
Abstract
Objective
The purpose of this study was to correlate the clinical findings in the Edinburgh Vein Study with the results of duplex scanning of the deep and superficial venous systems.
Methods
An age-stratified random sample of 1566 people (699 men and 867 women) aged 16–64 were selected from computerized age–sex registers of participating practices (twelve general practices with catchment areas geographically and socioeconomically distributed throughout Edinburgh). Screening included clinical examination, photography and duplex ultrasonography of the superficial veins and the deep veins down to popliteal level. Telangiectasia and varicose veins were graded 1–3 according to severity.
Results
Since there was good agreement between the duplex findings of the right versus left legs, the current analyses are based on 1092 subjects (486 men and 606 women) with complete duplex scan data in their left legs. There was no significant trend of increasing incompetence in either the deep veins only (P = 0.214) or in the combined deep and superficial veins (P = 0.111) with increasing severity of the telangiectasia. There was a statistically significant trend for increasing incompetence in (a) the superficial veins (P = 0.006) and (b) either the superficial or deep veins (P < 0.001) to be associated with advancing grade of telangiectasia. When stratified by gender, significant trends were maintained for male superficial vein incompetence and for either superficial or deep incompetence in both genders. Examination of incompetence in individual venous segments showed that increasing severity of telangiectasia was significantly associated with an increasing proportion of reflux in the upper and lower great saphenous and femoral vein segments. There was no significant association between small saphenous incompetence and increasing grade of telangiectasia.
Conclusion
There is a significant, but not wholly consistent, association between grade of telangiectasia and reflux in both the deep and superficial systems. This association does not apply to the small saphenous system.
Introduction
Telangiectasia, otherwise known as spider veins, hyphen webs, thread veins, sunburst veins, stellate veins and venous flares, are defined in the CEAP (clinical, aetiological, anatomical and pathological elements) classification for chronic venous disorders as a confluence of dilated intradermal venules of less than 1 mm in calibre. 1 Although many patients with telangiectasia are now treated with sclerotherapy or laser therapy, the condition has not been widely studied and its significance in relation to other pathological components of chronic venous disease has not been well defined.
Telangiectases are associated with significant symptoms. 2,3 Although telangiectasia and varicose veins commonly co-exist and indeed share certain histological features, 4 it cannot be assumed that they share a common pathophysiology. Given the association between telangiectasia and reticular and/or varicose veins 5–9 it remains unclear as to whether, and to what extent, symptoms can be attributed to incompetence in the saphenous system, as against small local perforators unconnected to the saphenous system.
An association between telangiectasia and reflux in adjacent reticular veins has been documented by Weiss and Weiss. 7 They reported a study using continuous wave Doppler in 2000 patients with reticular veins and thigh telangiectasias. Patients with saphenofemoral reflux, saphenopopliteal reflux or incompetent saphenous system perforators were excluded. Reflux was heard over reticular veins in 85%, the majority exhibiting the loudest reflux just proximal to the head of the fibula or distal to the lateral femoral condyle. They concluded that lateral and posterior telangiectases connect via thigh reticular veins to small lateral perforators at knee level. In 1969, Albanese et al. 10 described a lateral system of veins which were ‘subdermic’, although not specifically associated with telangiectasia, which connected to the deep system through a lateral system of perforators in the region of the knee.
Somjen et al. 8 studied, with continuous wave Doppler ultrasound, 37 legs (53 sites) with lateral and/or medial thigh telangiectasia. In 47 (89%) sites, they found reticular vein incompetence close to telangiectasia. At 30 sites, the reticular vein incompetence was associated with deeper subcutaneous vein reflux or with perforating vein incompetence.
Thibault (1990) performed duplex ultrasound on 500 limbs in 250 patients who had presented with cosmetic complaints related to varicose and/or spider veins. Incompetence in the superficial venous system (great or small saphenous veins) was documented in 236 (47%) while deep incompetence was present in only six (1%). 6
Engelhorn et al. 11 performed ultrasound scans on 269 limbs of female patients presenting with CEAP Class 1 telangiectasia. They detected great saphenous reflux in 39% and small saphenous reflux in 7%.
