
Abstract
The objective of this study is to report an overlooked cause of cervical swelling linked to a thoracic duct (TD) intraluminal obstruction. Four consecutive patients underwent supraclavicular fossa echo-colour-Doppler assessment (ECD) because of recurrent spontaneous cervical swelling. In all patients, during the swelling period we documented a TD dilation with hyperechogenic content, resulting undetectable during asymptomatic periods; ECD also allowed an effective differential diagnosis with TD cysts, obstructive malignancy or other causes of cervical swelling. In conclusion, ECD is to be considered an effective tool in cervical swelling and TD anomalies investigation.
Introduction
A recurrent cervical swelling, related to a spontaneous outlet obstruction of the thoracic duct (SOOTD), has rarely been reported. 1,2
The purpose of the study is to report echo-colour Doppler (ECD) effectiveness in detecting this unusual pathological condition.
Clinical series
Four patients, affected by SOOTD, underwent ECD by means of microconvex and linear high-frequency probes (8–13 MHz, Esaote Biomedica MyLabVinco Genoa, Italy).
The scanning began with a B-mode for thoracic duct (TD) detection, followed by a duplex and triplex assessment aimed to differentiate the TD (no blood flow signal) from other vessels.
Case 1 (the idiopathic recurrent SOOTD)
A 55-year-old woman was referred for a recurrent left supraclavicular swelling. A prior ECD had shown a ‘microcystic’ supraclavicular dilation – this pathological finding was not detected at our first assessment, which was performed following a not explainable swelling disappearance.
After a couple of weeks, such neck bulge spontaneously reappeared and the related ECD highlighted a dilated not compressible cervical TD (7 mm diameter; normal TD diameter reported in literature ranges from 1 to 4 mm). 3 One week later, the swelling and the ECD abnormal findings disappeared again, without any treatment.
Case 2 (the SOOTD treated by US-compression)
A 44-year-old woman was referred for a left supraclavicular swelling. ECD showed a dilated and obstructed thoracic duct (8 mm). Thoraco-abdominal computed tomography (CT) scan depicted a retroperitoneal effusion.
The patient was treated by fat-free diet and medium-chain triglycerides: clinical symptoms disappeared for some weeks, until she underwent another ECD because of a cervical swelling recurrence.
The examination found a dilated cervical TD. The obstruction did not seem to be complete since a slight echo-signals movement was seen in B-mode at the TD outlet. In order to force the TD flow, a tough compression was applied.
Surprisingly, a flush was seen rushing through the TD confluence into the subclavian vein while the TD emptied in a few seconds, even when the compression was stopped. After that, TD completely collapsed and became no longer visible.
Case 3 (the SOOTD with a TD confluence plug)
A 35-year-old woman was referred for a persistent swelling of the left supraclavicular fossa after many episodes of transient recovery.
Terminal TD obstruction and dilation (9 mm) was diagnosed by means of ECD (Figure 1a).
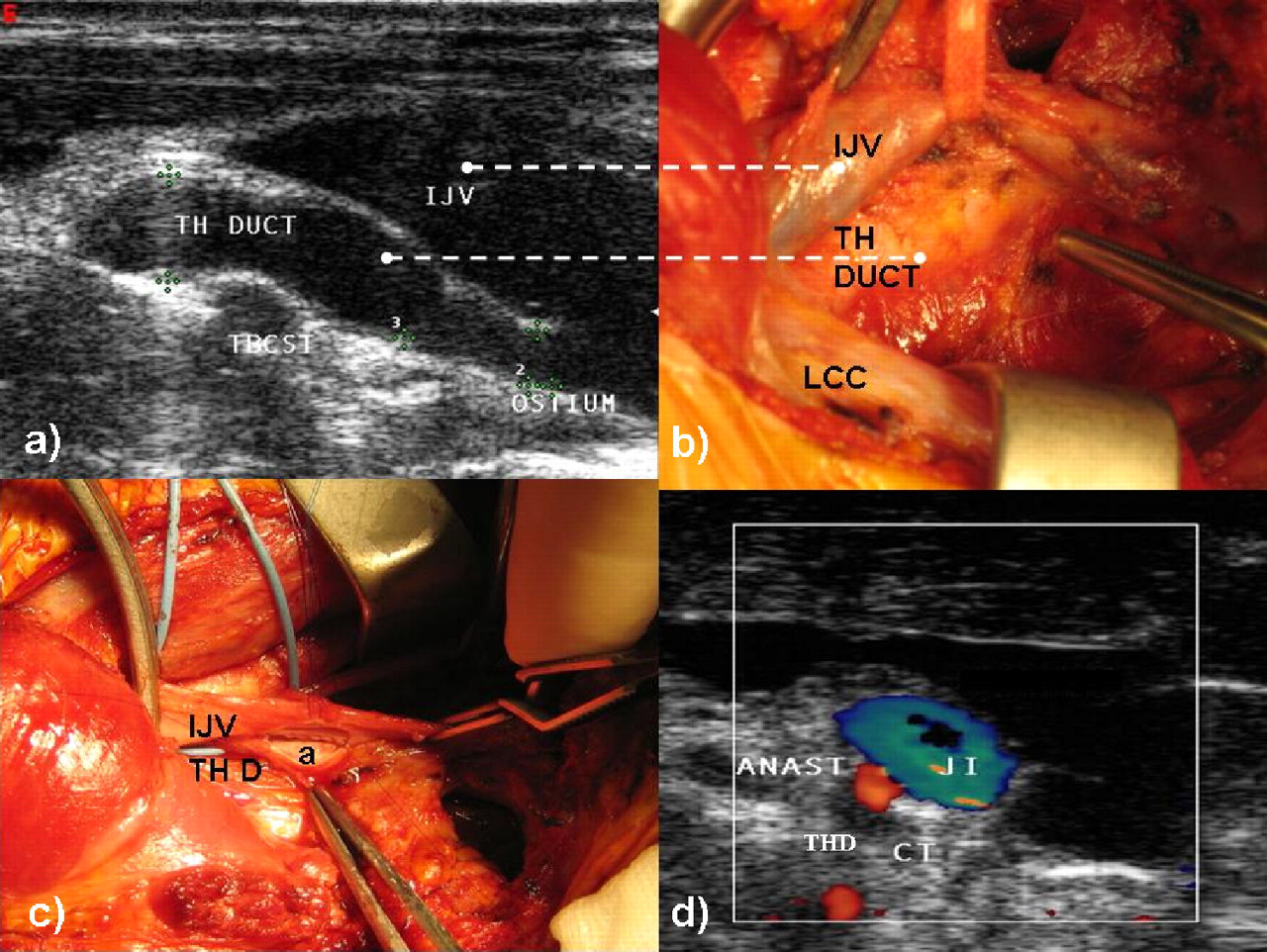
(a) Thoracic duct (TH DUCT) dilation (9 mm) at its confluence with the internal jugular vein (IJV); (b) Preoperative surgical field of the terminal thoracic duct (TH DUCT), placed underneath and between the left common carotid artery (LCC) and the internal jugular vein (IJV); (c) Side-to-side manual anstomosis (a) between the internal jugular vein (IJV) and the thoracic duct (THD); (d) Post-operative echo-colour-doppler check-up of the draining thoracic duct (THD)-internal jugular vein (IJV) anastomosis (ANAST)
