
Abstract
Objective
To define the anatomical variations of small saphenous vein (SSV) for varicose vein (VV) surgery by three-dimensional computed tomography venography (3D-CTV) and to analyse the impact of this preoperative evaluation on surgical outcomes.
Methods
A total of 120 consecutive limbs with SSV insufficiency having undergone VV surgery from January 2005 until December 2007 were enrolled. The medical records and images were analysed retrospectively.
Results
The relationship between SSV and gastrocnemial vein (GNV) were categorized into two: (a) SSV and GNV drained to popliteal vein (PV) separately (100 limbs, 87%) and (b) SSV and GNV made common channel which drained to PV (15 limbs, 13%). Saphenopopliteal junction morphology was normal (75 limbs), severe tortuosity near PV (19 limbs), ampullary ectasia (4 limbs) and duplicated drainage to PV (2 limbs). No recurrence of VV was noted.
Conclusions
CTV can provide thorough preoperative anatomic information of the SSV variations and reduce the recurrence of VV.
Introduction
Duplex ultrasound (DUS) can provide both anatomic and haemodynamic information of the venous system in the lower extremities. DUS is now considered as the gold standard investigation for varicose veins (VV). 1–3
Meanwhile, due to the recent advances in computed tomography technology and computer-assisted image processing, three-dimensional computed tomography venography (3D-CTV) can be used for preoperative evaluation of the VV. As we reported previously, CTV has lots of advantages for the diagnosis and treatment of the VV, especially in clinically difficult situations, such as recurrent VV, popliteal fossa varicosity or pelvic varicosity. 4
Surgery for small saphenous varicose veins has been reported to be more challenging with a higher complication rate and recurrence rate than surgery for great saphenous veins. 5,6 One of the major causes of recurrence is failure to obliterate the saphenopopliteal junction (SPJ) correctly, probably because of anatomic variabilities. 7
Recently Schweighofer et al. 8 reported the anatomic variations of the small saphenous vein (SSV) by cadaveric dissection. They provided some specific details on topographic anatomy concerning the SSV and reported their collected data for basic research background and for future comparison with DUS-based studies. As they mentioned, ‘back-to-basics’ understanding of the anatomic variation is critical in proper management of the disease. We have applied CTV technology for VV surgery for a few years and we think these objective 3D images can be a better data-set for topographic anatomic evaluation than DUS.
The aim of this study is to define the anatomical variations of SSV by 3D-CTV for VV surgery.
Materials and methods
A list of the patients who underwent VV surgery at Seoul National University Hospital from January 2005 until December 2007 was extracted from the Vascular Registry database. Among the 440 patients who underwent VV surgery, patients with duplex-proven reflux in the SSV were selected. Ten cases of popliteal fossa varicosities without SSV reflux and seven of SSV reflux treated with endovenous laser therapy were excluded because the aim of the current study was identification of surgical anatomy for SSV and the proportion of those cases was small. A total of 120 limbs in 103 patients with SSV insufficiency who underwent VV surgery were enrolled. Twenty-seven limbs had both GSV and SSV insufficiency. The medical records, DUS and 3D-CTV images were analysed retrospectively.
Preoperative imaging
After history-taking and physical examination, DUS and 3D-CTV were performed preoperatively as described previously. 9 In brief, DUS and CTV were done, mostly on the same day. CTV was done first with a 16-MDCT (Sensation 16, Siemens Medical Solutions, Erlangen, Germany) scanner. CT images were reconstituted with a personal computer-based 3D reconstruction software (Rapidia; Infinitt, Seoul, Korea). Saphenous veins and perforators larger than 1 mm were detected and marked on the CT volume-rendering images. The presence of reflux in axial veins and the marked perforators was evaluated by duplex. Retrograde flow more than 0.5 seconds was considered as the presence of perforator reflux. Surgeons reviewed this information preoperatively and CT volume-rendering images were used as road maps during the operation.
Operation
Under the spinal or general anaesthesia, the patient was laid in a prone position. A small 2 cm-sized transverse incision was made along the popliteal skin crease. After opening the fascia, SSVs were retracted and divided. Proximal SSV was ligated near SPJ and distal SSV was partially stripped down to upper- or mid-calf level for prevention of sural nerve injury. Perforator ligation and varicosectomy were done with minimal stab incisions, if needed.
