
Abstract
In the recent past, eight cases of transient ischaemic attack or cerebral vascular accident related to foam sclerotherapy have been reported. The following case is reported to add to the world clinical experience and raises the concern that foam sclerotherapy should continue to be evaluated and reported rigorously to establish the incidence of potentially devastating complications. While waiting for clinical studies to further establish best practice in this area of treatment, it may be in our patients’ best interests to reserve the option of foaming sclerosants for selected rather than routine cases of venous insufficiency.
Keywords
Introduction
This report describes what is likely the ninth documented cerebral vascular event associated with the treatment of varicose veins with foam sclerotherapy injection. This case demonstrates evidence of an air embolism in the middle cerebral artery in a patient without atrial septal wall defect. The purpose of this report is to heighten awareness of potential adverse outcomes related to foam sclerotherapy when performed within the current standards of care following the European Consensus Meeting Guidelines. 1
Case report
In May 2007, a 36-year-old healthy woman was evaluated and was noted to have insufficiency in her left great saphenous vein (GSV) with mild deep system reflux. She was treated conservatively for one month, during which she sought a second opinion with one of the authors. It was noted that she had experienced leg swelling and spontaneous leg cramps since her pregnancies in 2005 and 2006. She had been using compression hosiery and elevation for relief of her symptoms. Her medical history was significant for seasonal allergies controlled with cetirizine. Her only other medication was a daily vitamin. She denied tobacco or alcohol use.
On initial examination she was 5 foot 10 inchestall, and weighed 185 pounds. Her heart rate was 64 beats per minute with a blood pressure of 110/64 millimetres of mercury. In general, she had a normal physical exam with lower extremities revealing mild swelling bilaterally; multiple large varicosities were evident in the region of the anterior accessory distribution of the GSVs bilaterally with an ultrasound-based CEAP (clinical, aetiological, anatomical and pathological elements) classification of C3s0EpAs2,3,4 p17Pr. During preoperative mapping, duplex imaging revealed reflux in the bilateral GSVs with a diameter of 11 mm at the saphenofemoral junction (SFJ) on the right and 7 mm at the SFJ on the left. Reflux was also noted in the right small saphenous vein (SSV) with a diameter of 5 mm and in a distal thigh perforator with a diameter of 4 mm.
The patient returned to the office for staged treatments consisting of endovenous laser therapy (EVLT®) to her right GSV with microphlebectomy to her anterior thigh, EVLT® and microphlebectomy of her left GSV and tributaries and EVLT® of the right SSV. The procedures were well tolerated and she had uneventful follow-up when ultrasound showed treated veins that were incompressible without flow. Approximately two months following completion of the endovenous ablation and microphlebectomy treatments, the patient returned for sclerotherapy. She had a bilateral treatment for residual varicose and reticular veins using sodium tetradecol sulphate (manufactured by Bioniche Teo, Inverin Co. Galway, Ireland) 0.3% and 0.5%. A total of 5 mL of sclerosant was injected.
The patient returned one month later for a second treatment. At this appointment a total of 3 mL was injected. Two millilitres of 0.5% sodium tetradecol sulphate foamed (via the Tessari method with 4 mL of air to 1 mL of solution) were injected in addition to 1 mL of 0.3% liquid. She was treated while in a mild Trendelenberg position and additional cutaneous spider veins were ablated with a surface 940 nm laser.
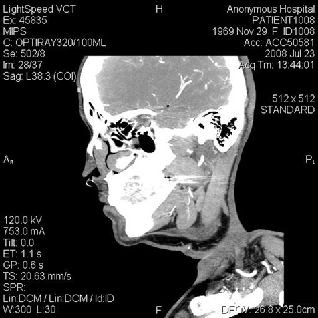
Initially, the patient tolerated the procedure well. However, while she was getting dressed she collapsed (unwitnessed) and was found conscious on the floor by a medical assistant less than five minutes after the physician had left the room. Her initial blood pressure was 120/80 with a heart rate of 70 and an oxygen saturation of 96% on room air. She was noted to have slurred speech, and though her pupils were equal and reactive, she was found to have a dense right hemiplegia. A survey physical exam demonstrated a regular heart rate without murmur, even and clear respirations, and equal palpable pulses. The emergency medical service was called and the patient was transported to the local medical centre emergency department (ED). In the ED her National Institute of Health stroke scale rating was 11. An urgent computed tomography scan (CT scan) of the brain demonstrated an air embolus in the left middle cerebral artery (MCA) with early ischaemic changes in at least a third of the MCA territory (see Figures 1–3). The CT scan also showed a cut-off of the proximal left MCA due to air bubbles. Some resolution of the patient's symptoms was noted within two-and-a-half hours from their onset, and within three hours from the onset of symptoms she had a normal neurological exam. Her initial lab panels including a complete blood count, comprehensive medical panel, prothrombin time, international normalized ratio, and creatinine kinase MB, were all within normal limits, as was her electrocardiogram.
