
Abstract
Introduction
‘Localized’ femoral vein thrombosis (FVT) is a relatively rare condition usually associated with traumas, external compression or iatrogenic etiologies and the consequence can be pulmonary embolism.
Report
This is the case of a 46-year-old woman who presented with pulmonary emboli secondary to ‘localized’ superficial FVT, coupled with post-puncture arteriovenous fistulas (AVFs), two days after trans-femoral vein radio-frequency cardiac ablation. After placing a temporary IVC-filter, the AVFs were sutured directly while the residual FVT was treated conservatively.
Discussion
Close local monitoring and adequate medical and surgical management are mandatory to avoid possible dangerous complications, also in apparently ‘low-risk’ iatrogenic AVFs.
Keywords
Introduction
Deep venous thrombosis and pulmonary embolism are rare complications after femoral vein catheterization. 1 In this report, we describe the case of a 46-year-old woman who presented with pulmonary emboli secondary to ‘localized’ superficial femoral vein thrombosis (FVT) coupled with postpuncture iatrogenic arterovenous fistulas (AVFs). The patient had been submitted to transfemoral vein radio-frequency cardiac ablation and the AVFs had been treated conservatively. The aim of this report is to discuss this original case of postpuncture FVT coupled with multiple iatrogenic AVFs and presenting as pulmonary emboli.
Report
A 46-year-old woman presented with pain in the left thoracic wall associated with dyspnoea two days after femoral vein catheterization. She had undergone percutaneous radio-frequency cardiac ablation for the management of recurrent atrioventricular nodal re-entrant tachycardia through right femoral vein access. The patient showed no evidence of haematological risk factors for thromboembolic disease. Vein catheterization was performed without ultrasound (US)-control and was difficult due to adiposities. After the procedure she developed a haematoma and a systolic bruit in the groin. Duplex ultrasound scans evidenced two small AVFs between the superficial femoral vein and the origin of the superficial femoral artery and excluded a local deep vein thrombosis. Short-duration local US-oriented compression was applied for 240′ with no after-effects. Considering the limited size of the AVFs and the absence of lower limb oedema or venous hypertension, the patient was discharged under low-dose subcutaneous anticoagulation therapy, planning the elective treatment of the AVFs. Two days later, she developed severe pain in the right thoracic wall, particularly during deep breaths coupled with dyspnoea. An emergency pulmonary computed tomography (CT) revealed an acute pulmonary embolus in the vessel feeding the middle lobe (Figure 1). A CT-scan of the abdomen and lower limbs also revealed a small residual ‘floating thrombus’ in the superficial femoral vein at the vein puncture level, which was identified as the source of pulmonary embolism; two small AVFs were also identified proximally and distally to the residual superficial FVT (Figure 2). After placing a temporary transjugular IVC-filter to avoid mobilization of thrombus material during surgical manoeuvres the patient was operated and the AVFs were sutured directly (Figure 3). The residual superficial FVT was treated conservatively and the patient was discharged under full anticoagulation therapy per os. The IVC filter was removed three weeks later and anticoagulation therapy was continued for 10 months. No new onset of FVT or recurrence of pulmonary emboli was observed at 12-month follow-up.
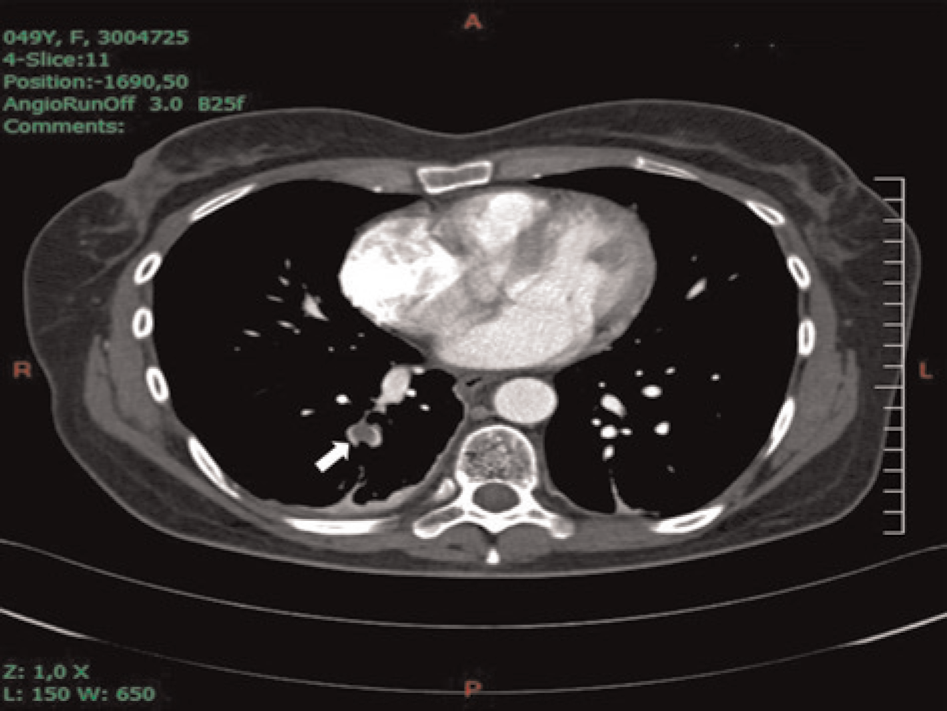