CTV image analysis
The CTV images were retrospectively reviewed by two expert radiologists (EP and WL). The type of SSV termination, SSV morphology, the relationship between SSV and gastrocnemial vein (GNV), and the relationship between SSV and adjacent nerves were recorded.
Statistical analysis
Data analysis was performed with SPSS (version 17 for Windows XP; SPSS Inc) software. Univariate analysis was obtained by Student's t-test. Significance was determined to be at P < 0.05.
Results
Patient demographics
A total of 120 limbs in 103 patients were enrolled. There were 57 (55.3%) women and 46 (44.7%) men with a mean age of 55 ± 11 years (range 22–75 years). All limbs had SSV insufficiency confirmed by DUS and underwent conventional operations of high ligation, segmental stripping and varicosectomy. Family history of VV was present in 19.4%, obesity (body mass index greater than 25 kg/m2) in 37.9%, diabetes in 9.7% and hypertension in 25.2%. Bilateral VV was found in 16.5%. CEAP (clinical, aetiological, anatomical and pathological elements) clinical grades were C2 in 106 cases (88.3%), C3 in 13 (10.8%) and C4 in 1 (0.9%).
SSV termination
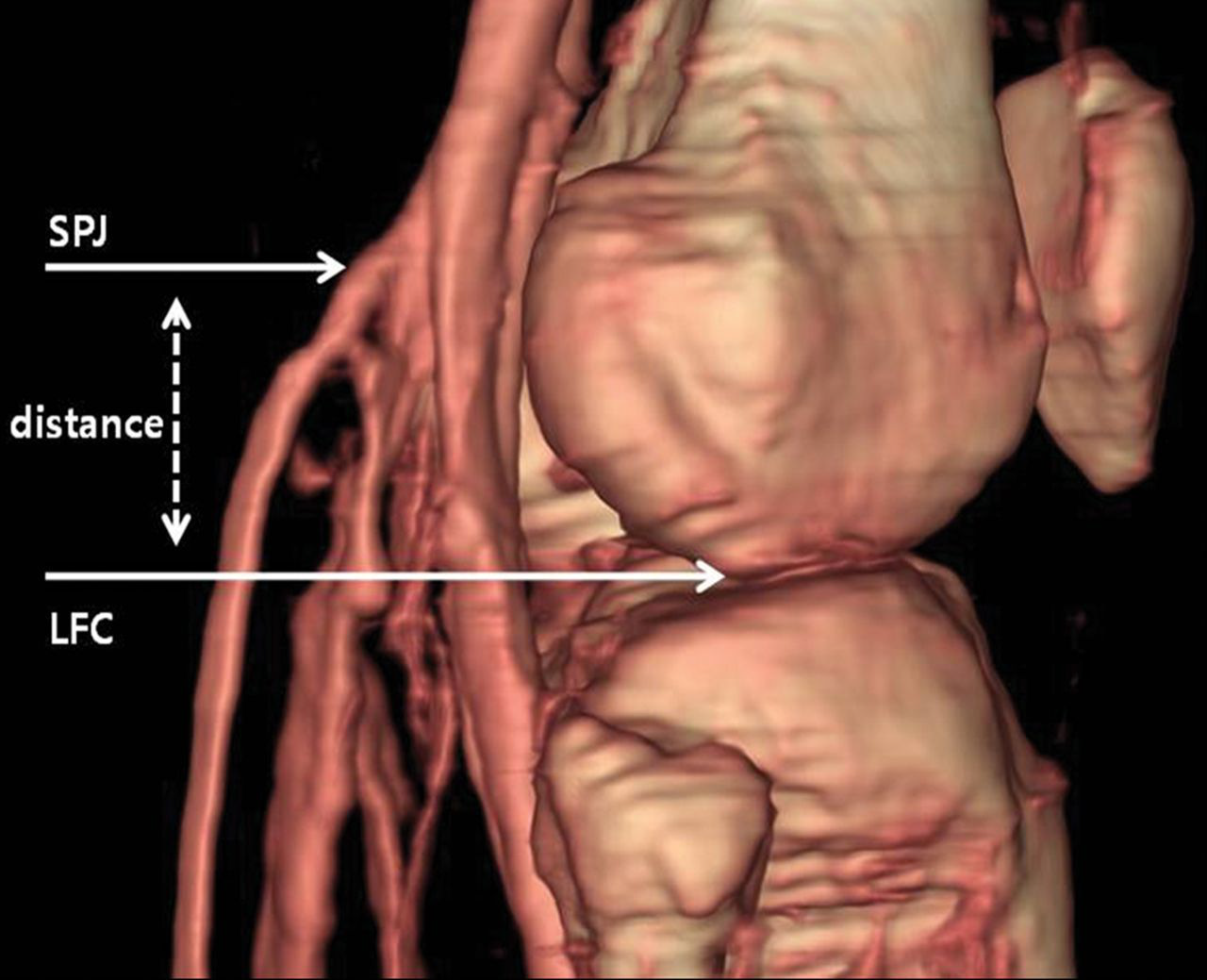
SSV terminated to popliteal vein (PV) in 115 limbs (95.8%) with SPJ in popliteal fossa. SSV terminated to the veins above the popliteal fossa without SPJ in five limbs (4.2%), including femoral vein in two, great saphenous vein in two and deep femoral vein in one (Figure 1). Among 115 limbs with SPJ, mean vertical distance between SPJ and lower margin of femoral condyle (LFC) was 44.7 ± 15.47 mm (range: 42.4–87.2 mm). LFC is considered as the location of the popliteal crease, where surgical incision was usually made. The vertical distance was