Studies such as these have been conducted in clinical series of patients presenting to venous clinics with a range of symptoms relating to chronic venous disease. Epidemiological research in the general population is more scant. In the Basle Study II, Widmer and colleagues examined 1678 men in the 64–75 age group, and reported varicosis in 23% of whom one-third had hyphen webs, one-third reticular and one-third varicosis in the saphenous systems. 11
Criqui et al. 12 conducted a cross-sectional survey in an ethnically diverse population of 2211 men and women. They demonstrated racial differences in the prevalence of visible and functional venous disease and incomplete correlation between clinical and duplex findings. They report telangiectasia in 55% of their population.
Zahariev et al. 13 reported a general practice survey of 26,785 clinic-based subjects of whom 11,724 (44%) reported chronic varicose venous disease and of these 41% had visible telangiectasias.
The demographic features and clinical correlations of telangiectasia in the general population of the Edinburgh Vein Study have been reported previously. 9 The purpose of the present study was to examine the relationship between telangiectasia and patterns of incompetence including deep vein reflux, as demonstrated by duplex ultrasound scanning.
Methods
The Edinburgh Vein Study was a cross-sectional survey of a random sample drawn from the general population of Edinburgh. The study was designed to provide a comprehensive range of clinical, ultrasonic and laboratory data as a baseline for later cohort follow-up. The methodology has been described previously in detail 9 and will be summarized here.
The study population consisted of men and women aged between 18–64 years. An age-stratified random sample was selected from the computerized age–sex registers of 12 general practices, whose catchment areas were geographically and socioeconomically distributed throughout the city. It was calculated that 1500 participants would be required to detect a significant difference in prevalence between groups and to enable the follow-up study to be conducted.
Subjects attended a special clinic where they completed a self-administered questionnaire and were examined, photographed, duplex scanned and had blood taken by a research team comprising a nurse, a technician and a clinical research fellow. The same three researchers were employed for the entire study. Observer variations were minimized by use of standardized simultaneous training and regular correlations of duplicate measurements between observers throughout the study.
The method of examination and classification was adapted from the Basle Study 14 as this was considered to be the best available model at the time for classifying the different categories of venous disease. The CEAP classification, first published by Porter et al. in 1995, was not available when the Edinburgh Vein Study was being designed and recruitment to the study commenced.
