
Abstract
Objective
Many venous trials mix patients with great saphenous vein (GSV) and small saphenous vein (SSV) diseases. There is no evidence that both respond similarly to treatment and our aim was to test this assumption.
Method
This cohort study compares patients with isolated GSV and SSV incompetence following treatment with open surgical ligation or endovenous laser ablation (EVLA). Outcomes included: quality of life (QoL; Aberdeen Varicose Vein Questionnaire [AVVQ]; Short Form 36 [SF36]; Euroqol [EQ5D]; and Venous Clinical Severity Score [VCSS]).
Results
A total of 370 patients with no differences in baseline QoL, underwent treatment. Despite equivalent morbidity, SSV sufferers had a lower VCSS (P < 0.001). Following surgery, SSV patients scored higher (worse) on AVVQ (P = 0.045) than GSV sufferers, but lower (better) following EVLA (P = 0.042).
Conclusion
The morbidity associated with SSV incompetence is greater than suggested by its clinical severity and responds differently following treatment to that of the GSV. Trials should consider patients with GSV and SSV reflux separately. EVLA may offer additional benefits to SSV sufferers.
Introduction
Endovenous laser ablation (EVLA) for varicose veins is associated with high initial occlusion rates, minimal complication rates and low recurrence rates at five years. Randomized controlled trials (RCTs) and meta-analyses have confirmed the technical efficacy of EVLA in comparison to surgery and other endovenous techniques. 1–4 There is compelling evidence that EVLA offers superior early quality of life (QoL) benefits when compared with surgery. 5
Many of the current trials contain both patients suffering from great saphenous (GSV) or small saphenous (SSV) insufficiency, but there is no evidence that these conditions have a similar impact on QoL or that they respond to treatment in a similar way. It is known that surgery on the saphenopopliteal junction (SPJ) is more hazardous than that on the saphenofemoral junction (SFJ) and that recurrence rates are higher. 6,7 While stripping of the SSV decreases recurrence, it may risk damage to the sural nerve. 7 EVLA of the SSV has been shown to demonstrate good technical success rates and to result in an overall improvement in QoL, 8,9 but little is known of the impact of treatment on QoL following either surgery or EVLA and there is no direct comparison available with treatment of the GSV.
The aim of this study is to investigate whether treatment of SSV incompetence yields similar results to the GSV and thus establish whether the current evidence base (centred on GSV intervention) can be applied in the case of SSV disease.
Materials and methods
All the data utilized in this study have been prospectively collected during an initial period of audit and pilot study work after the initiation of an endovenous ablation programme. All patients presenting to a single vascular unit were screened for suitability.
Inclusion criteria were primary, symptomatic, unilateral venous insufficiency due to isolated SFJ or SPJ incompetence with reflux in the GSV or SSV on venous duplex and a belief by both patient and surgeon that treatment is warranted and likely to be beneficial. Patients with recurrent disease following previous axial treatment were excluded.
Incompetence was defined as reflux > 1 second on spectral Doppler measurement.
Patients were not randomized, but allocated to the procedure of their choice, or the next available convenient list (day-case surgery unit or outpatient local anaesthetic procedure room) if both they and the listing surgeon were indifferent to the planned technique. Neither patients nor assessors were blinded to the procedure undertaken.
Interventions
All conventional surgical procedures were performed under general anaesthetic. In the case of the SPJ, preoperative duplex marking was employed. The aim of surgery was to perform a flush ligation of the junction with inversion stripping of the GSV to the knee or the SSV to the mid-calf where possible. Any incompetent perforators were accurately marked with duplex, allowing ligation via a 1–1.5 cm incision, and concomitant ambulatory phlebectomy was performed via stab incisions using a vein hook or a Kockherised mosquito clip. Mepore® dressings (Mölnlycke Health Care, Göteborg, Sweden) were applied to incised wounds and Steri-strips™ (3M, St Paul, MN, USA) to stab avulsion sites. Compression was initiated with bandages, which were substituted for Class II (20–30 mmHg) graduated compression stockings worn 24 hours a day for the first week and during the day for a further five weeks.