Angio-CT: embolus in the vessels feeding the middle lobe (arrow). CT, computed tomography

Angio-CT: small residual ‘floating thrombus’ in the superficial femoral vein at the vein puncture level (large dashed arrow); two small AVFs, were also documented, proximally and distally to the thrombus (thin arrows). The common femoral vein distal to the AVFs is markedly dilated. CFV, common femoral vein; AVFs, arteriovenous fistulas; CT, computed tomography
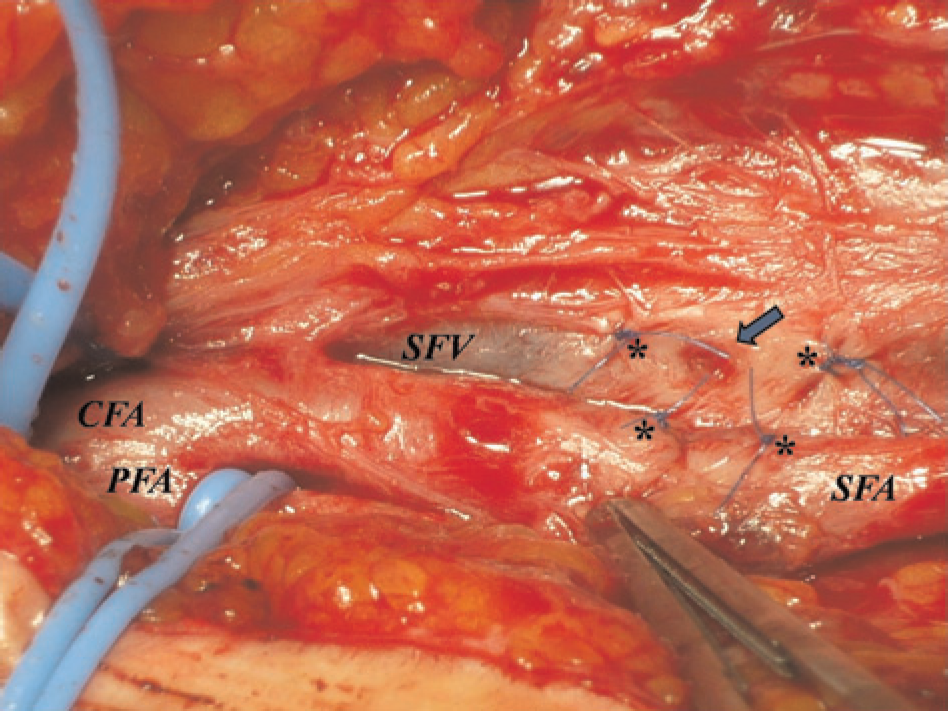
Intraoperative imaging. Suture of two small AVFs between the superficial femoral artery and vein (asterisks). The arrow shows a small postpuncture vein wall injury at the puncture level; presumably, the SFV thrombosis developed in this site. CFA, common femoral artery; SFA, superficial femoral artery; PFA, profunda femoris artery; SFV, superficial femoral vein; AVF, arteriovenous fistulas
Discussion
The incidence of iatrogenic postvascular-puncture complications (PVPC) has considerably increased in recent years because of the large number of endovascular procedures performed, particularly in cardiology. 1 Pseudo-aneurysms represent the most frequent PVPC in cardiac procedures while ‘localized’ FVT is a relatively rare but dangerous event. 1 In fact, few clinical cases of isolated FVT have been reported, particularly in the presence of external venous compression due to enlarging haematoma, mechanical inguinal compression or prolonged cardiac procedures. 2,3 A challenging problem in cases of repeated attempts of femoral vein catheterization is the damage to the vessel wall which significantly increases the risk of thrombosis at the puncture site, 2,3 resulting in pulmonary emboli if not recognized and treated early. In this particular case, the repeated vein punctures (Figure 3), associated with venous catheterization during prolonged cardiac procedure, may have caused sufficient trauma to the venous wall to explain the successive development of the superficial FVT. Also the local venous compression due to inguinal haematoma and the insufficient anticoagulation therapy probably played a major role. 3,4 In this case, the responsibility of the external mechanical groin compression is irrelevant considering the short duration of the compression and the late FVT-onset.
On the other hand, the role of the AVFs in promoting pulmonary embolism seems critical. The location of the AVFs, proximally and distally to the residual ‘floating thrombus’, suggests their responsibility in promoting thrombus fragmentation, mobilization and its consequent pulmonary migration. Also, the radiological characteristics of the ‘floating thrombus’ clearly show its embolic potentiality (Figure 2).
Regarding the prophylactic measures to decrease the rate of PVPCs, an accurate selection of the puncture site is mandatory. 2–4 In a large review of PVPCs only 16% of all AVFs were found between the common femoral artery (CFA) and vein, while 84% of all AVFs were found after groin puncture below the level of CFA. 5 Possible strategies for accurate vessel puncture, e.g. in patients with poorly palpable pulses, should include the use of ultrasound and the visualization of anatomical landmarks like the capitulum of the femoral bone. 5
Conclusions
It has recently been suggested that in cases of ‘non-haemodynamic’ iatrogenic AVFs a conservative management for at least one year should be justified. 6 This original case shows how close local monitoring and adequate medical and surgical management are mandatory to avoid severe general complications, also in apparently ‘low-risk’ AVFs.
Footnotes
Acknowledgements
The authors wish to thank Elena Harwood for the linguistic revision of this paper.