longer than 5 cm (high SPJ) in 44 limbs (38.3%). Thigh extension (TE) of SSV was encountered in 74 limbs (64.4%), which had a longer mean vertical distance between SPJ and LFC than limbs without TE (47.5 ± 15.28 mm versus 39.6 ± 14.65 mm, P < 0.01) (Figure 2).
Various types of small saphenous vein (SSV) termination in the popliteal fossa. Type A, saphenopopliteal junction (SPJ) with no significant thigh extension (34.1%). Type B, SPJ with thigh extension (61.7%). Type C, no SPJ (4.2%). PV, popliteal vein Distance between saphenopopliteal junction (SPJ) and lower margin of femoral condyle (LFC) was measured in three-dimensional volume rendering images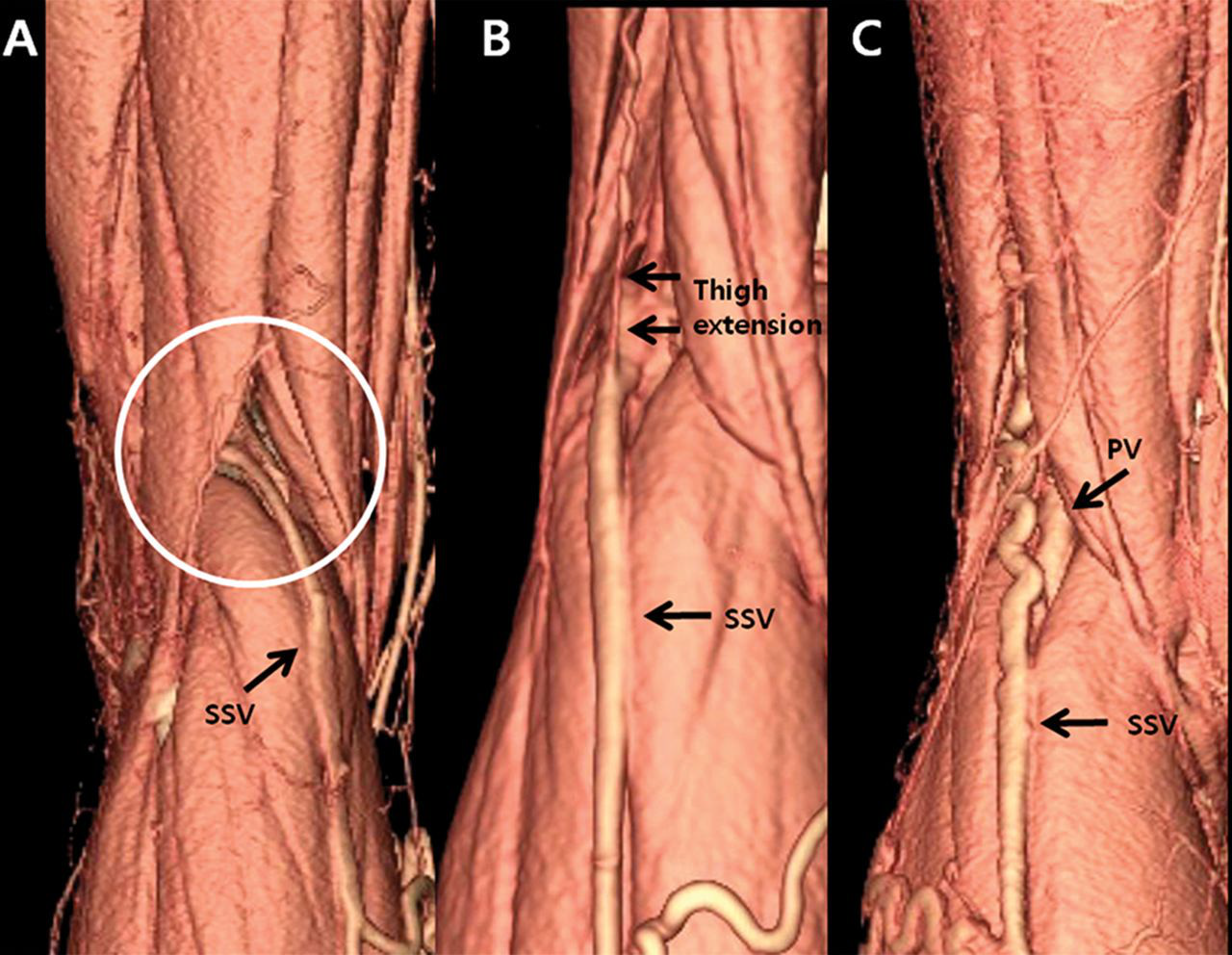
Relationship between SSV and GNV
The relationship between SSV and GNV was classified into two types: (A) SSV and GNV drained to PV separately (100 limbs, 87%), (B) SSV and