All EVLA procedures were performed under local tumescent anaesthesia in a dedicated procedure room within the outpatients department. Patients were preoperatively marked using duplex ultrasound. A 5F catheter was introduced into the vein using the Seldinger technique and its tip was accurately positioned at the junction using ultrasound. The patient was then put in the Trendelenburg position and perivenous tumescent local anaesthetic (40 mL of 2% lignocaine with 1:200,000 adrenaline in 1 L of 0.9% saline) was infiltrated along the vein and varicosities. Total local anaesthetic did not exceed the recommended maximum safe dose per patient. A sterile bare-tipped 600 nm laser fibre was introduced via the catheter for laser ablation of the GSV or SSV. Endovenous laser energy was delivered using an 810 nm diode laser generator (Diomed/Angiodynamics, Cambridge, UK) at 14 W power, continuous mode. Target energy delivery was 60–80 J/cm. Perforator ligation and ambulatory phlebectomy was performed concomitantly as in the surgical group as a single procedure; this is known to improve outcomes. 10 Compression was applied for one week using Panelast® (Lohmann & Rauscher International GmbH & Co. KG, Rengsdorf, DE, USA) elastic adhesive bandage, after which it was replaced by a Class II (20–30 mmHg) full-length graduated support stocking for a further five weeks.
All patients were discharged with Diclofenac 50 mg three times daily and Paracetamol 1 g four times daily to be taken regularly for one week. Patients were followed up at one week, six weeks, three months and one year.
Outcomes
The primary outcome measure was disease specific QoL using the Aberdeen Varicose Vein Questionnaire (AVVQ). This instrument has been shown to be reliable, valid and responsive, 11–13 and records the specific impact of venous disease on patient's QoL and is scored from 0 (no impact) to a theoretical maximum of 100.
Secondary outcomes
Postprocedural pain scores (10 cm visual analogue scale on days 1, 3 and 7) were noted in a patient diary, as were the number of days to return to normal activity and work.
Objective assessment of venous disease was performed using the venous clinical severity score VCSS (0 represents no significant venous disease and 30 is the maximum score). VCSS has been shown to be a valid, sensitive and responsive measure of the severity of varicose veins. 14,15
Generic QoL analyses were performed using the Short Form 36 UK version 1 (SF36) and Euroqol (EQ5D) instruments. The SF36 utilizes 36 items to derive eight domains each scored from 0 (worst possible) to 100 (best possible). The EQ5D utilizes responses to five domain questions which are transformed using a time trade-off tariff to a global index, scored on a scale of −0.513 (worst score) to 1 (best score). Both have been validated and utilized as a measure of efficacy and effects of varicose vein treatment. 11–13,16–22
All QoL instruments were recorded independently by the patients themselves on a voluntary basis. Each questionnaire was then checked and patients encouraged to complete any missing responses.
Statistical analysis
All data were recorded into a dedicated database (Microsoft Access, Redmond, WA, USA) and analysis performed utilizing SPSS (Chicago, IL, USA). A standardised statistical analysis protocol was used:
Continuous data were first tested for normality. Normally distributed data were analysed with t-test and quoted as mean (95% confidence interval) for dependent variables or mean (standard deviation) for independent variables. Non-parametric data were analysed using Mann-Whitney U test and Wilcoxon-signed rank test for paired data and quoted as median (interquartile [IQR] range). Friedman test was used to analyse multiple related samples across the study period. Categorical data were analysed using chi-squared or, if necessary, Fisher's exact test. No assumptions were made about the direction of any relationships and therefore two-tailed inference testing was employed throughout. The threshold significance level used in the analysis was 0.050 and values outside this are explicitly referenced in the text.
Continuous data are presented using standard statistical notation in box and whisker plots. The box indicates the IQR and the median represented by a line within the box. The whiskers represent the range of data within 1.5× IQR below the first quartile and above the third quartile.
Results
Figure 1 outlines the number of patients involved in analysis at each stage. Table 1 represents the baseline scores. The groups were similar in terms of age, sex and baseline QoL scores, with no significant differences. There was, however, a difference in baseline VCSS scores, where patients with GSV reflux score significantly higher than those with SSV reflux (P < 0.001) (Figure 3).
