
Abstract
Different internal jugular vein (IJV) abnormalities can be found in patients with multiple sclerosis (MS): stenoses, complete occlusion, distortions and intraluminal structures, such as membranes, webs and inverted valves. IJV duplication is a very rare phenomenon. We report a case of right IJV duplication as an incidental finding during IJV morphological and haemodynamic assessment in a patient with MS. A 55-year-old female patient was admitted to our Institute for IJV and vertebral veins morphological and haemodynamic assessment. During the last seven years she had been treated for MS. Colour Doppler ultrasonography in our patient did not reveal IJV or vertebral veins stenoses or abnormal valves, but instead right IJV duplication. This finding was confirmed using multislice computed tomography angiography and by selective phlebography. In conclusion, to our knowledge, a case of IJV duplication in a patient with MS has not been described yet. This further venous malformation can be assessed by the means of Doppler ultrasounds.
Introduction
As an addition to autoimmune theory, vascular theory supports the hypothesis that chronically impaired venous drainage from the brain can be one of the aetiological factors in multiple sclerosis (MS) pathogenesis. 1,2 The condition known as chronic cerebrospinal venous insuffiency (CCSVI) is characterized by internal jugular (IJV), vertebral and/or azygos vein stenoses and insufficient cerebral vein drainage. 1,2 By ultrasound evaluation of extracranial venous malformations, Zamboni et al. 1,2 re-awakened vascular theory in MS pathogenesis describing strong association between IJV stenosis, CCSVI and MS and showed that percutaneous angioplasty of narrowed IJV significantly improved validated outcome in some affected patients.
IJV duplication is a very rare phenomenon. The exact incidence is not known but reviewed literature describes only a few cases. 3,4 We report a case of right IJV duplication as an incidental finding during IJV morphological and haemodynamic assessment in a patient with MS.