GNV made common channel which drained to PV (15 limbs, 13%) (Figure 3). In type B, the SSV was ligated just peripheral to the junction of the SSV–GNV confluence.
Relationship between small saphenous vein (SSV) and gastrocnemial vein (GNV). (A) SSV and GNV drained to popliteal vein separately. (B) SSV and GNV made common channel before entering popliteal vein. PV, popliteal vein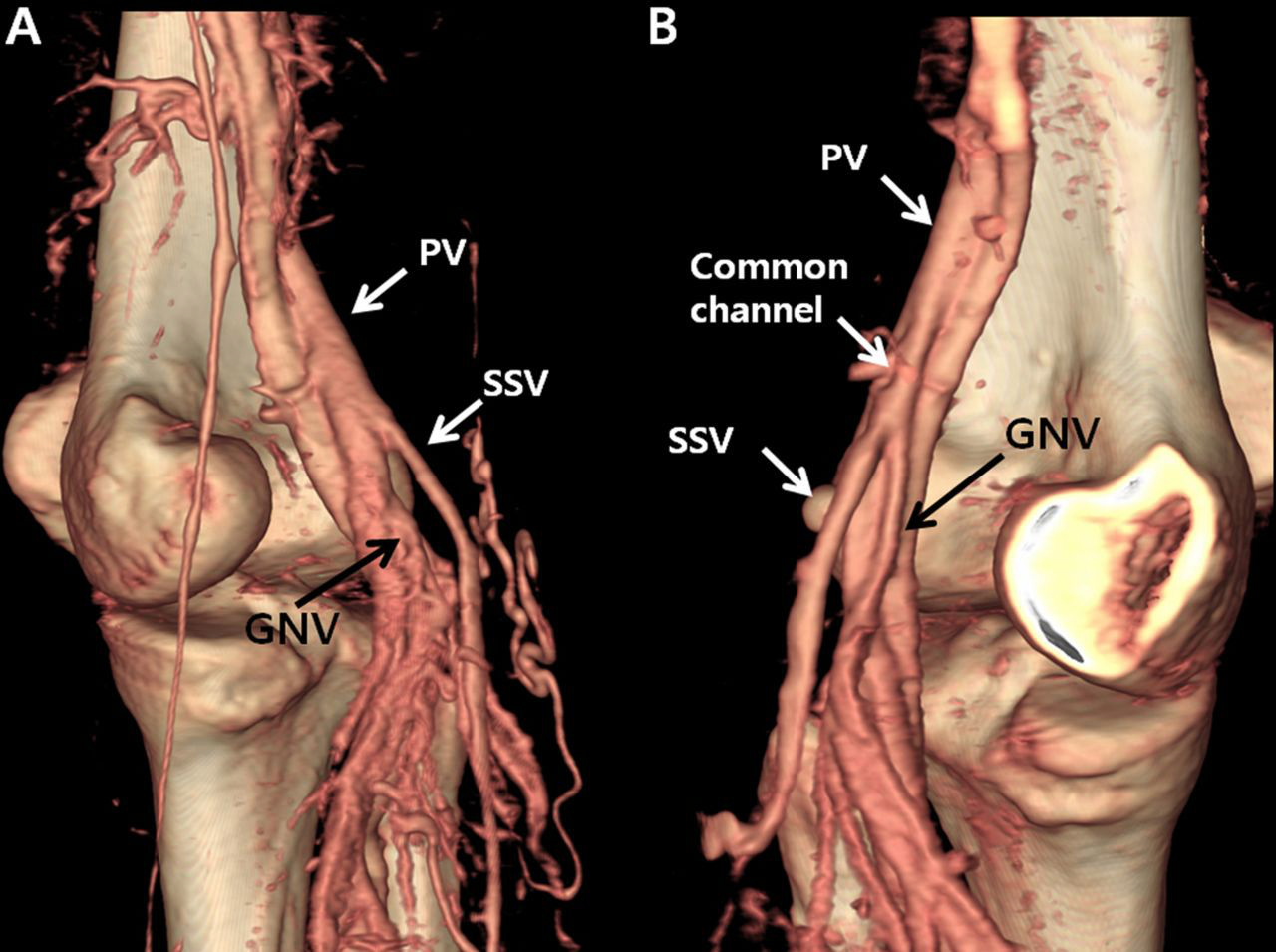
SPJ morphology
SPJ morphology was evaluated in the aforementioned type A SSV–GNV relationship. Single straight vein at SPJ which was ligated with no difficulty during the operation was considered as normal and found in 75 limbs. Anomalous SPJ was found in 25 limbs, which needs more meticulous surgical technique for ligation. This included severe tortuosity near PV in 19, ampullary ectasia in four and duplicated drainage of SSV in two (Figure 4).