The telangiectasia comprised blue intradermal venules <1 mm diameter. Telangiectasia
(CEAP 1) and varicose veins (CEAP 2) were graded for severity, with the help of
photographs from the Basle Study, into three grades according to degree and extent of
tortuosity and prominence of the veins. Figure 1 shows coloured photographs of the different grades of telangiectasia. Telangiectasia: examples of the three grades of severity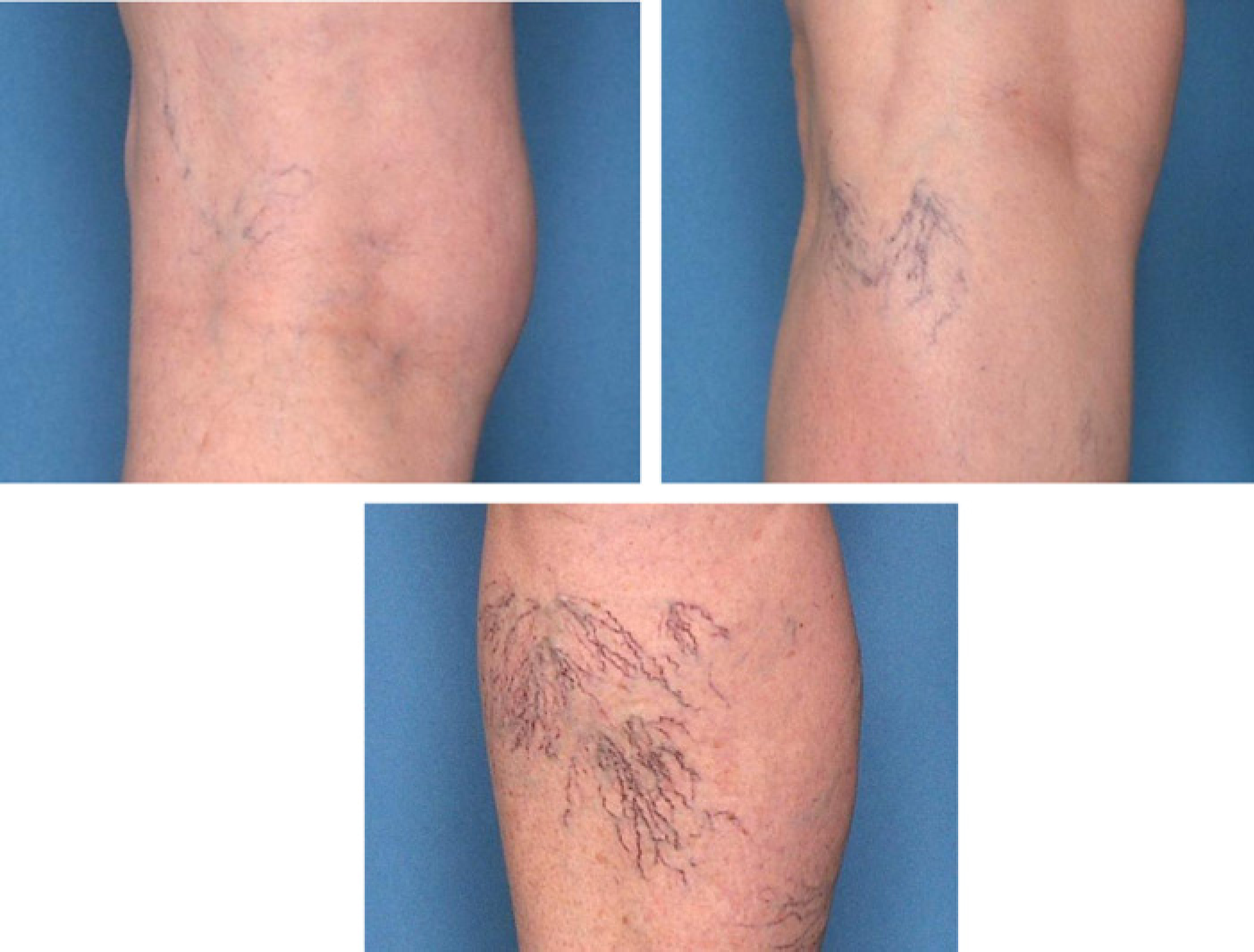
The duplex scans were performed with a Diasonics Prisma VST duplex scanner (Diasonics Sonotron, Zug, Switzerland) using a 5.0 MHz linear array probe. Cephalad venous flow was induced using a pneumatic cuff placed around the calf (cuff width 10 cm, length 50 cm) which was rapidly inflated and deflated using an automatic cuff inflator (Oak Medical, Scunthorpe, UK) to mimic a hand squeeze and the duration of any reflux was measured. 7 Since high-definition duplex scanning was not available to us when the project started, duplex data were therefore limited to an examination of the main stem deep veins and great and small saphenous trunks.
Measurements were made in eight venous segments along the deep and superficial veins of both legs. The deep vein segments examined were the common femoral vein (CFV), proximal to the saphenofemoral junction; the femoral vein (a) approximately 2 cm distal to the confluence with the profunda femoris vein (upper FV) and (b) in the lower third of the thigh (lower FV); and the popliteal vein (a) above the skin crease (above knee popliteal) and (b) below the skin crease (below knee popliteal). The superficial vein segments were the great saphenous veins (a) just distal to saphenofemoral junction (upper great saphenous vein [GSV]) and (b) in the lower third of the thigh (lower GSV); and the small saphenous vein just distal to the saphenopopliteal.
For the superficial segments, reflux of >0.5 second duration was considered to be clinically significant while for each of the CFV, upper and lower FV and above and below knee popliteal segments, reflux of >1.0 second duration was considered clinically significant. 15
Venous segments showing reflux were divided into three groups: (i) superficial segments only; (ii) one or more deep vein segments affected while all the superficial segments were normal; and (iii) one or more superficial segments affected plus one or more deep segments showing reflux. The slides of those subjects with grade 2/3 telangiectasia (who had no history of a varicose vein operation) were examined in detail by two of the authors (CVR and CJE). Sites (medial, lateral, posterior, anterior) of telangiectasia were recorded.
