
Abstract
Objective
Chronic post-traumatic arteriovenous fistula (AVF) is a late complication of vascular injury and can be presented with symptoms of congestive heart failure, venous hypertension and distal ischaemia. We present an unusual case of chronic ischaemic leg ulcer in young adult caused by post-traumatic AVF.
Case report
A 29-year-old male patient was admitted to our hospital with symptoms of chronic ulcer located on the lateral side of the lower left leg. Arterial pulses distally from the groin were absent. His medical history revealed him to have sustained gunshot injury of the left thigh in the war conflict 18 years before. Angiography showed a large AVF between superficial femoral artery and femoral vein. The patient underwent surgical repair of AVF with reconstruction of superficial femoral artery by saphenous vein interposition under spinal anaesthesia. Completion angiography confirmed AVF exclusion. Leg ulcer healed within a month.
Conclusion
Chronic leg ulcer may be the only symptom of large post-traumatic AVF in young adults.
Introduction
Post-traumatic arteriovenous fistula (AVF) may be a complication of stab wound, blunt trauma, gunshot injury or even fracture. Most often it occurs after medical interventions or diagnostic procedures such as angiography or surgical interventions that have caused inadvertent trauma to the artery and vein. 1
Clinical symptoms depend on the size and location of AVF. Small AVFs located on extremities are usually asymptomatic and are identified accidentally. 1,2 Larger AVFs present with prominent superficial veins, oedema of a limb or, in the case of larger communication between artery and vein, with the symptoms of congestive heart failure. 3 Large AVF can produce symptoms of distal ischaemia and present like symptomatic peripheral artery disease. We present history, clinical findings, diagnosis and successful treatment of chronic ischaemic leg ulcer as a complication of post-traumatic AVF in a young adult.
Case report