Three views clearly demonstrating air embolism in left middle cerebral artery. Axial view of brain showing air embolism in left middle cerebral artery Three views clearly demonstrating air embolism in left middle cerebral artery. Sagittal veiw of brain showing air in left middle cerebral artery Three views clearly demonstrating air embolism in left middle cerebral artery. Coronal view of brain showing air in left middle cerebral artery

Despite the resolution of symptoms, the patient was then transported in a Trendelenburg position with high-flow oxygen to Massachusetts General Hospital's Acute Stroke Service. There she received hyperbaric oxygen therapy and intravenous heparin.
Approximately two days after her air embolism the patient had a transthoracic echocardiogram that suggested a possible intrapulmonary shunt. However, at the time of a subsequent transesophageal echocardiogram two months later no evidence of patent foramen ovale or intra-atrial shunt was noted.
Discussion
In 2006, an adverse neurological outcome was reported in Dublin, Ireland. This case reported a 61-year-old man who received 20 mL of 0.5% foamed polidocanol. 2 Volume was thought to have contributed to this outcome; therefore, smaller dosages were recommended for future treatments. The next two cases were reported in August of 2008: the first was a 72-year-old woman who underwent foam sclerotherapy after endovenous laser ablation and microphlebectomy. 3 She had two residual calf perforators. Each perforator received 2 mL of 2% Sotradecol foam, resulting in symptoms consistent with a transient ischaemic (TIA) attack. This information was reported in the same article as a 35-year-old woman who had 10 mL of foamed sclerosant injected into the reticular veins. Unfortunately, this woman fell and struck her head after the procedure, resulting in a more complicated neurological picture, including a new onset of seizure activity. She was documented to have suffered an air embolism in her vertebral artery. In 2009, a large study in France reviewed 1025 patients at 20 clinics who received foam sclerotherapy treatments. 4 These data included one case of TIA that fully resolved in 30 minutes. 4 A fifth case was reported in July of 2009, in which a 33-year-old man was reported to have suffered a right cerebellar infarct four days after receiving 4 mL of foamed 0.5% polidocanol. 5 Also in 2010, a sixth case was reported with a delayed neurological event, occurring in a 48-year-old woman four days after having sclerotherapy. 6 There are two more cases of similar events not described in this report, but referenced in French and German, making this the ninth case ever, but the seventh in the last five years.7,8
Of note, there was a case report in 1994 of a 41-year-old woman with a neurological event in the Netherlands after she was injected with 2 mL of 3% and 1 mL of 1% liquid polidocanol. 9 She experienced a warm sensation in her abdomen, followed by a bad taste in her mouth, paraesthesia in the right side of her body, and right upper visual field changes. This lasted for two days then fully resolved. Also, in 2004, a case of an ischaemic stroke was reported after liquid sclerotherapy in a 51-year-old woman who had two separate polidocanol injection sessions prior to the stroke. The injections given were 0.5 mL of 1%, 18 days prior to the event, followed by 0.5 mL of 0.5% three days prior to the event. The patient suffered mild aphasia and right brachiofacial hemiparesis. 10 Since these two cases were with liquid sclerosant, they will not be counted in the foam-related cases.
Ultrasound-guided foam sclerotherapy was revolutionized in 1995 after being coined ‘microfoam’ and being injected under ultrasound guidance by Cabrera et al. 11 Although performed with increased frequency since its inception, there is no clear safety profile for this treatment modality, which is currently not accepted by the Food and Drug Administration. Review articles suggest safety but state that more research must be done. 12 As this is the ninth documented adverse neurological event with symptoms worse than migraine/visual change, foam sclerotherapy may have more risks than previously thought. Informed consent should include possible TIA or cerebrovascular attack (CVA) with a potential incidence as high as one in every 1025 people. 4 It is important to recognize that there is published research on foam sclerotherapy involving 3259 consecutive patients, none of whom suffered from CVA or TIA 13 – making a lower incidence more likely unless there is underreporting of such cases as reported herein. With the understanding of the potentially serious complications associated with treatment, all offices using foamed sclerosants should be equipped with the ability to administer oxygen therapy and have an emergency system in place for transport to an ED for further evaluation and treatment. Access to hyperbaric oxygen therapy may also be considered in emergency planning.
Summary
Although risks are associated with all medical procedures, the risk benefit ratio must be kept in balance as the field of phlebology advances. Perhaps foam sclerotherapy should be reserved for cases of severe disease, and the patient should be told of the possibility of CVA/TIA as part of their informed consent. Physicians who perform foam sclerotherapy should have a plan in the event of post-treatment neurological deficits, including transport to hospitals or facilities equipped to manage CVA/TIAs. Liquid sclerosants offer an excellent alternative to foam for vessels less than 0.5 cm. Clinical trials and organized reporting of complications, possibly in the form of a registry, with respect to the use of foamed sclerosants, may help establish a more accurate incidence of this type of serious adverse event after what is becoming common practice in the treatment of chronic venous disease. It is likely that this is an underreported complication. This case has been briefly described in two other journal publications.14,15