Case report
A 55-year-old female patient was admitted to our institute for IJV and vertebral veins morphological and haemodynamic assessment. During the last seven years she had been treated for MS. The disease clinical form presentation was relapsing–remitting type, last two years in remission. According to Zamboni et al.,
1,2
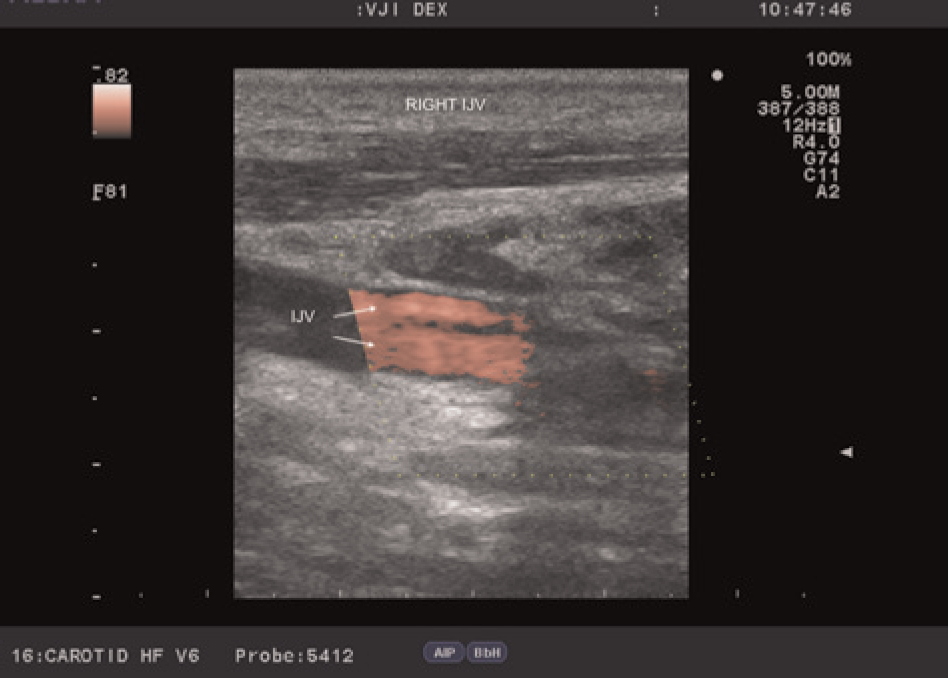
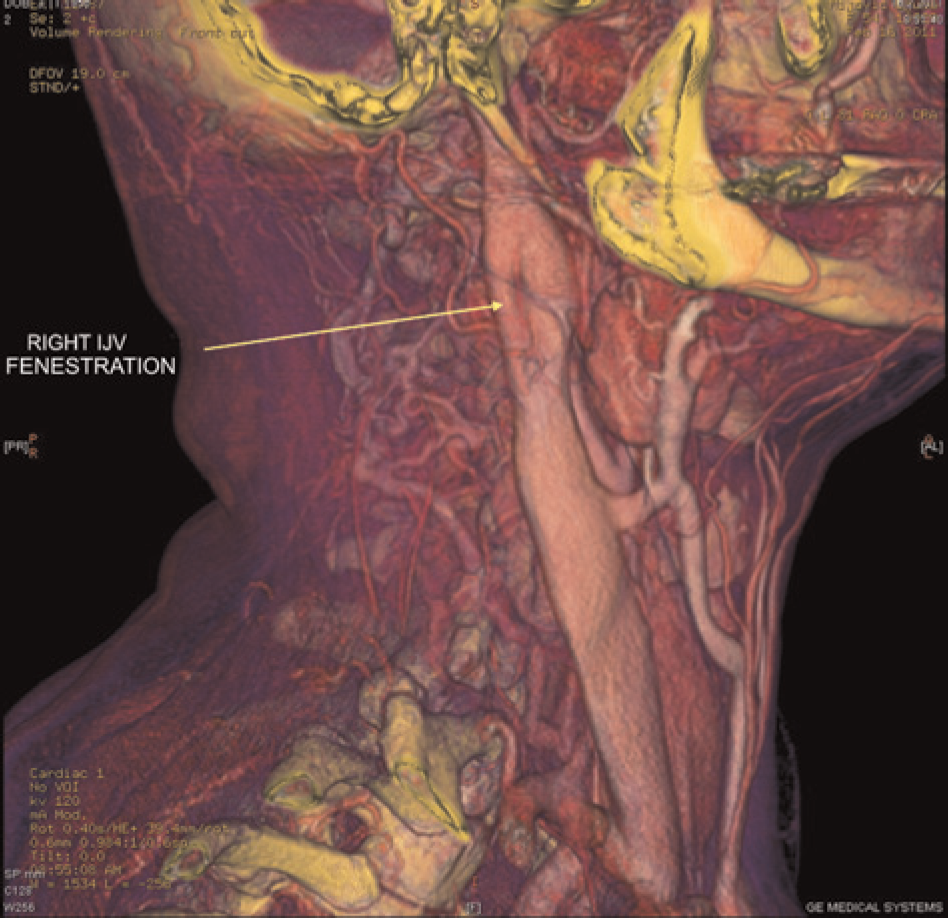
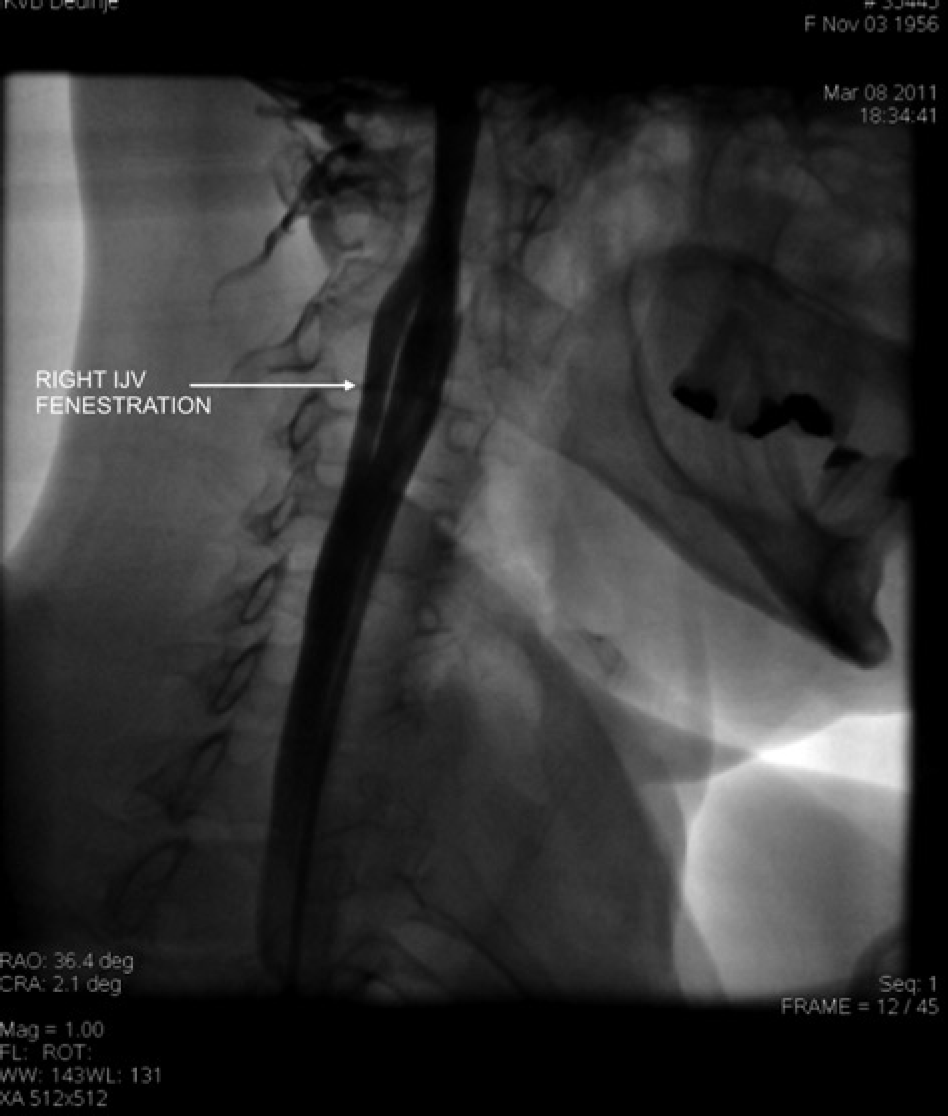
different IJV abnormalities can be seen in patients with MS, which can be easily assessed by colour Doppler ultrasonography of IJV and vertebral veins. Colour Doppler ultrasonography in our patient did not reveal IJV or vertebral veins stenosis or abnormal valves, but instead right IJV duplication (Figures 1 and 2). This finding was confirmed using multislice computed tomography angiography (Figure 3) and by selective phlebography (Figure 4).