A 29-year-old male patient was admitted to our hospital with the symptoms of chronic ulcer located on the lateral side of left lower leg (Figure 1). The ulcer developed after minor accidental scratch six months before admission. Arterial pulses were absent distally from the groin. Left foot was colder than the right one. Scars from the old penetrating gunshot wound were found on the medial and contralateral side of the left thigh. Over the scar on the medial side of the thigh, audible murmur and palpable thrill were detected. The patient's medical history revealed him to have sustained a high-velocity gunshot injury of the left thigh at age 11 during the war in Croatia. He was operated on; however, no medical documentation was available. Current clinical examination and diagnostic evaluation showed no symptoms of congestive heart failure and we found no prominent superficial veins. The patient did not complain of intermittent claudications.

Chronic leg ulcer at admission
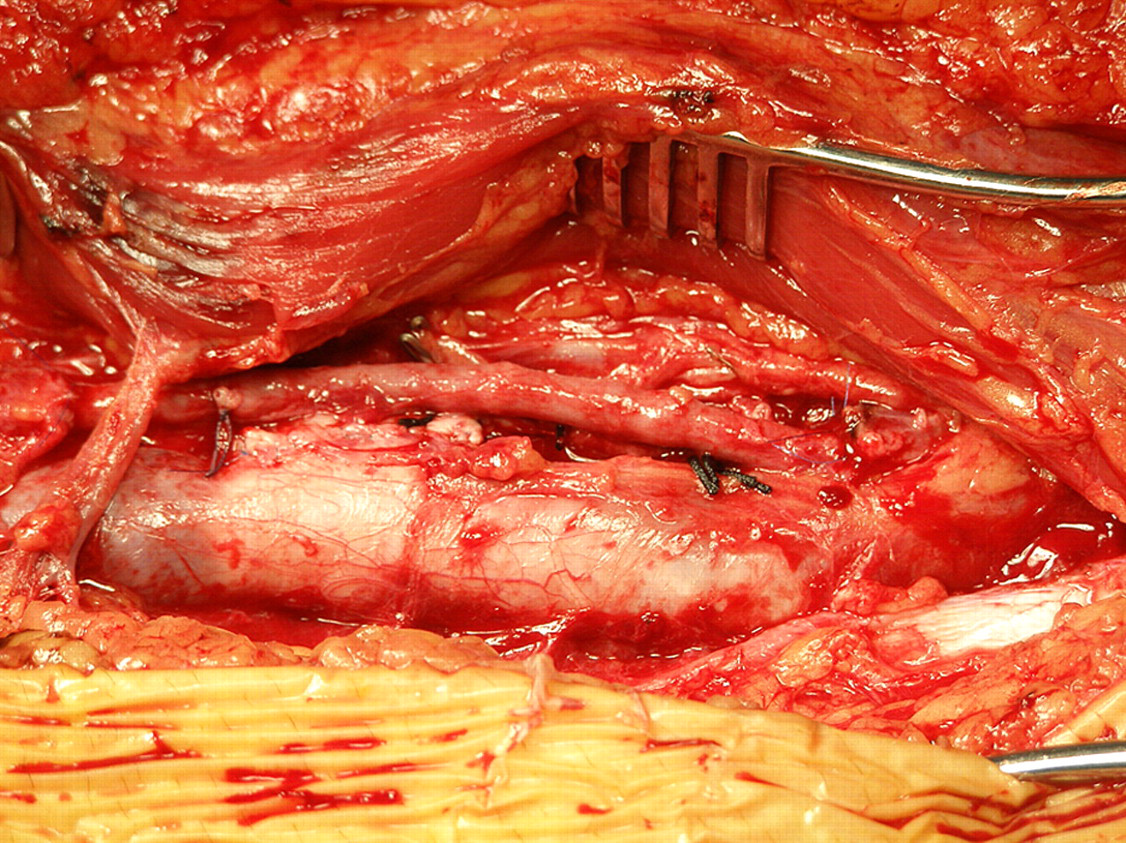
Angiography showed a large communication between the middle third of the superficial femoral artery and femoral vein of the left thigh (Figure 2). Reconstruction of femoral vessels was indicated. Under spinal anaesthesia, AVF was approached directly by linear incision in the Hunter region. After the preparation of the superficial femoral artery, vein and fistula between them (Figure 3), the patient was administered a bolus of heparin sulphate (5000 units) intravenously. Upon cross-clamping the proximal and distal parts of the fistula, we separated the superficial femoral artery and femoral vein by longitudinal incision. The superficial femoral vein was primarily repaired by continuous suture (Prolene 5-0). Because of the arterial wall changes, the superficial femoral artery was reconstructed by interposition of the vein graft in the length of 5–6 cm, previously taken from the opposite leg (Prolene 6-0) (Figure 4). Completion angiography showed good intraoperative result (Figure 5). After bleeding control, the wounds were closed by layers by continuous suture. In the postoperative course, pedal pulses of the left leg were palpable. The patient was discharged from the hospital on postoperative day five without any complications.