Various morphologies at saphenopopliteal junction: A, normal; B, tortuosity; C, ampullary ectasia and D, duplicated drainage. PV, popliteal vein; SSV, small saphenous vein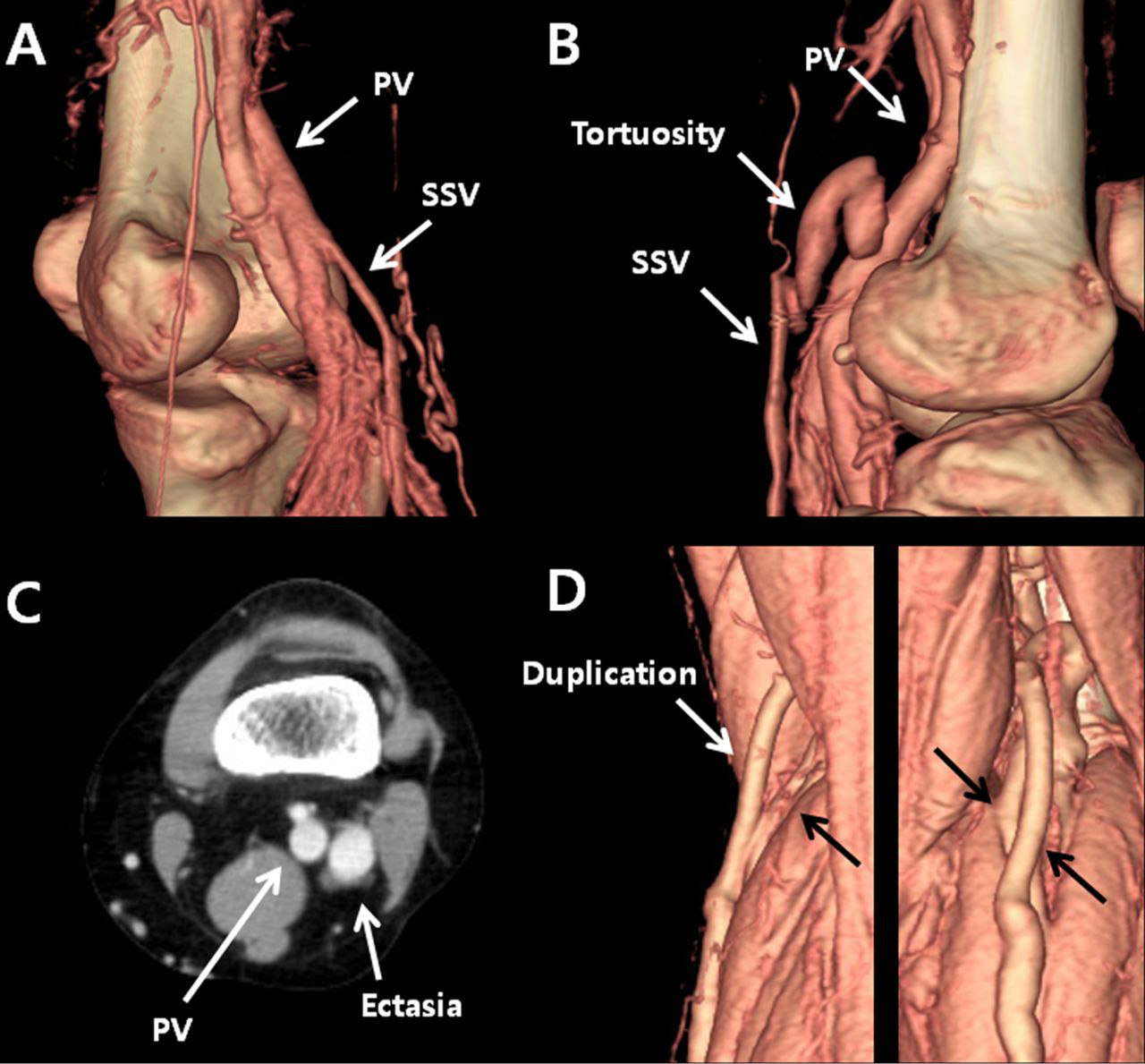
Neural topography
Location of small saphenous vein (SSV) in relation to the nerves at the level of the origin of gastrocnemius muscle
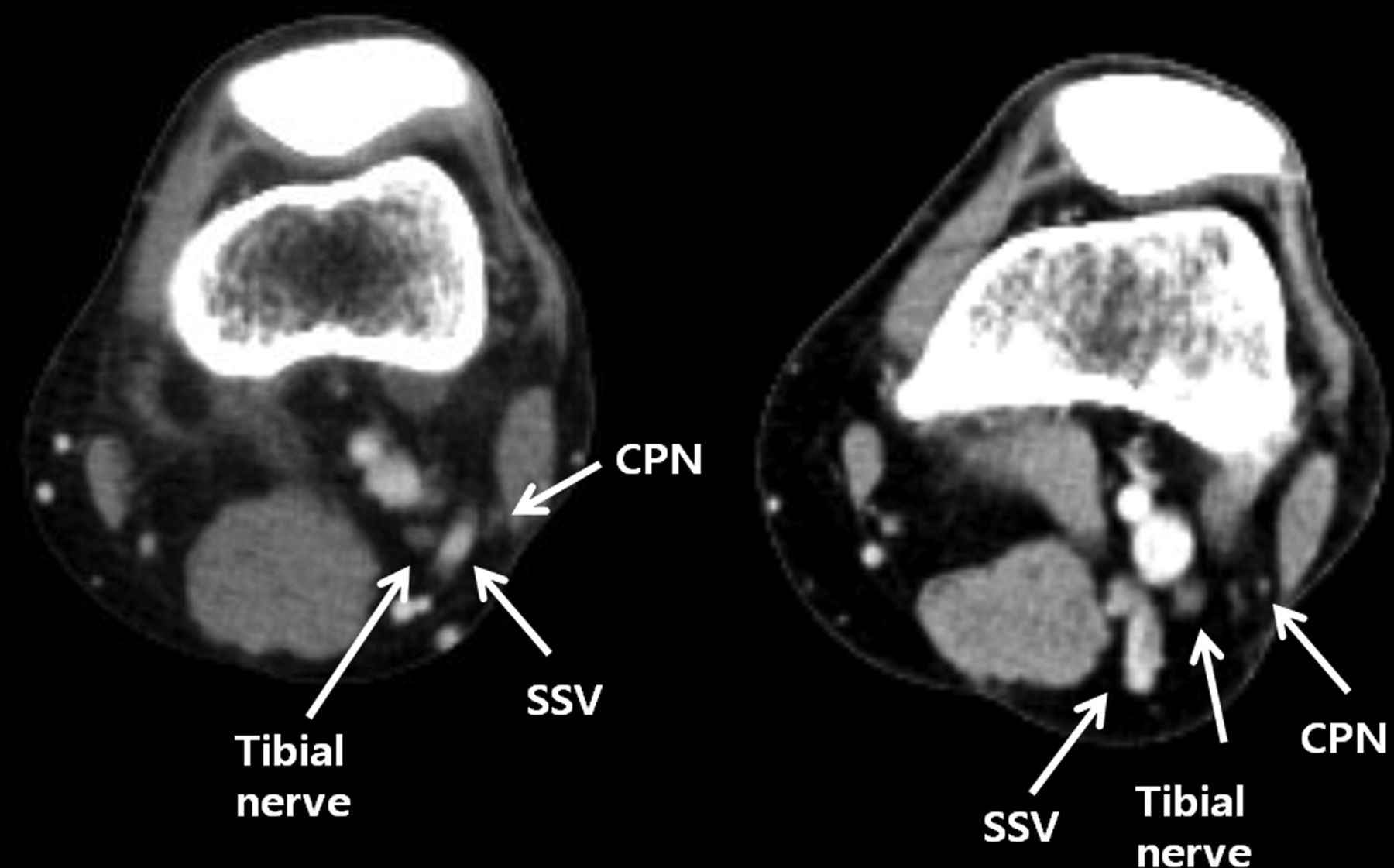
Localization of nerves in the popliteal fossa. Tibial nerve and common peroneal nerve (CPN) are marked in the axial view of computed tomography venography images. SSV, small saphenous vein
Clinical follow-up and adverse events
Within two weeks after surgery, patients were examined in the outpatient clinic and routine postoperative DUS was performed during 4–6 weeks after surgery. No residual reflux at SPJ was found. During six months follow-up, two transient sural nerve neuralgia were resolved spontaneously. Seven patients complained residual reticular vein or telangiectasia, and two of them were treated with sclerotherapy. No recurrence of VV was noted. No renal dysfunction or severe allergic reaction was developed in this series.
Discussion
As the public needs for proper treatment of VVs are increasing, the knowledge about the anatomy and haemodynamic of the venous system is rapidly increasing. The standard treatment for VV due to GSV insufficiency is high ligation of the saphenofemoral junction and stripping, which gives the best long-term results in some randomized trials. 10
But for SSV insufficiency, it has been reported that SSV surgery is more challenging due to higher recurrence and complication rates than GSV surgery. Lin et al. 11 reported that SSV with reflux is more than twice as difficult to surgically correct as a GSV with reflux. The main reason for that is the presence of many anatomic variations in SSV anatomy and close proximity of the vein with adjacent nerves in the somewhat crowded popliteal fossa.