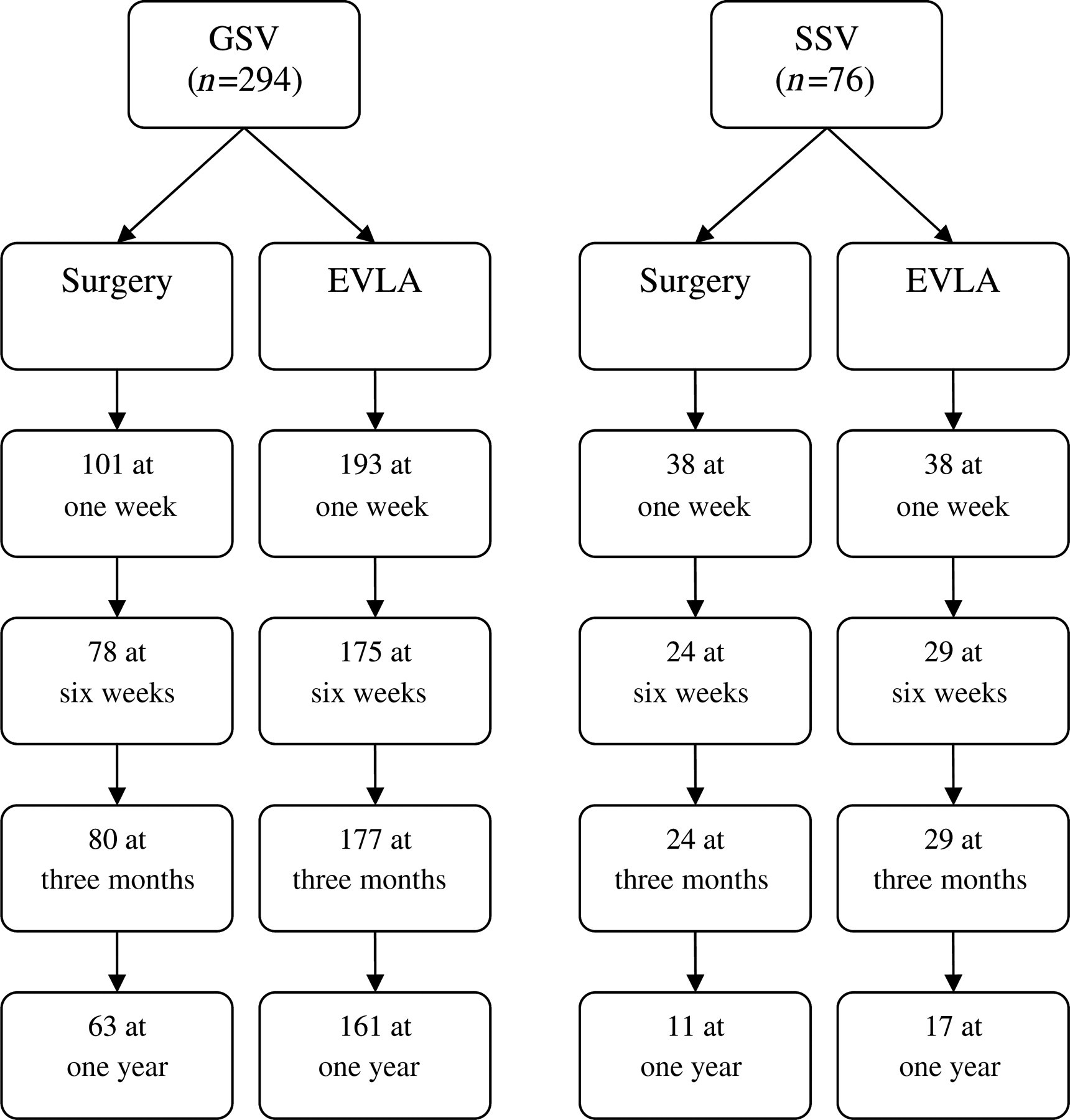
Numbers of patients used in the analysis at each time point
Baseline Results
EVLA, Endovenous laser ablation; VCSS, Venous Clinical Severity Score; AVVQ, Aberdeen Varicose; EQSD, Euroqol Index
Vein Questionnaire figures are quoted as median (IQR) unless otherwise stated
Postprocedural pain scores were very low overall. There was no significant difference between GSV and SSV sufferers in terms of perceived pain scores on day one (1.6 [0.4–3.9] versus three [0–5.9] – postsurgery, [P = 0.581], 1.3 [0–3.0] versus 1 [0.1–2.5] – post-EVLA [P = 0.582]), day three (1.6 [0.4–3.9] versus 3.0 [0–5.9] – postsurgery [P = 0.098], 0.3 [0–1.5] versus 0.2 [0–1.6] – post-EVLA [P = 0.801]) and day seven (0.5 [0–2.8] versus 0.6 [0–3.5] – postsurgery [P = 0.551], 0 [0–1] versus 0 [0–0.6] – post-EVLA [P = 0.202]).