Special diet led to an almost complete regression of supraclavicular fossa swelling.
Despite the cervical swelling regression, ECD showed a remaining dilation of the TD (6 mm), which was obstructed by a homogenous and hyperechogenic plug. Compression with the probe was unable to restore the chyle flow into the subclavian vein.
In this case, the performed magnetic resonance imaging (MRI) was deceiving since it just showed a lacunar left supraclavicular fossa effusion, without detecting any dilated TD. A draining procedure was performed because of long-lasting symptoms not responding to medical therapy: it consisted of a side-to-side anastomosis between the TD and internal jugular vein distal to the confluence obstruction (Figures 1b, c and d).
Case 4 (the right-sided SOOTD with a TD confluence septum)
A 41-year-old presented a persistent swelling of the right supraclavicular fossa (Figure 2), which spontaneously appeared 11 months before, without signs of remission and increasing in volume during upper limbs muscular activity.

Right recurrent cervical swelling, increasing in volume during upper limbs muscular activity, caused by an extremely rare case of right sided thoracic duct spontaneous confluence obstruction
The MRI diagnosed a ‘sopraclavicular likely lipoma structure’, which gave indication to surgery.
The subsequent ECD assessed a right-sided thoracic duct, an anatomical variant reported in literature in 2% of the population, 4 draining into the jugular–subclavian confluence, where a TD confluence obstruction was assessed.
The obstruction was visualized as a hyperechoic septum, morphologically resembling a malformative valve, to our knowledge never previously described.
Such precluded chyle flow seemed to be the result of the thoracic duct dilation (6 mm).
Probe compression of the duct was unable to relieve the pathological scenario.
Restricted diet and manual lymphatic drainage, using a specific amount of pressure (less than 9 ounces per square inch) and rhythmic circular movements, confirmed its efficacy in stimulating the lymph flow. 5
At six-month follow-up, a significant clinical improvement was recorded in accordance with a TD calibre reduction (2 mm).
Discussion
Lymphographic TD evaluation is a traditional diagnostic method, but limited by a low detection rate, by a contrast agent need and by a long execution time. Endoscopic ultrasound, CT and, moreover, MRI are feasible, 2 but at the same time limited by their invasiveness and contrast medium use, respectively.
The SOOTD rareness leads to a big lack of medical and surgical approved indications. 1
Conservative (manual lymphatic drainage, diet) and surgical therapeutic strategies have shown interesting results in our reported experience, even if longer follow-up and more numerous cases are certainly required.
This analysis reports a pathological condition characterized by a recurrent cervical swelling, adding to the relative differential diagnosis of an idiopathic TD confluence obstruction. The chyle stop seemed to be due to an ECD detectable malformation of the valve, which is usually located at the jugular–subclavian confluence.
Conclusions
Duplex scan of the supraclavicular fossa, results to be an effective mean to diagnose distal dilations of the thoracic duct. In conclusion, this is a very rare SOOTD report and it offers the basis for further, wider multicentre studies because of the rareness of the condition.