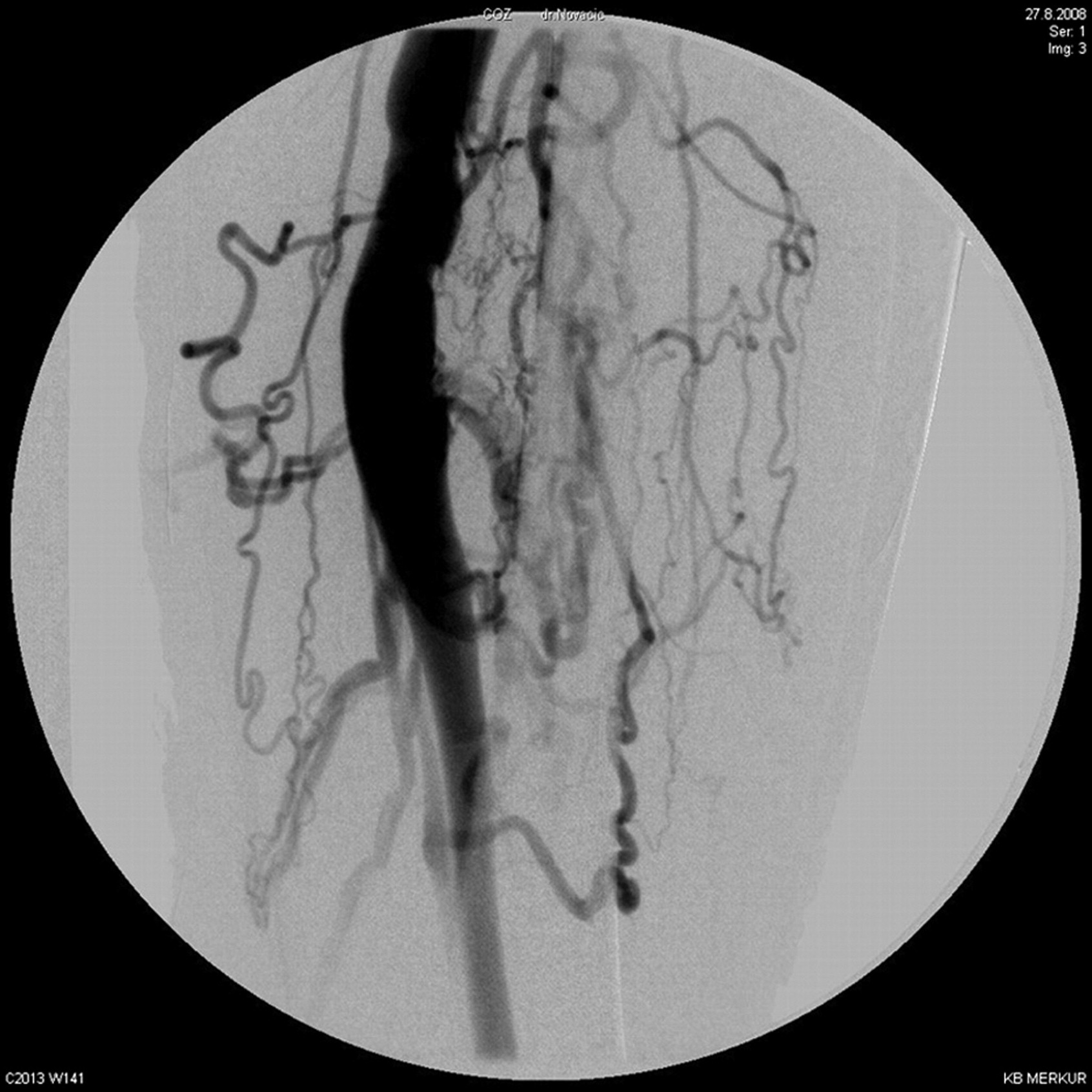
Preoperative angiography shows a large communication between left superficial femoral artery and femoral vein

Arteriovenous fistula after preparation of the superficial femoral artery and vein
Intraoperative findings after surgical repair of the fistula with reconstruction of the superficial femoral artery by vein graft interposition
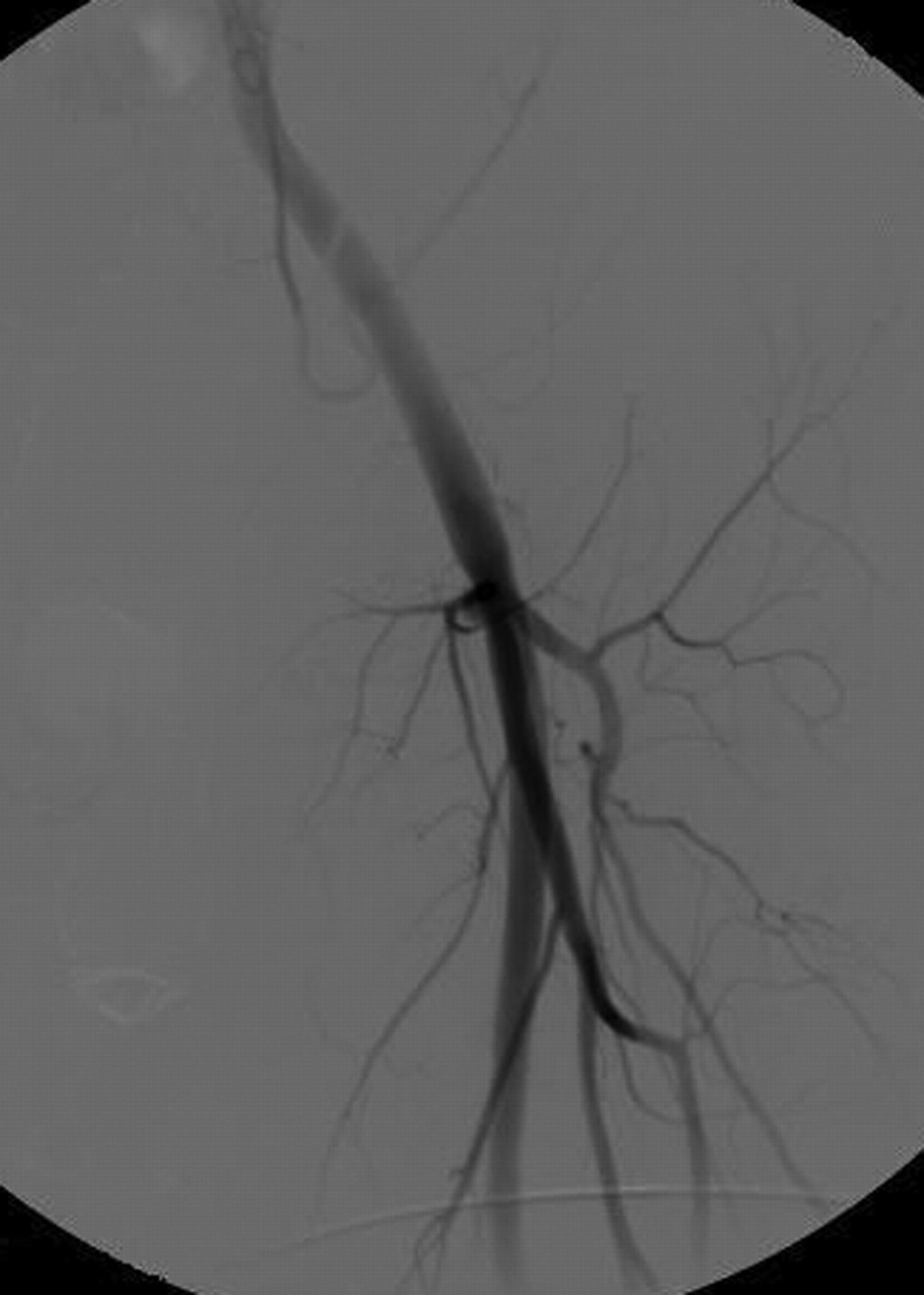
Postoperative angiography after surgical repair of arteriovenous fistula
First follow-up was scheduled one month after discharge from the hospital. Ischaemic ulcer was healed (Figure 6), pedal pulses on both sides were palpable and there was no difference in pedal skin temperature. Duplex control of peripheral arteries showed good results. After two-year follow-up, the patient had no evidence of AVF with normal vascular status of the leg.

Healed ischaemic ulcer and pigmentation of the distal third of the left lower leg one month after treatment
Discussion
AVFs of lower extremities are mostly seen in the femoral region as a complication after medical interventions, usually angiography or other interventional procedures. The incidence of post-traumatic AVF increases during armed conflicts with numerous gunshot injuries. Gunshot injuries are usually managed by emergency surgical intervention and AVF can persist as a late complication, 2,4 as in the case of in our patient who had sustained a high velocity gunshot injury as an 11-year-old child during the war in Croatia. Eighteen years after the injury, he presented with an ischaemic ulcer, after an accidental scratch, as a symptom of inadequate perfusion of the left lower leg. Most post-traumatic AVFs are asymptomatic and are detected accidentally. Symptomatic AVF can present with leg enlargement, dilated superficial veins and symptoms of congestive heart failure or rarely distal ischaemia. 