There was no statistical difference in the number of days taken to return to function when comparing GSV and SSV disease. The number of days to return to work were GSV – 14 (11–28) versus SSV - 17.5 (8.5–21) – postsurgery (P = 0.595), six (2–10) versus four (2–14) – post-EVLA (P = 0.656) and return to normal activities 14 (7–21) versus 12 (2.5–26) – postsurgery (P = 0.734), four (1–14) versus three (2–14) – post-EVLA (P = 0.504).
Primary outcome measure: disease specific quality of life (AVVQ)
Intragroup analysis: Both GSV and SSV patients show a significant improvement in disease specific QoL over the study period following both treatments (GSV [surgery] – P < 0.001; GSV [EVLA] – P < 0.001; SSV [surgery] – P = 0.001; SSV [EVLA] – P < 0.001) (Figure 2). Prior to this improvement, GSV patients see a significant initial deterioration in AVVQ scores at one week (surgery – P = 0.005; EVLA – P < 0.001). Likewise this is seen post surgery in the SSV group (P = 0.046), but does not reach significance with SSV patients receiving EVLA (P = 0.075).
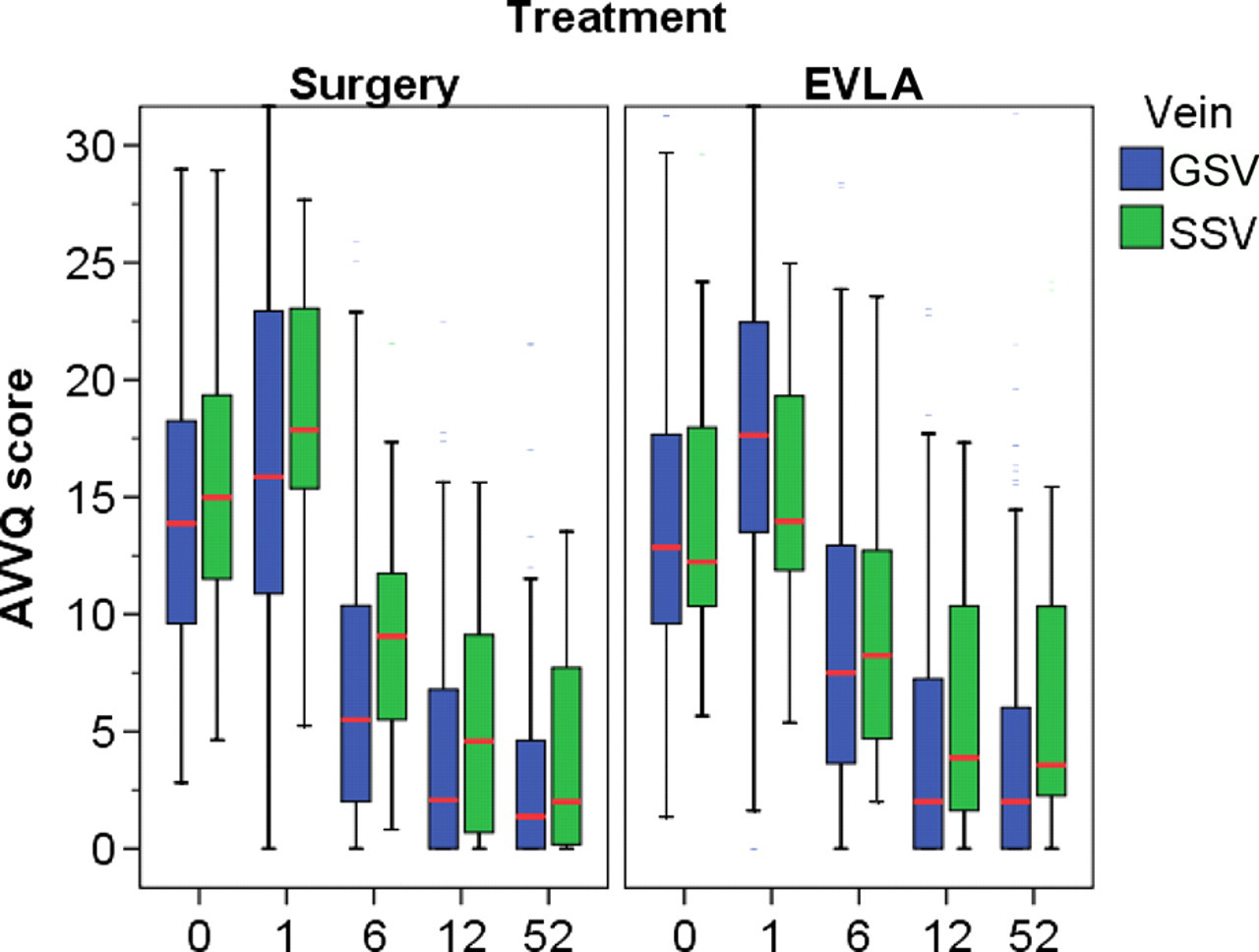
Aberdeen Varicose Vein Questionnaire results over time in weeks
Intergroup analysis: Overall, patients suffering from SSV reflux have higher AVVQ scores post treatment than GSV patients (P = 0.006). If this is broken down by treatment, following surgery the AVVQ scores for patients with SSV disease are higher and reach statistical significance at six weeks (P = 0.045). However, following EVLA the reverse is true and SSV sufferers score lower at one week (P = 0.042).