All data were entered into a dBase IV database (dBase Inc., Vestal, NY, USA) and analysed on the Edinburgh University main frame computer using SPSS-X (SPSS, Chicago, IL, USA) and SAS (SAS Institute Inc., Cary, NC, USA) packages. Grade of telangiectasia in the right and left legs were compared using a kappa statistic. Fisher's exact test and the chi-squared test for linear trend were used to compare patterns and location of reflux by grade of telangiectasia.
Results
The Edinburgh Vein Study population comprised 1566 subjects (699 men and 867 women). The mean age was 44.8 years (standard error [SE] 0.43) for women and 45.8 (SE 0.48) for men. The cohort comprised 98.9% white, reflecting the ethnic mix of the city. A total of 1411 (90.1%) subjects were classified as having telangiectasia, 1286 (82.1%) were categorized as grade I, 120 (7.7%) as grade 2 and 5 (0.3%) as grade 3. Due to relatively small numbers, telangiectasia grades two and three have been combined in all subsequent analyses.
When legs were considered separately, the prevalence of right leg grade 1 was 78.3% (1226) and grades 2/3 6.1% (96), while left leg grade 1 was 80.3% (1257) and grades 2/3 5.2% (82) giving a kappa of 0.6. Since there was no difference between the right and left legs, the remainder of this paper is based on those 1092 subjects (486 men and 606 women) with complete duplex data on their left leg.
Associations of superficial and deep reflux with telangiectasia in the left legs of 1092 subjects
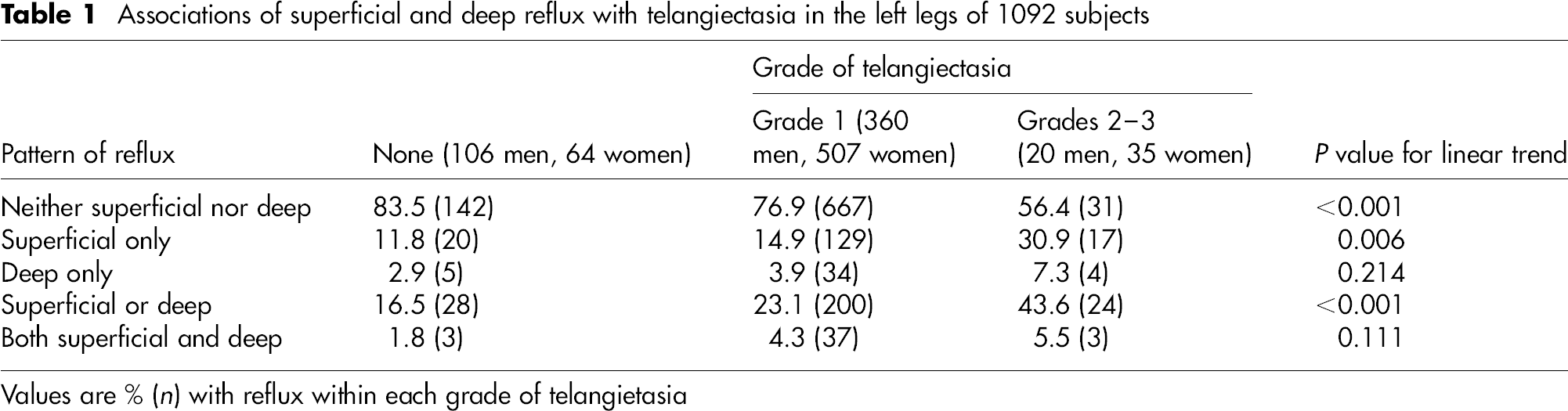
Values are % (n) with reflux within each grade of telangietasia
When stratified by gender, there were no significant trends of increasing incompetence across increasing severity of telangiectasia for deep or for combined superficial and deep veins in either sex, nor for superficial veins in men (data not shown). In contrast, significant trends of increasing vein incompetence among worsening severity of superficial veins (P = 0.009) and for either superficial or deep incompetence were noted (P < 0.001).