Colour Doppler ultrasonography showing right internal jugular (IJV) vein duplication Colour Doppler ultrasonography. Arrows indicate right internal jugular vein double lumen Multislice computed tomography angiography shows right internal jugular vein (IJV) duplication Selective phlebography showing right internal jugular vein (IJV) duplication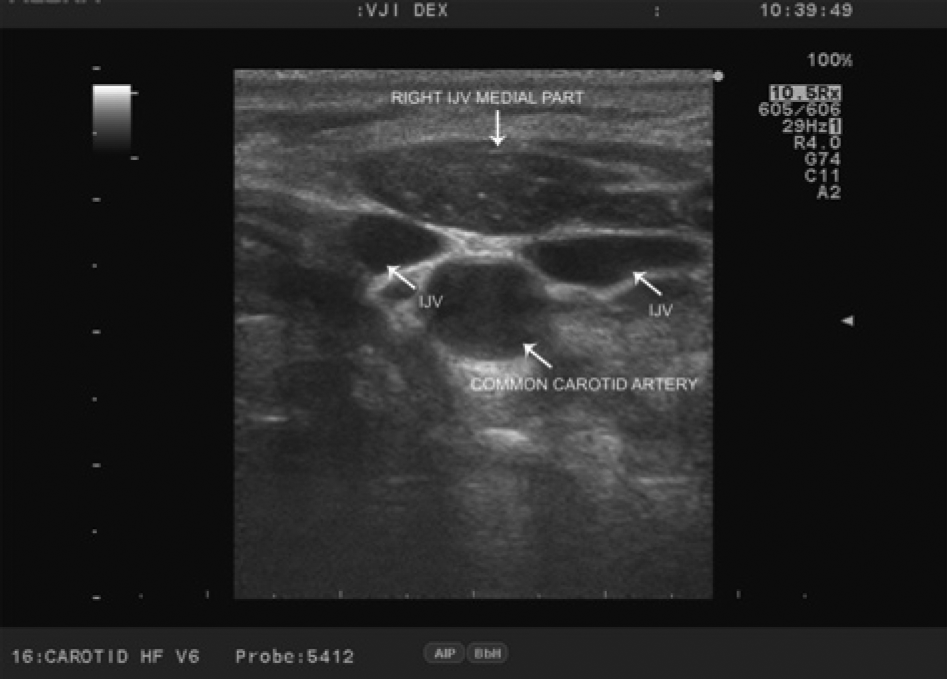
Discussion
Different IJV abnormalities can be found in patients with MS and CCSVI: stenoses, complete occlusion, distortions and intraluminal structures such as membranes, webs and inverted valves. 1,2 CCSVI extracerebral venous morphology and haemodynamics characteristics can be easily assessed in patients with MS by colour Doppler sonography with changes in posture.
In a recent study (publication pending in Phlebology), we examined 64 patients with clinically proven MS as well as 37 healthy individuals. We assessed IJV morphological and haemodynamic abnormalities by the means of high-resolution B-mode ultrasounds performed with the patients in the sitting and supine positions. Although no statistically significant differences in the frequency of stenosing lesion was observed between patients with MS and healthy controls, by adding haemodynamic Doppler information in the IJV, venous outflow was significantly different in 42% of MS patients showing flow abnormalities (27/64), as compared with 8.1% of the controls (3/37), P < 0.001. IJV duplication, seen in our case, was an incidental finding.
According to Lee et al., 5 the jugular vein malformations seen in patients with CCSVI are recognized as ‘truncular’ venous malformations in their 2009 Consensus document. High IJV duplication, as a form of jugular double channel seen in our patient with MS, could be classified as venous truncular malformation.
Incidence of IJV duplication is unclear, but some anatomists reported an incidence of 4/1000 patients during neck dissection. 6 The IJV duplication is usually described in association with phlebectasia, which was not observed in our case.
There are three theories explaining pathogenesis of the IJV duplication. 6 Vascular hypothesis suggests that the IJV duplication can be a result of the secondary venous ring appearance at a lower level. 6 When considering embryological background, it is known that right anterior cardinal (precardinal) vein proximal to the right brachiocephalic vein forms superior vena cava with common cardinal, while the distal segment of precardinal vein becomes right IJV. 7 Taking into account truncular malformations origin, malalignment and incomplete fusion on behalf of the primordial cardinal veins may explain the IJV duplication seen in our case. On the other hand, double jugular channel could also occur due to IJV vertical septation. 8,9
The neural hypothesis supports the view of the spinal accessory nerve relationship to the transverse process of the atlas alternation and disruption in the IJV development. 6 On the other hand, the bony hypothesis suggests that ossification of the bony bridges of the jugular foramen may be the cause of IJV duplication. 6
To our knowledge, a case of IJV duplication in a patient with MS has not been described yet.
Conclusion
Whenever colour Doppler ultrasonography is performed for the IJV morphological and haemodynamic assessment in patients with MS, attention should be paid to the possible appearance of the various venous abnormalities including IJV duplication. The significance of this finding in MS patients is yet to be determined.
Footnotes
Acknowledgement
This manuscript was supported by grant no. 41002 of the Serbian Ministry of Science and Technological Development.