3,5 However, persistence of chronic ischaemic leg ulcer without claudications is a rare complication of post-traumatic AVF and this differential diagnosis should also be considered. The risk of congestive heart failure increases with the duration of AVF patency, particularly if the fistula is large and occurs in approximately 3% of patients. 3 Rich et al. 2 reported that only 6.3% of 588 patients with AVF had a diagnostic delay by more than six months after the injury. The diagnosis of AVF can be confirmed with duplex ultrasonography scan, however, angiography is still the superior diagnostic tool for AVF detection and treatment planning, particularly for chronic AVF. Computed tomography and magnetic resonance angiography are alternative diagnostic modalities. 1
When repair of AVF is indicated, surgical or endovascular procedure may be performed, depending on anatomical characteristics and technical possibilities. 6,7 In addition, patients should be evaluated for early repair whenever it is possible due to technical difficulties associated with venous hypertension produced by AVF. 8
When surgical repair is performed, the artery and vein are separated from each other and the joint regions are reconstructed. If the anastomosis cannot be performed without tension due to the loss of tissue, autogenous saphenous vein or synthetic graft can be used in vascular reconstruction. Alternatively, endovascular repair offers some advantages as a less invasive procedure; however, it is associated with the risk of embolization, thrombosis of stent-graft, maldeployment, endoleak and recurrence. Embolization may be an option for small AVFs, but more often endovascular approach to AVFs involves the use of a covered stent. 6
In conclusion, AVF is a vascular complication resulting from penetrating trauma. The diagnosis of AVF should be considered in patients with a history of extremity injury and leg ulceration, even without classical AVF symptoms. Surgical repair can be safely performed to avoid further haemodynamic changes and complications.