The majority of surgeons did not perform formal dissection of the SPJ, presumably because of their fear of nerve damage, but followed the SSV down and ligated it a distance from the SPJ they judged safe. This could be one cause of the high rates of recurrence following SSV surgery. 12 Rashid et al. 13 analysed the outcome of 59 operations for SSV varicose veins and showed that there was a failure to identify and ligate the SPJ in 13 (22%) patients, despite preoperative duplex marking.
Nerve damage during varicose surgery is a major complication and the commonest cause of litigation following VV surgery against phlebologists. 14,15 Hence, accurate anatomic knowledge about the VV and neural topography is necessary to prevent this complication.
Duplex US imaging is the gold standard investigation for VVs and most surgeons have recommended that duplex imaging should be used routinely for SSVs, because of the variability of anatomy at the SPJ. 3,16–18 But duplex ultrasonography (USG) has limitations such as operator-dependent variable results, a time-consuming procedure, possible omission of perforators in unusual locations and a difficulty in the evaluation of pelvic vessels.
Uhl and Gillot 19 and Uhl et al. 20 reported that CTV with 3D reconstruction is a new promising adjunctive tool to assess recurrent or complex varicose networks in addition to duplex USG, which is mandatory for haemodynamics. In addition, a complete mapping of the venous network, providing anatomical as well as haemodynamical data, is crucial for making decisions and surgical achievement.
We reported previously that CTV could provide an excellent road map for VV surgery without significant complications. It cannot replace DUS, but can provide additional powerful 3D images. 4 In this study, we intended to identify the variable surgical anatomy by CTV preoperatively, which was useful for preoperative planning and preventing adverse events during operation in patients with SSV reflux. So we focused our assessment on the location of SPJ, SPJ morphology and the relationship between SSV and GNV and neural topography which are important for correct removal of reflux mechanism and prevention of complication.
Elsewhere, new international nomenclature and classification systems for the SPJ were reported. 21–23 In a recent autopsy study, SSV anatomic variations were reported among 83 limbs in 51 cadavers. 8 The neural topography at the origin of the gastrocnemius muscle showed common peroneal nerves located lateral to SSV in 81 (97.59%) limbs and tibial nerves in 53 (63.86%) limbs. That result was similar to that in our study identified in 3D-CTV.
TE was about 84% in Schweighofer's data, but 61.7% in our data. This disparity may be due to the resolution of CTV. But it may not be important in regarding the management of patients, because these small TEs may not have haemodynamical impact on varicosities. When we consider the autopsy data as the standard anatomic variation, our data from CTV showed comparable similarity and could be used as a reliable preoperative examination. In comparison with Schweighofer's autopsy study, the power of this study is that the exact anatomy of the individual patient can be evaluated before surgery, so the surgery can be performed with full knowledge of the patient-specific anatomy and haemodynamics.
CTV has some limitations. Sural nerve location could not be evaluated by CTV because of the small diameter of the nerve and many variations of the nerve division. In this study, transient sural nerve neuralgia developed in two patients and residual varicosity in seven patients among 103 patients in six months after surgery. This promising result might owe to the thorough preoperative CTV examination. Possible disadvantages of CTV such as renal dysfunction, allergic reaction to radiocontrast, radiation injury and additional cost can be a problem. But careful patient selection and meticulous protocol can minimize these complications.
This present study has limitations. There is no control group who were treated without the aid of 3D-CTV image. However, there was no residual SPJ reflux at routine postoperative DUS at 4–6 weeks after surgery in our series. Comparing with other studies, Rashid et al. 13 reported 22% of incompetent SPJ completely missed during surgery with preoperative duplex localization. O'Hare et al. 24 reported 10% residual incompetence at six weeks after surgery. Although there is no statistical comparison, we think these differences are meaningful.
Conclusion
The thorough preoperative evaluation of SSV anatomical variations by 3D-CTV was feasible and it may contribute to minimizing complications and recurrence after VV surgery with SSV reflux.