VCSS scores
Intragroup analysis: As with AVVQ, all four groups show a significant improvement following treatment (GSV [surgery]) – P < 0.001; GSV [EVLA] – P = 0.001; SSV [surgery] – P = 0.043; SSV [EVLA] – P = 0.001) (Figure 3).

Venous Clinical Severity Scores over time in weeks
Intergroup analysis: There were no postprocedural differences observed.
Generic quality of life
Intergroup analysis: The most notable difference in SF36 domains was observed in Social function, where six weeks post-SPJ surgery patients recorded significantly lower scores than post-SFJ surgery (P = 0.015). Following EVLA the scores were the same (P = 0.292) (Figures 4 and 5). A similar trend was observed in role limitation due to physical disability (physical role), with lower scores in the SSV patient group following surgery, but this failed to reach statistical significance with these numbers.
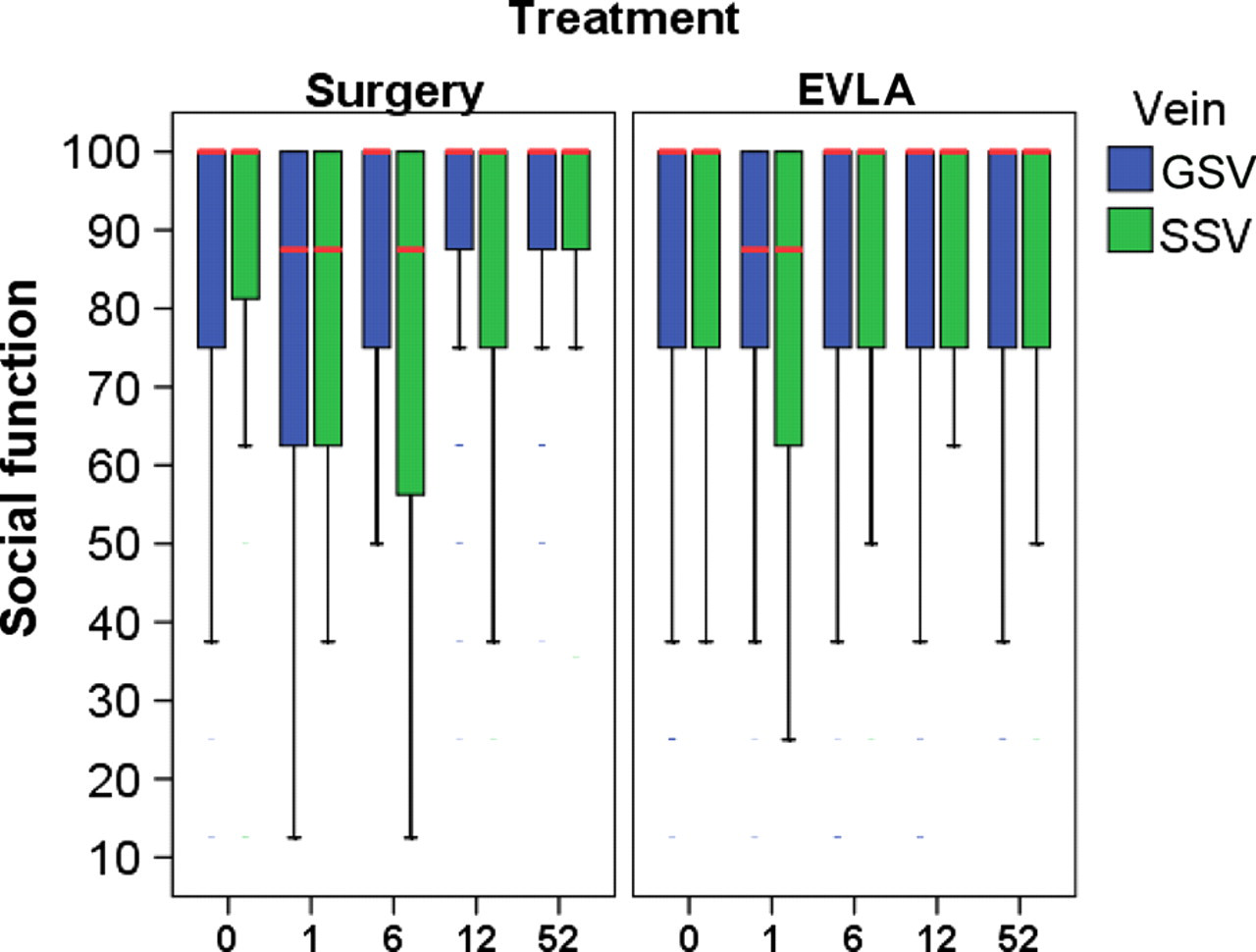
Short Form-36 social function domain over time in weeks
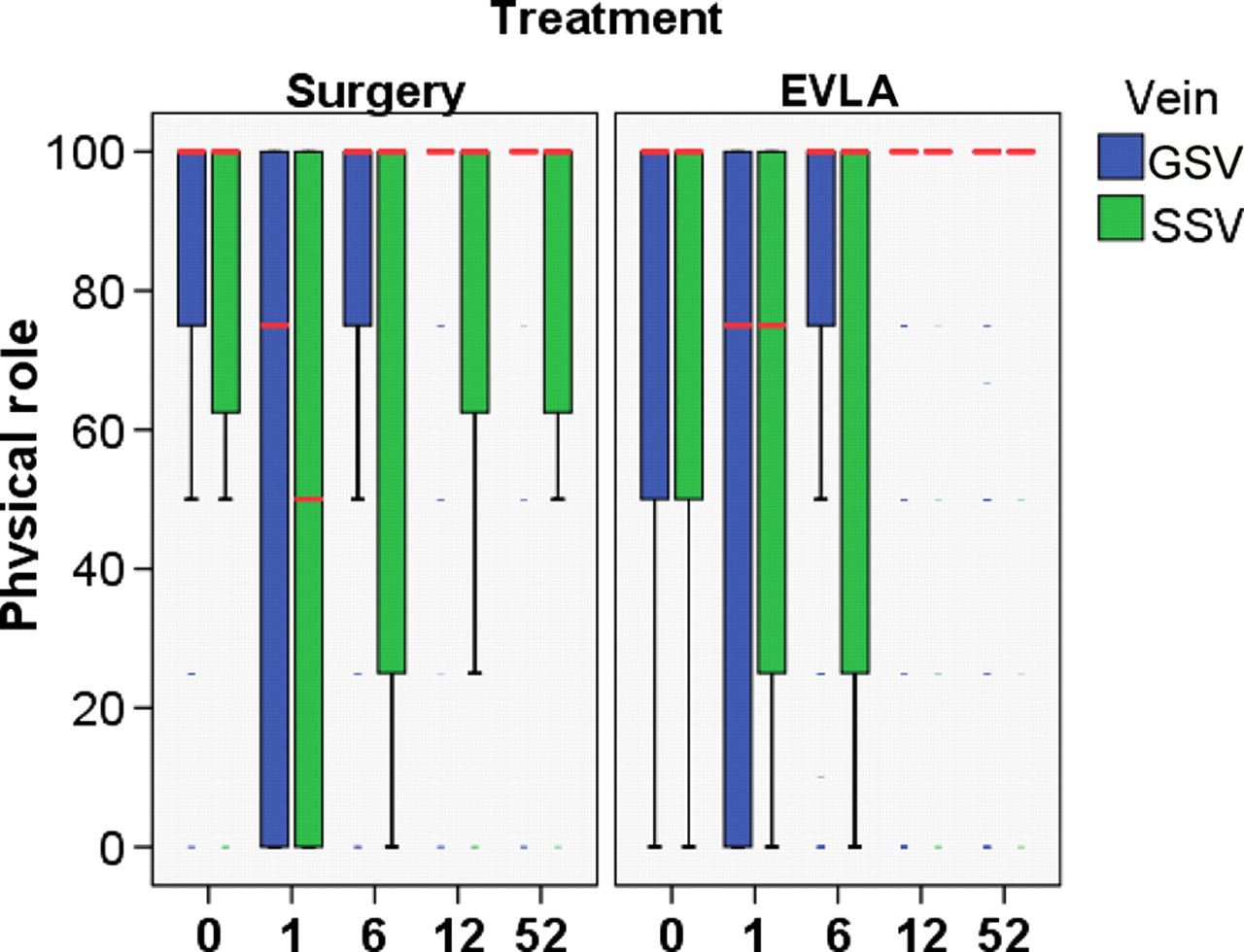
Short Form-36 physical role domain over time in weeks
There were no significant differences between either axis in terms of EQ5D scores over the time period.