Associations between location of reflux and grade of telangiectasia in the left legs of 1092 subjects
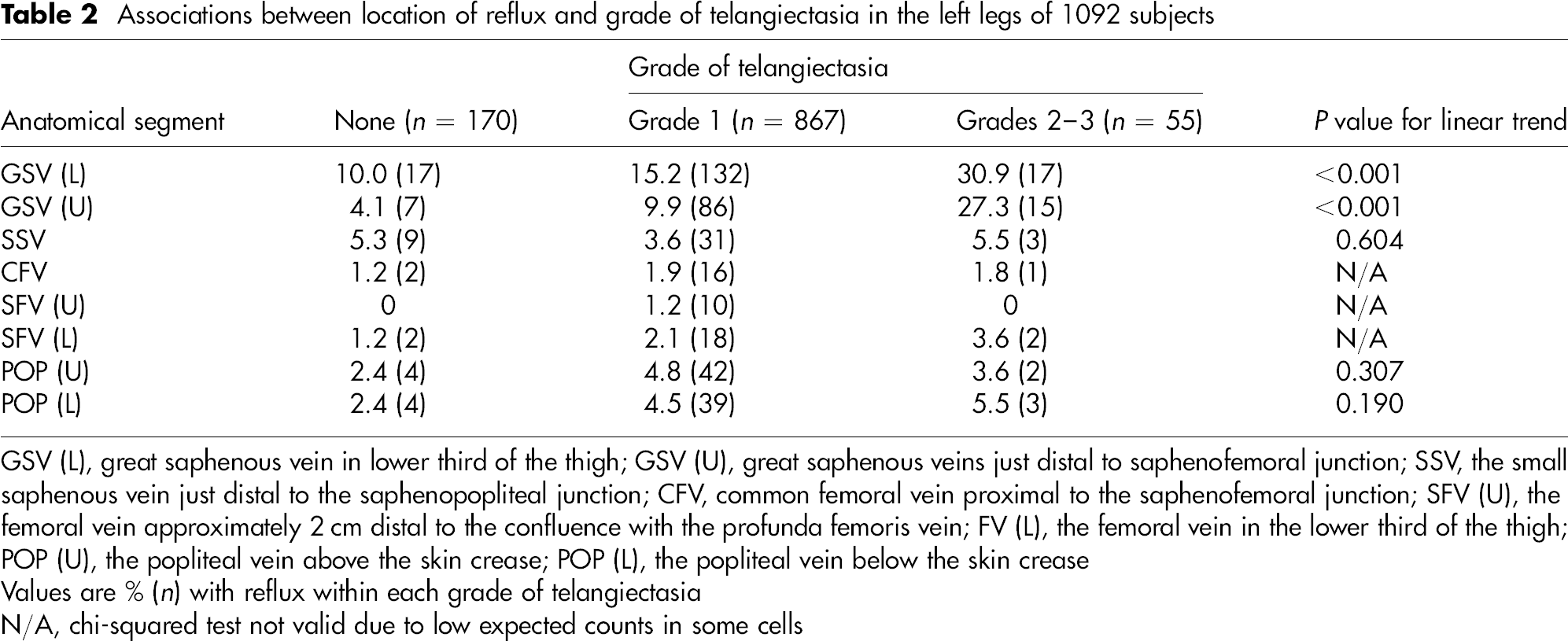
GSV (L), great saphenous vein in lower third of the thigh; GSV (U), great saphenous veins just distal to saphenofemoral junction; SSV, the small saphenous vein just distal to the saphenopopliteal junction; CFV, common femoral vein proximal to the saphenofemoral junction; SFV (U), the femoral vein approximately 2 cm distal to the confluence with the profunda femoris vein; FV (L), the femoral vein in the lower third of the thigh; POP (U), the popliteal vein above the skin crease; POP (L), the popliteal vein below the skin crease
Values are % (n) with reflux within each grade of telangiectasia
N/A, chi-squared test not valid due to low expected counts in some cells
Associations between GSV and SSV segment reflux and site of telangiectasia in the left leg of 52 subjects
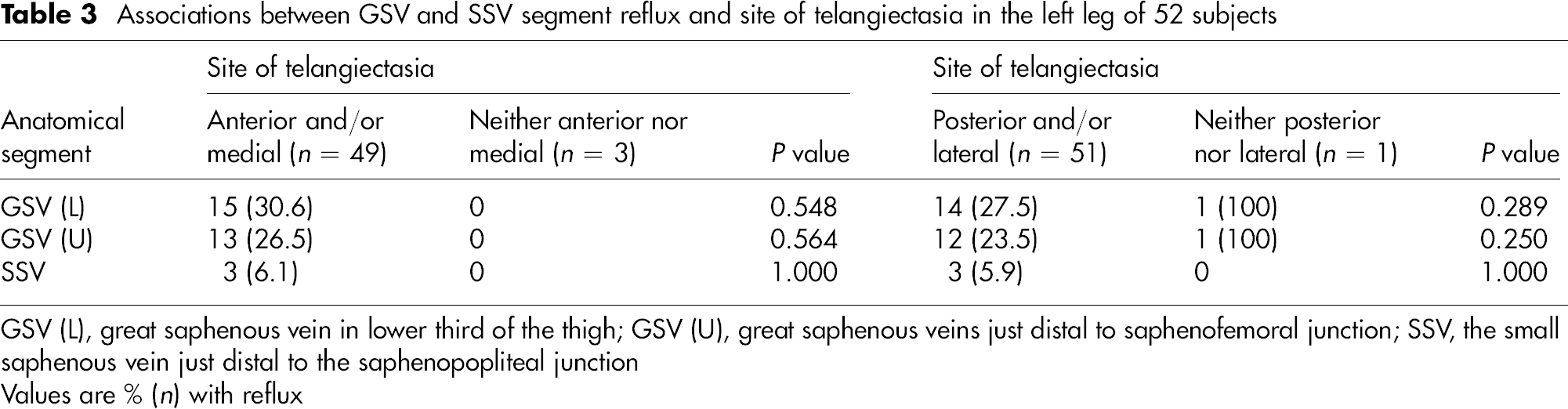
GSV (L), great saphenous vein in lower third of the thigh; GSV (U), great saphenous veins just distal to saphenofemoral junction; SSV, the small saphenous vein just distal to the saphenopopliteal junction
Values are % (n) with reflux
Discussion
There was a significant trend between grade of telangiectasia and increasing reflux in the GSV (upper and lower segments) in the left legs of 1092 subjects. Also significant trends were seen with reflux in the superficial or deep veins, but not with deep vein reflux alone. This may be a small-number issue resulting in low power to detect significant associations.
