most marked on forced ankle dorsiflexion. The aberrant artery was tied and ligated under tourniquet control to reduce the risk of excessive bleeding from the large venous aneurysm, releasing the tension on the posterior tibial vein. The patient made an uneventful recovery and was discharged on the same day. He was symptom free at one month follow-up.
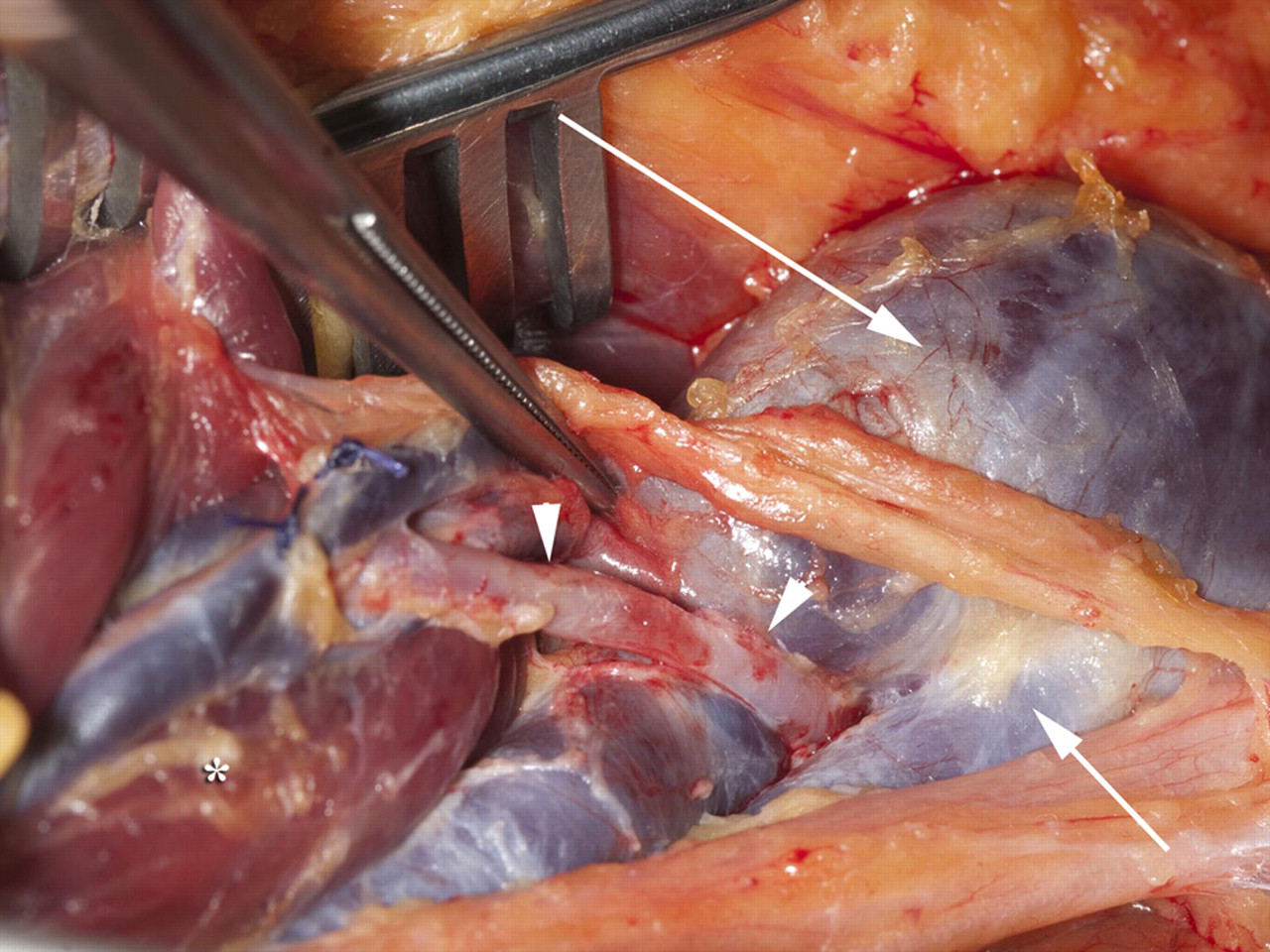
Operative exploration of the right popliteal fossa revealed abberant medial sural artery (arrowheads) emerging as the level of the tibio-peroneal trunk (short arrow) impinging on the posterior tibial vein causing poststenotic dilation (long arrow) before supplying the medial head of gastrocnemius (*)
Discussion
Isolated popliteal vein entrapment is uncommon when compared with popliteal artery entrapment. 1,2 To our knowledge this is the first documented case of an aberrant medial sural artery causing popliteal vein entrapment. The venous network within the popliteal fossa can be highly variable and the sural arteries can overlie popliteal vein tributaries in normal anatomy. 3 The primitive popliteal artery develops as a fusion of the fetal axial artery proximally and the fetal sciatic artery distally during embryological weeks 6–10. This development coincides with the migration of the medial head of the gastrocnemius muscle from the lateral epicondyle of the femur across the popliteal fossa to the proximal aspect of the medial femoral condyle before the distal third of the popliteal artery has fully formed. 4 The medial head of gastrocnemius carries its blood supply, via the medial sural artery, with it during this proximal migration. In this case, we observed higher branching of the medial sural artery than that typically described. We hypothesize that consequent development of the popliteal venous tributaries produced a sling, proximal to the medial sural artery between the posterior tibial vein and tibio-peroneal trunk. This venous sling limited subsequent cranial migration of the medial sural artery with the medial head of gastrocnemius and is likely to have resulted in the observed entrapment of the posterior tibial vein. We observed no clinical evidence of medial gastrocnemius muscle ischaemia following ligation of the culprit medial sural artery which we relate to collateral supply via the lateral sural artery. 5
In summary, we report the first case in the literature of popliteal venous entrapment secondary to an aberrant medial sural artery in a patient with symptomatic great saphenous distribution varicosities. Division of the medial sural artery to relieve entrapment is safe due to the dense anastomotic supply to the gastrocnemius mucle.
Footnotes
Acknowledgement
The authors confirm that this work is their own and that there has been no duplicate publication. Patient consent to publish this work has been obtained. No funding was received to undertake this work. There are no conflicts of interest.