Complications
Patients with SSV disease tended to suffer more complications following treatment (sensory disturbance – P = 0.003; deep venous thrombosis – P = 0.042) (Table 2). Two deep vein thromboses were seen at one week post-SSV surgery. Both patients were anticoagulated and by six weeks had a re-canalized and competent vein, with no sequelae by one year. EVLA of the SSV was associated with a significantly higher incidence of sensory disturbance than EVLA of the GSV (P = 0.021). A similar trend following conventional surgery did not reach significance with these numbers (P = 0.110).
Complications given in absolute figures, with percentages in brackets
GSV, great saphenous vein; SSV, small saphenous vein; EVLA, endovenous laser ablation; DVT, deep venous thrombosis
Discussion
This retrospective cohort study was an examination of a high-quality data-set prospectively collected in the context of everyday practice to assess the hypothesis that isolated incompetence of these two superficial venous axes result in similar morbidity and respond in a similar manner to treatment. This is not a randomized study and there was no attempt made to blind investigators or patients. Care must be taken in interpretation: a comparison of the two treatments for the same disease pattern should optimally be made in the context of randomized trials. This study does, however, offer evidence against the above primary hypothesis and some insight into the relative merits of the two treatment strategies.
The baseline results highlight an important point: those suffering from saphenopopliteal incompetence and small saphenous reflux tend to result in a lesser degree of clinical severity on objective scoring than those with great saphenous disease, despite suffering comparable QoL impairment at presentation. This is a novel finding; objective clinical assessment of the severity of small saphenous varicose veins underestimates the negative effect of this disease on sufferers. This clearly has implications in commissioning, where increasingly intervention is being rationed by clinical severity.
The significant improvements seen in clinical and QoL scores following treatment demonstrate the efficacy of both treatments and have been described previously. 1,3,5 This study suggests that following saphenopopliteal surgery, patients suffer a greater disease specific QoL impairment than following saphenofemoral surgery, but in contrast may do better following EVLA.
Saphenopopliteal surgery was observed to have a greater negative effect on social function than saphenofemoral surgery, but no detectable difference was seen following EVLA. There was no real difference clearly observed in the other domains, although trends were present. This implies that there may be additional benefits of EVLA for small saphenous disease compared with great saphenous over conventional surgery. It is difficult to explain these differences; in particular there was no difference in pain or recovery times and there were higher rates of sensory disturbance following small saphenous EVLA when compared with great saphenous ablation.
QoL analysis is subject to high degrees of variability, particularly in the context of venous dysfunction. The poor control of external variables offered by this methodology has decreased the power of this study to detect discrepancies, but differences between these disease patterns were seen nonetheless. The existing literature comparing treatments in the context of great saphenous (or predominantly great saphenous) insufficiency cannot simply be assumed to be true for small saphenous dysfunction; rather separate RCTs or appropriately powered subgroup analyses should be established and multiple regression modeling should be applied to future comparisons of the two different disease patterns. This evidence base can then be used to inform decision-making in both a clinical and commissioning context.
Footnotes
Acknowledgements
Thank you to A I Mekako for his significant assistance in the recruitment and initial follow-up of these patients.