This study confirms an association between saphenous incompetence and telangiectasia (grades 2 and 3). However, the association is not a strong one: 43.9% of subjects with grades 2/3 telangiectases have no trunk varices (26.7% men, 53.9% women). Furthermore, although we have confirmed that the two conditions commonly co-exist, no deductions can be drawn from our data as to what is cause or effect, i.e whether saphenous reflux is responsible for the development of telangiectasia or vice versa. The fact that 84% of subjects with grade 1 and 66% of those with grade 2/3 telangiectasia have no detectable saphenous reflux indicates that the association is not strong.
Given that the popliteal fossa was the most frequent location for telangiectasia it is interesting that there was no significant association between increasing grade of telangiectasia and small saphenous reflux.
A systematic approach to the therapy of venous disease with prior investigations and elimination of truncal reflux if present before treating telangiectasia is conceptually attractive. However, the weak association between the telangiectasia and saphenous or deep incompetence found in this study offers little support for such a policy.
In this study we did not evaluate reflux in reticular veins. Other studies have shown an association between telangiectasia and reflux in adjacent reticular veins. 7,8
Conclusions
If anatomy is to be fully understood and therapy appropriately directed in patients presenting with telangiectasia, there is a need for studies employing high definition duplex to track reflux in saphenous systems, reticulars and perforators.
Analysis of the follow-up data of the Edinburgh Vein Study population is currently underway, and this may shed light on the evolution of telangiectasia in this population and its association with other components of chronic venous disease.